
Abstract
Between 10% and 25% of older adults experience frailty in later life (Bandeen-Roche et al., 2006; Fried et al., 2001), which reduces their ability to respond to and recover from everyday challenges encountered as part of aging. Exactly how best to define and operationalize frailty remains up for debate (Bergman et al., 2007). There is agreement within the broader scientific community, however, that regardless of the underlying mechanisms, frailty is multidimensional, characterized by the presence of multiple risk factors or deficits, and that it signifies a loss of resilience across one or more domains of functioning (e.g., physical, psychological, or social) that results in an increased vulnerability to stressors (Bergman et al., 2007; Resnick, 2014; Zaslavsky et al., 2013). For example, because of a loss of resilience (e.g., loss of social relationships or reduced activity tolerance), a relatively minor physical change (e.g., acute illness) has the potential to trigger a cascade of negative events for a frail older adult, including disability in basic and instrumental activities of daily living, institutionalization, and mortality (Bandeen-Roche et al., 2006; Fried et al., 2001; Provencher et al., 2012).
Researchers also agree that frailty is a clinically useful concept. The concept of frailty has increasingly been adopted in aging research (e.g., see Afilalo et al., 2009) because it can be applied across diagnostic categories to define people who are at risk for decline or adverse events and who may subsequently benefit from interventions to ameliorate such effects (Bergman et al., 2007). Several validated frailty scales have been developed to aid researchers and clinicians in screening and identifying frail older adults (e.g., Fried Frailty Criteria, Frailty Index; Dent et al., 2016).
The ability to screen at-risk frail and slightly frail (i.e., prefrail) people is especially important because the progression to frailty is not inevitable, and evidence suggests that it is possible to slow or reverse its development (Gill et al., 2006). Occupational therapists are uniquely suited to address frailty in older adulthood by assessing at-risk people and intervening to bolster existing reserves, as well as compensating for reductions in resilience (e.g., losses in strength, activity tolerance, or social engagement) and preventing losses of resilience that contribute to the development of frailty (Provencher et al., 2012). Moreover, occupational therapy intervention delivered in hospital, home, and community settings has been shown to improve functional ability, social functioning, and quality of life (Clark et al., 1997; Murphy et al., 2010; Steultjens et al., 2004) among older adults. Because occupational therapy intervention has been successful for other older adult populations with problems that also occur in the context of frailty (e.g., weakness and social isolation), occupational therapy intervention could have similar positive results for frail older adults. To effectively contribute to efforts to attenuate the effects of frailty, however, occupational therapy practitioners need to use evidence-based practices.
The purpose of this scoping review was to examine the existing evidence related to the use of occupational therapy intervention to improve outcomes among frail community-dwelling older adults. Specifically, we sought to (1) characterize how frailty was defined and operationalized in occupational therapy interventions delivered to frail older adults, (2) characterize and describe the types of occupational therapy treatments delivered as part of those studies and the treatment dose used, and (3) describe the primary outcomes of interest.
Method
We used a scoping review method (Arksey & O’Malley, 2005; Levac et al., 2010) to systematically search the literature. Scoping reviews are a good methodological choice when the goal of the study is to examine the nature and extent of a body of research, identify gaps in the literature, or inform decisions about whether to proceed with a systematic review. The scoping review included the following five steps: (1) identifying the research question; (2) identifying relevant studies; (3) selecting studies that met the inclusion criteria; (4) charting the data; and (5) collating, summarizing, and reporting the results.
Search Strategy and Study Selection
We performed a scoping review of the published, English-language peer-reviewed publications in the Cochrane Database of Systematic Reviews, CINAHL Complete, PsycINFO, Scopus, PubMed Central, MEDLINE, and the Web of Science. Because we anticipated that the number of occupational therapy–specific research articles published on frailty would be relatively small, we included all studies published between January 1996 and January 2017 to maximize the possible number of studies that could contribute data for the review. Before commencing the review, our research team consulted with a medical librarian to identify candidate databases and develop a list of search terms that best fit the research question and that were commonly used in each database.
The search stream was entered exactly as follows in the search field for each database: “[Occupational therapy OR activities of daily living OR rehabilitation] AND [Frail OR frail elderly OR prefrail OR vulnerable OR frailty OR physical frailty] AND [Intervention OR trial OR program OR randomized control trial OR feasibility OR treatment OR evaluation OR prospective studies].” We intended to apply the search stream to the title, abstract, and keyword field in each database. However, our selected databases offered different field options, and so there was slight variation in the fields used across each database. For the Scopus, PubMed Central, and Web of Science databases, the search stream was applied to the “title/abstract” fields. In the Cochrane Database of Systematic Reviews, the search stream was applied to the “title/abstract/keyword” fields. CINAHL, PsycINFO, and MEDLINE do not use a combined “title/abstract” or “title/abstract/keyword” field search, so we applied the search stream to the “word in subject heading” field.
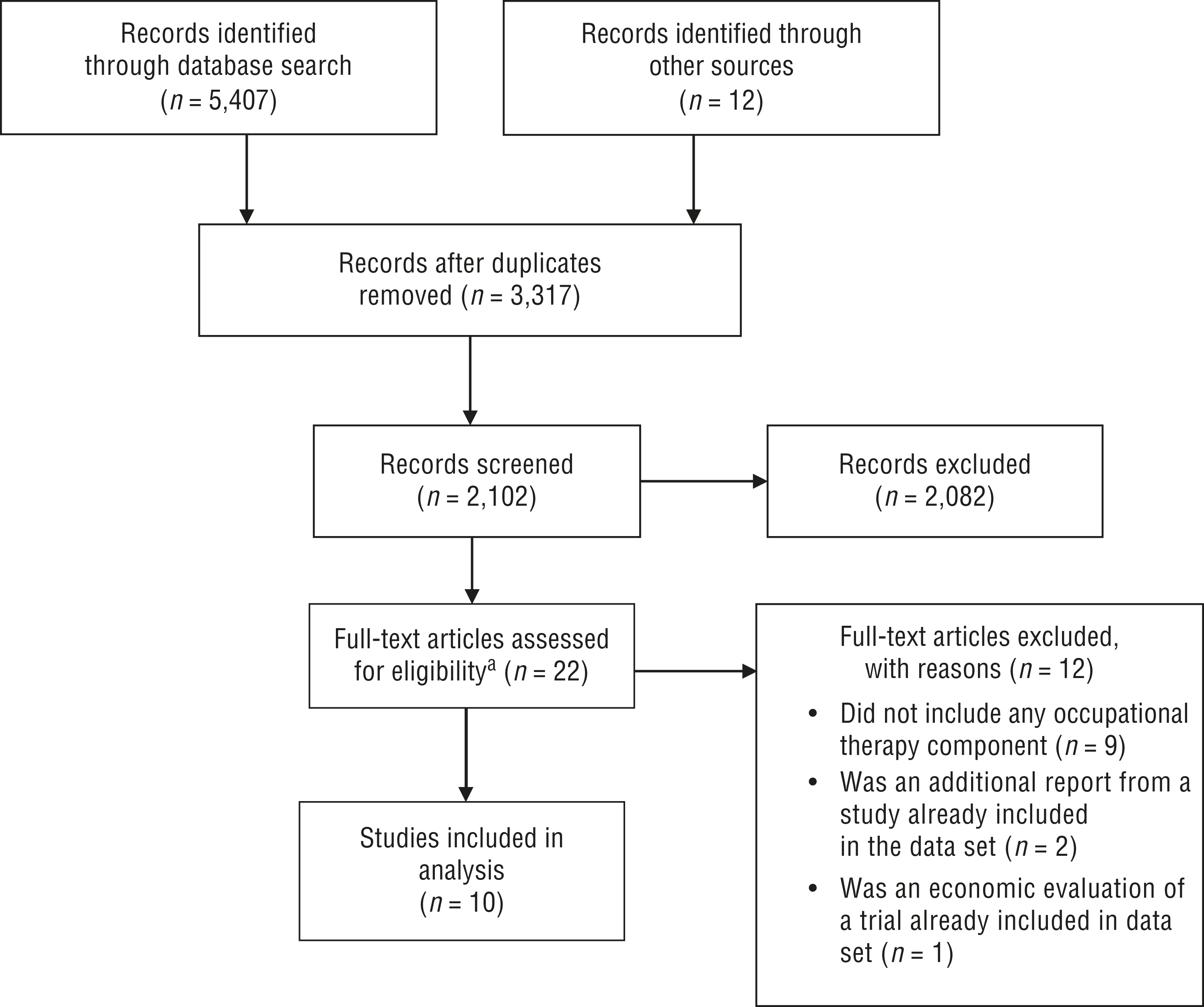
The search resulted in 5,419 articles. A total of 3,317 duplicates were removed. We independently performed the initial screening of the remaining 2,102 titles and abstracts on the basis of specific inclusion criteria (outlined next), resulting in the exclusion of an additional 2,082 articles. During the screening stage, we resolved 11 conflicts over whether to include articles by discussing the article in relation to the inclusion and exclusion criteria until we reached consensus.
Because one objective of the review was to examine how frailty was defined and conceptualized in the occupational therapy intervention literature, we did not use a prespecified operationalization of frailty to include or exclude articles, with one exception. We excluded articles that used only a diagnostic label (e.g., stroke, Parkinson’s disease, multiple sclerosis) to infer frailty without providing any other explanation or definition. We defined community-dwelling older adults as people age 55 yr or older who resided in the community either in their own homes or in assisted living facilities. To be included in the review, a minimum of 51% of a study’s sample had to be age 55 yr or older. We defined occupational therapy interventions as those that included intervention content that was delivered by an occupational therapist either alone or in combination with other disciplines or treatments. We excluded studies if they were not intervention studies, did not include an occupational therapy component, were not delivered to a majority older adult population, or were not delivered to community-dwelling older adults.
We all participated in fully reviewing the remaining 20 articles, included reviewing the reference lists. The reference review process led to the inclusion of 2 additional studies for a total of 22 articles. When disagreements arose regarding the inclusion of certain studies, we discussed them until a consensus was reached. For each study meeting the inclusion criteria, the data were extracted and entered into a table (Table 1). In cases in which multiple articles referenced the same study, we counted those studies as duplicates. We did, however, include results from additional publications in the “Primary Results” column of Table 1. After full review, we ultimately removed 12 studies because either they did not include any occupational therapy–related treatment or they were additional reports (e.g., they reported the long-term outcomes or economic evaluation) of studies already included in the data set (Figure 1).
Studies of Occupational Therapy Intervention Among Frail, Community-Dwelling Older Adults (N = 10)
Note. ADLs = activities of daily living; BADLs = basic activities of daily living; HRQOL = health-related quality of life; IADLs = instrumental activities of daily living; LGST = life goal-setting technique; MMSE = Mini-Mental Status Examination; OT = occupational therapy or occupational therapist; PT = physical therapist; QOL = quality of life; RCT = randomized controlled trial; RN = registered nurse; SPCP = standard preventive care program; SW = social worker.
We extracted data using a data extraction grid designed for the purposes of the study and based on McMaster University’s Critical Review Form for Quantitative Studies (Law et al., 1998). Data points extracted for analysis included (1) definition or operationalization of frailty, (2) the dose of the intervention, (3) the types of treatments delivered as part of the intervention, and (4) the outcome measures used as part of the intervention. When data elements were only described in general terms, we attempted to contact the study’s corresponding author to obtain further details (e.g., the content of any occupational therapy intervention delivered).
Results
Study and Participant Characteristics
The 10 studies included in this scoping review were published between 1999 and 2016. All studies included people age 65 yr or older, with 2 studies focusing on older adults age 70 yr or older and age 80 yr or older, respectively (Dahlin-Ivanoff et al., 2010; Metzelthin et al., 2013). Participant age ranged from 65 to 97 yr across the group of studies. The majority of participants were women of European descent. Only 2 studies were conducted in the United States; the remaining 8 studies were conducted in Finland (n = 1), Sweden (n = 2), the United Kingdom (n = 1), Belgium (n = 1), the Netherlands (n = 2), and Japan (n = 1). Six studies were two-arm, randomized controlled trials (RCTs; De Vriendt et al., 2016; Gitlin et al., 2006; Mann et al., 1999; Metzelthin et al., 2013; Ollonqvist et al., 2008; Stewart et al., 2005); 1 was a three-arm RCT (Dahlin-Ivanoff et al., 2010); 2 were nonrandomized multicondition trials (de Almeida Mello et al., 2016; Yuri et al., 2016); and the remaining study was a single-group, within-subject, repeated-measures design (Fisher et al., 2007). In the RCT studies, the most common comparison condition was usual care.
Operationalization of Frailty
The operationalization of frailty was inconsistent across studies. Ollonqvist et al. (2008) used government agency guidelines to determine frailty status, operationalizing it as eligibility to receive the Finnish government’s social care allowance for pensioners. Three studies used validated frailty measures either alone or in combination with other measures to identify frail participants (de Almeida Mello et al., 2016; Metzelthin et al., 2013; Yuri et al., 2016). For example, de Almeida Mello et al. (2016) screened participants for inclusion using the Edmonton Frailty Scale, the Katz Scale, or a diagnosis of dementia. One study used a combination of frailty indicators (e.g., weakness, exhaustion, fatigue) rather than a validated measure (Dahlin-Ivanoff et al., 2010). The remaining studies operationalized frailty as either the presence of disability in one or more daily activities (De Vriendt et al., 2016; Fisher et al., 2007; Gitlin et al., 2006) or as needing home services to remain independently living at home (Mann et al., 1999; Stewart et al., 2005).
Occupational Therapy Intervention Content and Dose
Four studies were categorized as occupational therapy dominant because they used occupational therapy alone or as the primary intervention (De Vriendt et al., 2016; Fisher et al., 2007; Gitlin et al., 2006; Mann et al., 1999). Six studies either embedded the occupational therapy intervention in a multidisciplinary approach (e.g., using occupational therapy in addition to other professional services; Dahlin-Ivanoff et al., 2010; Metzelthin et al., 2013; Ollonqvist et al., 2008) or included it as a separate treatment package that was evaluated against other treatment approaches (de Almeida Mello et al., 2016; Stewart et al., 2005; Yuri et al., 2016).
Across studies, the occupational therapy intervention included an evaluation and treatment plan. In 2 studies, the occupational therapist provided both standardized educational content in a group setting and individual assessments (Dahlin-Ivanoff et al., 2010; Ollonqvist et al., 2008). The primary foci of occupational therapy intervention across studies were recommendations and training in the use of adaptive devices or assistive technologies (6 studies), performance of self-care (6 studies), and recommendations for home modifications (5 studies). One study explicitly included a focus on productivity and leisure pursuits (De Vriendt et al., 2016). Treatment strategies varied across the studies, but most used a combination of education, skills training, recommendations for adaptive devices or home modifications, or referrals to other services (e.g., speech or physical therapy).
The dose of occupational therapy intervention content varied across the data set and was difficult to determine for the majority of studies. Authors often described the treatment dose in terms of the number of sessions (or contact days). With the exception of 2 studies (De Vriendt et al., 2016; Gitlin et al., 2006), authors did not report the exact length of the sessions. Three studies did not provide sufficient detail to determine the intervention dose (de Almeida Mello et al., 2016; Mann et al., 1999; Metzelthin et al., 2013). The primary barrier to calculating intervention dose was that some studies reported the use of an occupational therapy evaluation and plan of care but did not report the number of intervention contacts that resulted from implementing the plan of care (i.e., de Almeida Mello et al., 2016; Mann et al., 1999; Metzelthin et al., 2013; Stewart et al., 2005).
On the basis of the available data, the minimum intervention dose was 134 min (De Vriendt et al., 2016). We were unable to determine the maximum dose. The total study duration also varied, with 2 studies lasting 2–3 mo (De Vriendt et al., 2016; Fisher et al., 2007), 2 studies lasting between 8 and 9 mo (Stewart et al., 2005; Yuri et al., 2016), 3 studies lasting between 1 and 2 yr (Dahlin-Ivanoff et al., 2010; Mann et al., 1999; Metzelthin et al., 2013), and 3 studies lasting more than 3 yr (de Almeida Mello et al., 2016; Gitlin et al., 2006; Ollonqvist et al., 2008).
Frailty Intervention Outcome Measures
The outcome measures used to determine the effectiveness of interventions targeting frail older adults varied throughout the 10 studies. Ability or disability in daily activities was the most common primary outcome; it was used in 6 studies (De Vriendt et al., 2016; Fisher et al., 2007; Gitlin et al., 2006; Mann et al., 1999; Metzelthin et al., 2013; Stewart et al., 2005). Six different measurement tools were used: the FIM®, the Katz ADL Index (Katz et al., 1970), a study-specific ADL index, the Assessment of Motor and Processing Skills (Fisher & Jones, 1999), a modified World Health Organization questionnaire (de Bruin et al., 1996), and the Community Dependence Index (Eakin & Baird, 1995).
Additional primary outcomes included postponing or reversing frailty indicators (Dahlin-Ivanoff et al., 2010; Yuri et al., 2016), quality of life (Yuri et al., 2016), support received from relatives and municipal or private services (Ollonqvist et al., 2008), permanent institutionalization (de Almeida Mello et al., 2016), and social integration (Mann et al., 1999). The most common secondary outcomes were fear of falling, quality of life, social participation, health care costs, caregiver burden, and death.
Discussion
We conducted a scoping study to characterize the use of occupational therapy interventions to improve outcomes among frail community-dwelling older adults. Provencher et al. (2012) previously noted an underutilization of the frailty concept in occupational therapy discourse and among occupational therapy researchers. The general underutilization of the concept in the occupational therapy research literature may help explain why so few studies met our inclusion criteria and why so few of those studies were published in occupational therapy journals. In addition, the majority of the studies included in this review were conducted outside of the United States. One plausible explanation for this is that our review focused on interventions delivered to community-dwelling older adults. Because occupational therapists can deliver services in both home and primary care settings in many European and Scandinavian countries (as opposed to the United States, where primary care practice is uncommon), it is possible that the lesser number of U.S.-based studies with this population is an artifact of differences in practice contexts and, by default, research contexts.
Operationalization of Frailty
Among the studies included in this review, only 3 used a validated frailty measure to either identify frail participants or to assess the effect of the intervention (de Almeida Mello et al., 2016; Metzelthin et al., 2013; Yuri et al., 2016). The majority of studies operationalized frailty in terms of functional ability or disability. In our view, operationalizing frailty in these ways is problematic for several reasons.
The increasingly multidisciplinary nature of frailty research (Elsawy & Higgins, 2011; Wells et al., 2003) necessitates clarity in how studies operationalize frailty, especially if the results are to be used and interpreted across the broader scientific community. In the broader aging literature, frailty is characterized as a constellation of factors or deficits, and it is considered a concept distinct from related terms such as physical function and disability. Although frailty is predictive of ADL disability (Al Snih et al., 2009; Boyd et al., 2012; Fried et al., 2001) and some frail older adults may develop ADL disability (especially in the later stages of frailty), frailty and disability do not refer to the same phenomenon (Fried et al., 2004). Not all disabled people are frail, and not all frail people have a functional disability.
Distinguishing frailty from related concepts is also important if occupational therapists intend to prevent or delay the development of frailty because evidence suggests that, to be most effective, frailty interventions should target prefrail or moderately frail older adults (Daniels et al., 2008; Stuck et al., 2002). Using ADL disability as a proxy for frailty could mean that interventions are targeting a group who are already severely frail and, therefore, less likely to benefit from intervention (Fernández-Garrido et al., 2014; Reuben et al., 1990). We are not suggesting that functional disability is not an important metric to consider in frailty research, only that it should be included along with a validated frailty measure to ensure that intervention recipients can indeed be classified as frail.
Occupational Therapy Treatment Content and Dose
Our search stream and study selection strategy resulted in intervention studies that used occupational therapy as the primary intervention and as part of a multidisciplinary approach. There is continued emphasis on comprehensive, multidisciplinary geriatric assessment for frail older adults (Elsawy & Higgins, 2011; Wells et al., 2003), and occupational therapists can play an important role in multidisciplinary approaches (Provencher et al., 2012). However, some multidisciplinary studies did not describe the occupational therapy content or dose in great detail. It is plausible that such omissions may be as much the result of publication biases and, in particular, the lack of space allotted to fully report all features of research studies as to deficits in study methodology.
Information on content and dose is paramount to translating evidence into clinical practice. Researchers should, therefore, work to ensure that it is possible to determine the contributions of occupational therapy in multidisciplinary approaches. Researchers can address this issue by carefully delivering and documenting the role of occupational therapy in interventions and quality improvement initiatives (and including additional data in the appendices of published reports). Researchers may also be interested in using intervention designs, such as the Multiphase Optimization Strategy Trial (Collins et al., 2007), that could be used in multidisciplinary approaches to evaluate the occupational therapy–specific contributions to the outcomes of interest.
Frailty Intervention Outcome Measures
The primary and secondary outcomes represented in the studies we reviewed reflect the tendency for studies to operationalize frailty in terms of activity disability or limitation. Only 3 studies (Dahlin-Ivanoff et al., 2010; Metzelthin et al., 2013; Yuri et al., 2016) reported changes in frailty status as a primary outcome. Future research proposing to reduce the impact of frailty among older adult populations should use measures of frailty and collect data preintervention and postintervention to determine the impact on frailty. Additional factors amenable to occupational therapy intervention (e.g., cognitive functioning and social participation) and contributing to the development of frailty (Resnick, 2014; Zaslavsky et al., 2013) were not more widely represented in the outcomes assessed. Future studies should investigate whether occupational therapy intervention might have a positive impact on other primary and secondary outcomes, such as social participation, social role functioning, depressive symptoms, or self-management of chronic conditions, because those factors are also implicated in the development of frailty.
Limitations
We limited this review to research on frail, community-dwelling older adults. As such, we omitted research with institutionalized populations, which constitute a significant proportion of frail older adults. Such interventions may have operationalized frailty differently, used different treatment approaches to ameliorate the effects of frailty, or focused on different outcomes. Despite these limitations, we followed a rigorous scoping review methodology (Arksey & O’Malley, 2005; Levac et al., 2010), searched a wide range of electronic databases to ensure that the most relevant studies were included, and used multiple reviewers at every step of data extraction and analysis. We are therefore confident that this scoping review provides a clear and current summary of occupational therapy interventions conducted with frail, community-dwelling older adults.
Implications for Occupational Therapy Practice
Occupational therapy can potentially attenuate the development and consequences of frailty by comprehensively evaluating and addressing individual and environmental factors related to older adults’ psychosocial functioning, social participation, and physical functioning. The results of this scoping review suggest that additional research is needed to build the evidence base. Researchers and practitioners can contribute to this goal in the following ways:
Researchers and practitioners can become familiar with frailty as a concept distinct from disability or functional ability.
Researchers can become familiar with frailty screening measures and consider integrating measures as part of research designs or clinical practice to identify at-risk older adults and track their response to intervention.
Practitioners can evaluate home environments and assistive technologies that could help prevent or slow older adults’ progression to frailty.
Conclusion
We conducted a scoping review of occupational therapy interventions to reduce frailty. Studies included in this review most often operationalized frailty as activities of daily living disability versus as a clinical syndrome or loss of reserve, as is common across the broader gerontological literature. In addition, the majority of studies did not use validated frailty measures to identify frail older adults. Future studies should consider operationalizing frailty in line with the broader gerontological literature and including validated frailty measures. Such additions would allow for better comparisons of the efficacy of occupational therapy–based interventions with other approaches to frailty reduction.
Footnotes
*
Indicates article included in the scoping review.