
Abstract
Students in the health professions need to build skills for interprofessional practice (Doll et al., 2013). Occupational therapy practitioners often are a part of an interprofessional team consisting of other health care professionals. These teams can be found in a variety of settings, including acute inpatient rehabilitation and home health care.
Interprofessional education (IPE) has been proposed as a method to foster development of collaborative teams who practice across disciplines (Gilbert et al., 2010). According to the World Health Organization (WHO; 2010), IPE occurs when two or more professionals learn about, from, and with each other to enable effective collaboration and improve health outcomes. The Interprofessional Education Collaborative Expert Panel (2011) identified four core domains of competencies: values and ethics for interprofessional practice, roles and responsibilities, interprofessional communication, and teamwork.
IPE is an effective method to increase interprofessional communication skills and patient-centered care (Thistlethwaite et al., 2013). IPE can lead to increased interprofessional practice (IPP) that influences the culture of safety in health care settings, which in turn drives performance on measures of employment satisfaction and patient experience. Working in interdisciplinary teams was identified as a competency deemed essential for the education of health care professionals (Institute of Medicine, 2003). Thus, IPE should begin during didactic coursework of health care programs (Alotaibi et al., 2015).
With the increased importance of IPE, programmatic accrediting bodies are beginning to integrate standards regarding IPE. For both occupational therapy doctoral and master’s degree programs, the Accreditation Council for Occupational Therapy Education (ACOTE®) Standard B.5.21 states that students must be able to effectively communicate, coordinate, and work interprofessionally with those who provide services to individuals, organizations, and/or populations to clarify each member’s responsibility in executing components of an intervention plan (American Occupational Therapy Association [AOTA], 2012). For occupational therapy doctoral programs, ACOTE Standard B.4.8 states that students must be able to interpret the evaluation data in relation to accepted terminology of the profession, relevant theoretical frameworks, and interdisciplinary knowledge (AOTA, 2012). In addition, accrediting bodies in the United States, such as ACOTE, are encouraging academic institutions to adopt IPE programming (Schreiber & Goreczny, 2013).
Faculty beliefs regarding IPE have been previously examined (Curran et al., 2007). Successful integration of IPE into any academic program requires support from program faculty. A study of respiratory therapy faculty found that educators recognized IPE as an important component of education but were challenged in incorporating it into their curriculum (Vernon et al., 2017). No literature was found that investigated occupational therapy faculty perceptions of IPE.
The main purpose of this study was to identify occupational therapy faculty beliefs and perceptions of IPE. Between-groups assessments of ranking of IPE competencies and the likelihood of offering IPE programs affiliated with an academic health care center (AHC) and programs not affiliated with an AHC were examined.
Method
Qualtrics (Provo, UT) was used to develop a 43-question survey based on a previously published questionnaire that assessed perception of IPE among faculty in health professional academic programs (Curran et al., 2007). The target population consisted of occupational therapy faculty members at ACOTE-accredited programs. Accredited programs were identified online through the use of AOTA's (2018a, 2018b) directories of such programs. We then visited each program’s respective web page to retrieve faculty email addresses. Our survey was sent to 1,488 faculty.
The survey included four sections:
Section 1 collected respondent demographic characteristics, such as age of program, degree awarded, number of students, and type of institution.
Section 2A collected information regarding knowledge of IPE and the program’s inclusion of IPE in the curriculum. Agreement with the WHO (2010) definition of IPE was assessed, and ideas about the number of credit hours necessary for IPE instruction were examined. Faculty were asked to rank the importance of the four IPE competencies by ordering them from 1 (most important) to 4 (least important). Sections 2B and 2C were adapted from Curran et al. (2007). These sections were scales of beliefs about IPE (9 questions) and beliefs about interprofessional learning (12 questions).
Sections 3A and 3B collected information regarding knowledge of IPP and beliefs and perceptions about interprofessional collaborative practice in health care. Sections 2B, 2C, and 3B used a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree).
Section 4 allowed respondents to answer open-ended questions on barriers and opportunities for implementing IPE in their programs.
Data Collection and Analysis
We received approval from the Augusta University institutional review board before soliciting emails were sent. A pilot email was sent to a random 50 email addresses to assess the functionality of Qualtrics. Afterward, the anonymous survey was distributed online to the remaining faculty. Two reminder emails were sent at 2 and 4 wk to faculty who had not yet completed the survey. The survey was closed after 6 wk. Statistical analysis was conducted using IBM SPSS Statistics (Version 24.0; IBM Corp., Armonk, NY).
Results
In total, 1,488 emails were sent, 52 were returned as undeliverable, and 7 respondents reported not meeting the inclusion criteria because they were retired or not hired directly within the occupational therapy department. Thirty-two percent (n = 456) took the survey. The response rate was better than those of other faculty surveys that used an emailed link, which were reported to be about 20% (e.g., Kaplowitz et al., 2004). Median time to complete the survey was 9 min, 30 s. More than half of the respondents (56.3%; n = 247) reported being part of a program that has been established for more than 25 years, and 40.1% (n = 176) reported being part of a program that had been established for 25 yr or less. More than three-quarters of respondents (76.3%; n = 335) reported being faculty at a nonprofit institution. More than half (66.5%; n = 292) identified themselves as faculty at a program with more than 90 students. A total of 45.1% (n = 198) reported that they had an AHC on campus, and 54.9% (n = 241) reported that they did not. Table 1 summarizes the demographic characteristics of the respondents’ occupational therapy programs.
Respondent Demographics
Note. — = not applicable.
All but 1 respondent agreed with the WHO (2010) definition of IPE; 71.6% (n = 312) reported regularly including IPE in their curriculum, and 77.2% (n = 328) wanted to see a greater emphasis on IPE in their curriculum. Case studies were the most popular method of IPE instruction, with 71.5% (n = 218) including it most of the time or always. Even with the desire for a greater emphasis on IPE, 40.4% (n = 176) of respondents reported not knowing how many credits programs should require to competently teach IPE.
Faculty who reported that their campus was part of an AHC (75.1%; n = 197) were more likely to include IPE in their curriculum than those who reported that their campus was not part of an AHC (68.6%; n = 148). Of faculty with an AHC on campus, 85% (n = 168) reported that their institution offered at least five academic health care programs. Of faculty without an AHC on campus, only 43% (n = 103) reported that their institution offered five or more academic health care programs (Figure 1). A χ2 test indicated a statistical difference in the number of academic program offerings between occupational therapy programs that consider themselves a part of an AHC versus those that do not (χ2 = 81.5, p < .01). In addition, 71.2% (n = 302) of respondents reported that physical therapy was the top program with which occupational therapy programs collaborated, and 59.2% (n = 251) stated that nursing was the second most popular.
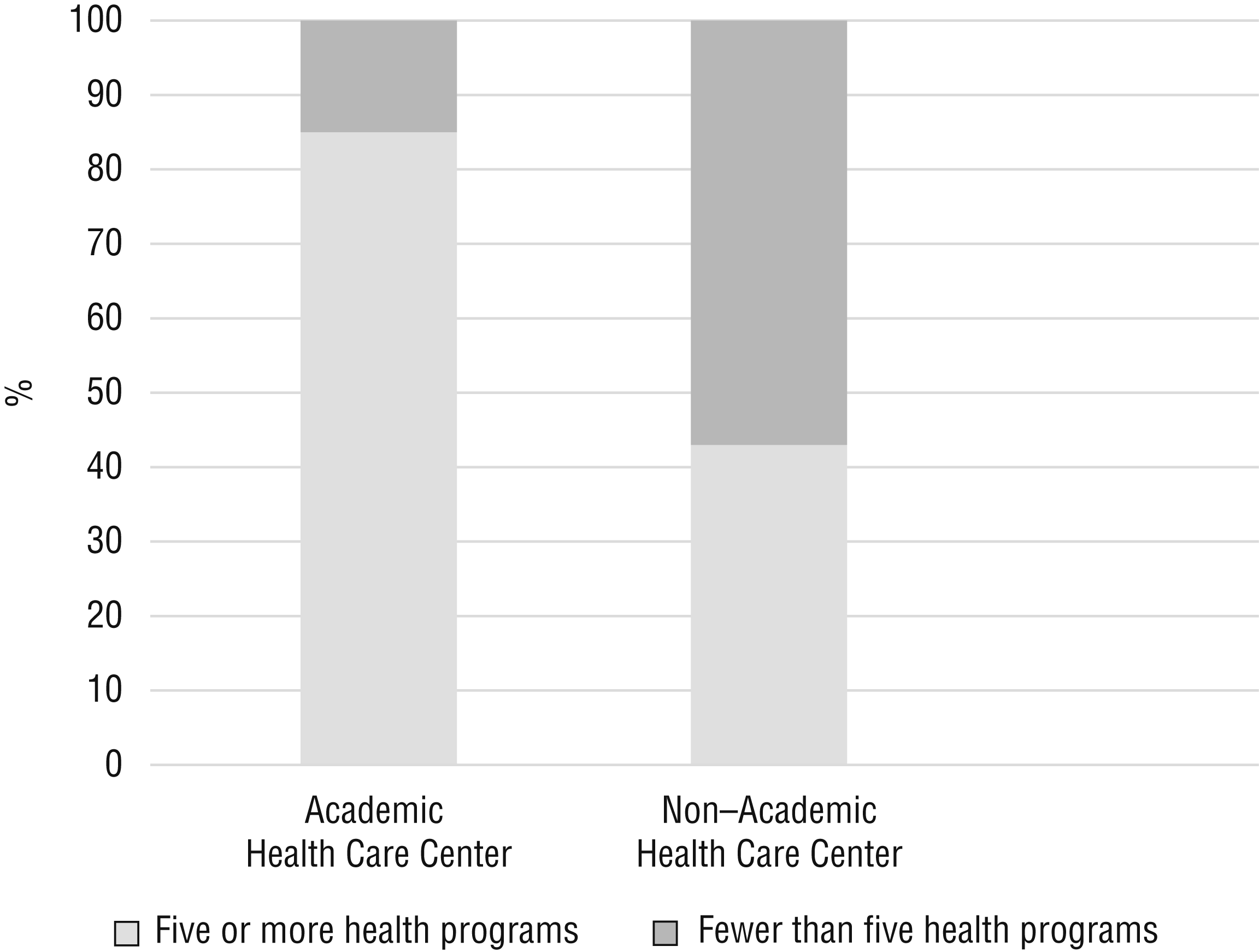
Academic health program offerings.
Faculty responses largely supported the need for IPE: The majority (97.9%; n = 410) strongly agreed (n = 289) or agreed (n = 121) that patients would ultimately benefit if health care students worked together to solve patient problems. Even though faculty generally supported the need for IPE, 69.2% (n = 286) of respondents were indifferent or did not agree that current curriculum requirements could be removed to make room for IPE. More than half of survey respondents (54.4%; n = 223) strongly agreed (n = 76) or agreed (n = 147) that ACOTE should mandate IPE in the occupational therapy curriculum.
Faculty were asked to rank the importance of the four IPE competencies (Figure 2). Of the 406 who ranked the competencies, 37.7% (n = 153) ranked ethics as the most important, and 38.0% (n = 154) ranked communication as the second most important. A Mann–Whitney U test revealed no significance in ranking IPE competencies in regard to importance on the basis of having an AHC on campus or not. IPE competency rankings were not significantly different between programs that did and did not have an AHC on campus.
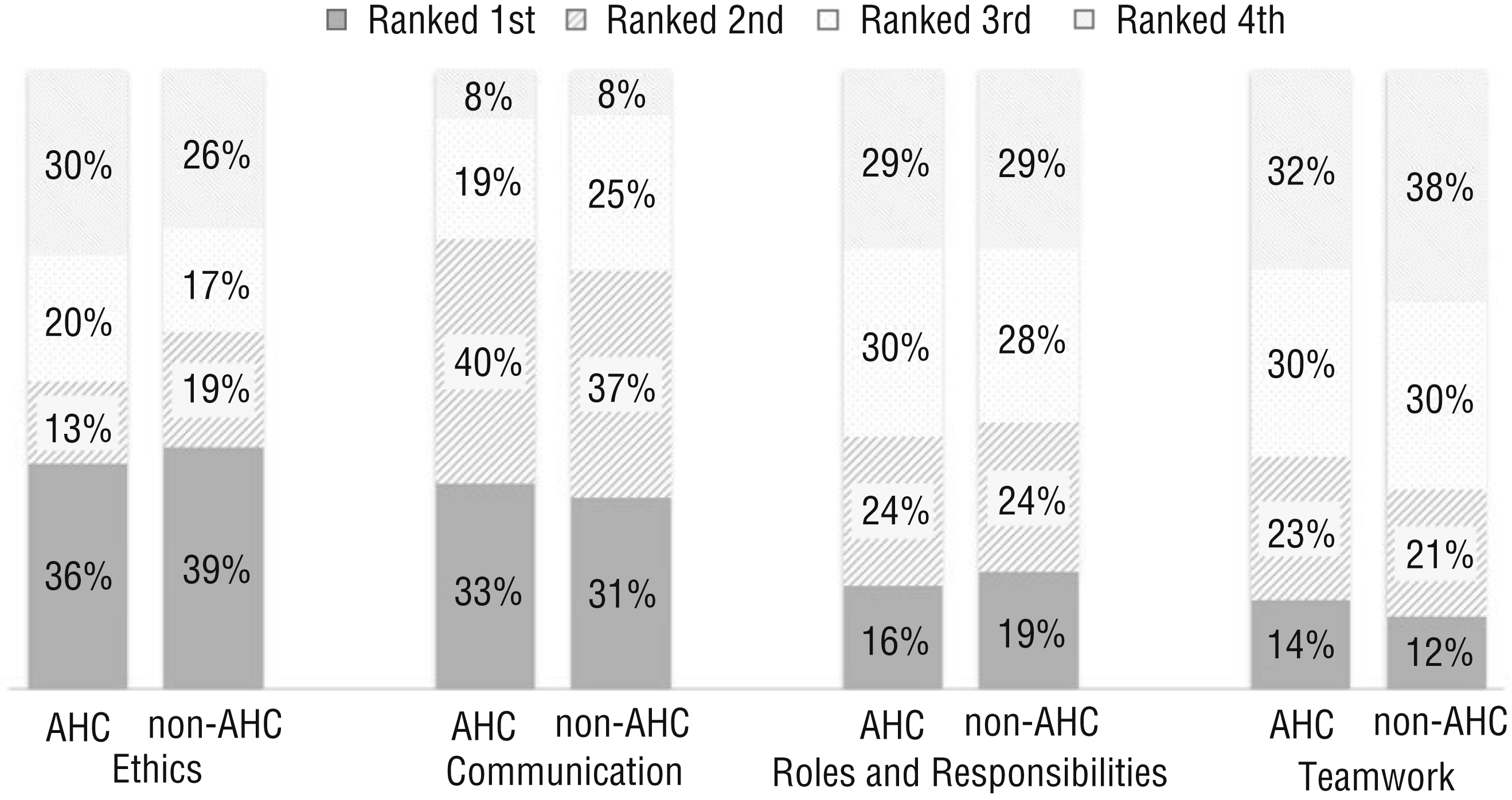
Ranking of interprofessional education core competencies from 406 survey respondents.
Of the faculty who responded, 78.3% (n = 314) reported that clients receiving interprofessional care were more likely to be treated as whole persons, and 90.1% (n = 360) agreed or strongly agreed that the give and take among team members helped them make better client care decisions. In addition, 62.5% (n = 248) of respondents reported that working in an interprofessional environment kept most health professionals enthusiastic and interested in their jobs.
Many respondents identified opportunities for implementing IPE within their program. Of the 309 respondents, 39.8% (n = 129) mentioned that IPE enhanced or improved the learning environment, and 31.7% (n = 98) believed that IPE improved understanding of the role of occupational therapists in health care teams. Even though respondents mentioned many opportunities, they also reported barriers to implementing IPE. Some of the most common responses were not having enough time (38.9%; n = 129) and lack of faculty (33.7%; n = 112).
Discussion
The main objective of this study was to evaluate the beliefs and perceived importance of IPE among occupational therapy faculty. Faculty responses revealed supportive beliefs regarding IPE and a positive perception of IPE’s relevance within the occupational therapy curriculum. Even with positive beliefs and perceptions, more than half of respondents did not have an opinion on the number of credit hours required to teach IPE. This finding highlights a possible lack of knowledge of IPE and methods to better incorporate IPE into their curriculum.
According to our data, faculty who are part of an AHC have the opportunity to collaborate with a larger variety of professional programs than faculty who are not part of an AHC. Interestingly, all faculty surveyed had similar views on which competencies are the most important in IPP. This suggests that faculty generally agree on the most important competencies for IPE. Of the four competencies, ethics and communication are the most difficult to assess and were ranked as the two most important. Roles and responsibilities and teamwork, which tend to be more procedural and are more measurable, ranked last.
Health care workers have a high rate of burnout, which is associated with elevated stress levels on the job (Harry, 2014). More than half of respondents, 61.8% (n = 248), agreed that working in an interprofessional environment keeps most health professionals enthusiastic and interested in their jobs, which may reduce burnout in occupational therapy practitioners. Our findings suggest that employers willing to foster interprofessional working environments may see economic benefit as a result of the reduction of practitioner turnover and improved employee satisfaction.
Limitations
Research involving surveys has limitations because of the nature of self-report. All of the results are opinions of faculty members at ACOTE-accredited programs. The survey did not distinguish whether the respondents were chairs, program directors, or faculty. Chairs and program directors may have perspectives that differ from those of faculty. Larger programs with cohorts totaling greater than 100 students have more faculty, which may have led to oversampling of the larger programs. Although our survey instrument was adapted from validated questionnaires, an approach that is consistent with previous methodology (Curran et al., 2007), we realize that our survey may still have validity and reliability concerns.
Implications for Occupational Therapy Education
Occupational therapy faculty are in an ideal position to influence future practitioners to partake in a more IPP. The AOTA (2010) occupational therapy Scope of Practice includes providing services to persons, groups, and populations from all ages and various settings. These services can be optimized through an interprofessional team. Actions need to be taken to allow occupational therapy programs to further support the ability for curricula to offer IPE experiences. Therefore, occupational therapy faculty should
Explore opportunities to offer IPE experiences to their students;
Collaborate with administrators in supporting college- and university-wide IPE;
Assess student perceptions of already-implemented IPE; and
Assess perceptions of recent graduates of occupational therapy programs that offer IPE.
Conclusion
Occupational therapy faculty support the need for IPE. Limitations in time and number of faculty were reported as barriers to increasing offerings. Even though faculty support IPE, they do not know how many credit hours are required to teach IPE, suggesting the possibility of a lack of knowledge about IPE instructional methods. Occupational therapy departments in AHCs have opportunities to collaborate with a larger number of academic programs. There is consistency in the ranking of IPE competencies across occupational therapy programs. As IPE continues to be increasingly common in health program accreditation standards, occupational therapy faculty need to continue to seek opportunities to incorporate IPE in current curricula.