
Abstract
Systemic lupus erythematosus (SLE) is a highly inflammatory autoimmune disease that affects multiple organs, such as the kidneys; skin; and the cardiovascular, pulmonary, and central nervous systems (Petri et al., 2012; Pons-Estel et al., 2010). The disease can be mild or life threatening. SLE affects about 1.5 million people worldwide (Lupus Research Alliance, 2016) and disproportionally affects women and non-White populations (Pons-Estel et al., 2010). The peak age of onset is between ages 15 and 40 yr (Pons-Estel et al., 2010). Major symptoms associated with SLE include physical and mental fatigue; muscle weakness; cognitive impairment; hair loss; mouth sores; sensitivity to sunlight; and a malar rash on the face that extends over the cheeks and nose, referred to as a butterfly rash (Petri et al., 2012).
SLE severely affects occupational performance, participation, and self-esteem (Bauernfeind et al., 2009; Leuchten et al., 2014). A thematic analysis of 46 qualitative studies of people with SLE reported themes of restricted lifestyles, disrupted identity, and social stigma (Sutanto et al., 2013). Pain, fatigue, decreased memory, and unpredictability of the disease were identified as symptoms limiting participation. Two studies reported that the most difficult occupations for people with SLE were doing housework, home repairs, and paid work as well as participating in physical and social leisure activities; however, basic self-care activities were not as difficult (Katz et al., 2008; Macejová et al., 2013).
These findings were similar to those of another study that examined occupational performance deficits in an international group of people with SLE (Stamm et al., 2014). Moreover, occupational performance deficits have been found to be related to decreased muscle strength (Andrews et al., 2015), joint involvement and pain (Björk et al., 2015), and fatigue and cognitive impairment (Connolly et al., 2014; Katz et al., 2008; Pettersson et al., 2010; Sutanto et al., 2013). Work loss has been reported to be considerable and to range from 20% to 40% in people with SLE (Al Dhanhani et al., 2009; Yelin et al., 2009, 2012).
Literature on the role of occupational therapy or nonpharmacological management of SLE is limited. Yet, people with SLE have reported dissatisfaction with care and information received for fatigue, pain, cognitive impairment, and ability to perform daily activities (Serrano-Aguilar et al., 2015), all of which are within the scope of occupational therapy practice. An understanding of the effectiveness of interventions targeted at improving these outcomes can help occupational therapy practitioners select evidence-based interventions to use with people with SLE. Thus, the purpose of this review is to summarize evidence focused on interventions and outcomes that are of interest to occupational therapy practitioners, similar to other systematic reviews conducted on rheumatoid arthritis and fibromyalgia (Poole & Siegel, 2017; Siegel et al., 2017). Specifically, the review was completed to answer the following question: What is the evidence for the effectiveness of interventions within the scope of occupational therapy practice on occupational performance, pain, fatigue, depression, and cognitive impairment in people with SLE?
Method
This review is part of the American Occupational Therapy Association (AOTA) Evidence-Based Practice Project. The methods used for the review were based on Preferred Reporting Items for Systematic Reviews and Meta-Analyses (Moher et al., 2009) guidelines. The methodology consultant to the AOTA Evidence-Based Practice Project, as well as AOTA staff and the authors, developed the search terms for the systematic review. The advisory group reviewed terms to ensure that they would collect relevant articles in each database. A medical research librarian with experience in completing systematic review searches confirmed the search strategy and completed the searches. Table 1 lists the search terms; the search strategy is outlined in Appendix A (at the end of this article).
Search Terms for Systemic Lupus Erythematosus
Note. AAROM = active assistive range of motion; ADLs = activities of daily living; AROM = active range of motion; EMG = electromyography; IADLs = instrumental activities of daily living; NCV = nerve conduction velocity; PROM = passive range of motion.
Databases and sites searched included MEDLINE, PsycINFO, CINAHL, OTseeker, and Ergonomics Abstracts. The following Evidence-Based Medicine Reviews databases were also included: the Cochrane Database of Systematic Reviews, the Cochrane Controlled Trials Register, and the Database of Abstracts of Reviews of Effectiveness. In addition, bibliographies from articles included in the databases and relevant journals were hand searched as needed to confirm that all appropriate articles were included.
Inclusion criteria required that the intervention or study be within the scope of occupational therapy practice as defined in the Occupational Therapy Practice Framework: Domain and Process (3rd ed.; AOTA, 2014), be published in English and related to adults, and be considered as peer-reviewed scientific literature (Level I, Level II, or Level III as defined by Sackett et al., 1996). The literature included in the review was published between January 2000 and December 2017, and it included adult participants with a diagnosis of SLE. Exclusion criteria included data from conference proceedings, presentations, dissertations, theses, and non–peer-reviewed research literature.
The initial citation and abstract search yielded 74 articles that were related to SLE. The first and second authors independently reviewed the citations and abstracts, and duplicates between the multiple databases and articles that did not meet the inclusion criteria described earlier were removed. Discrepancies were discussed until consensus was reached. From the remaining list, the full-text versions of potential articles were retrieved, and the first two authors made further exclusions on the basis of predetermined exclusion criteria. Discrepancies were discussed until consensus was reached. A summary of article exclusions with reasoning is presented in Figure 1. Details on each article’s interventions, methods, outcome measures, and major findings are summarized in Table 2 (at the end of this article). The following relevant outcomes were emphasized: function or occupational performance, depression and anxiety, coping and self-efficacy, fatigue, cognition, and disease symptoms.
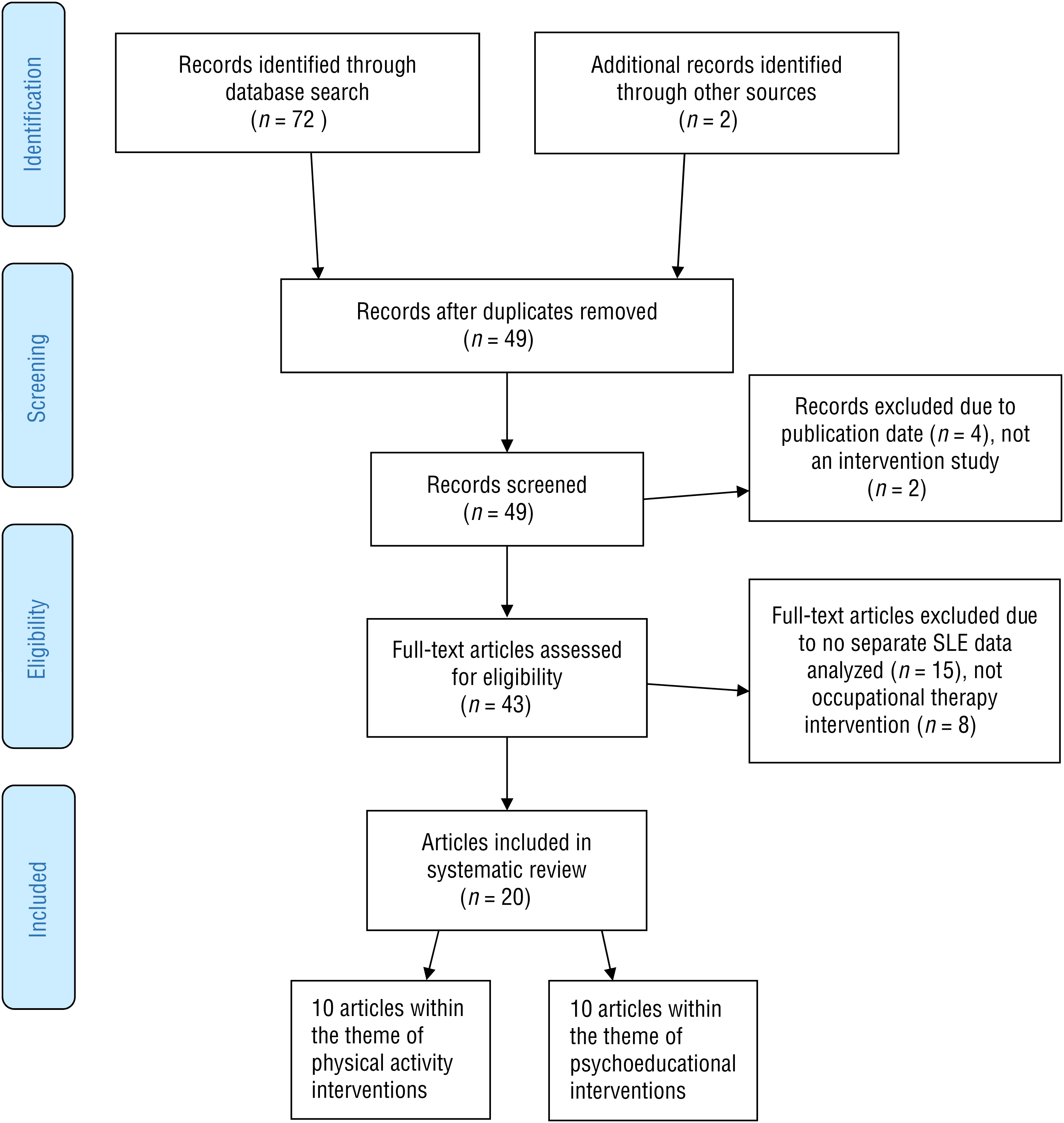
Flow diagram for inclusion and exclusion process of peer-reviewed studies.
Methodological quality and bias were assessed independently by the second and third authors with the PEDro scale (de Morton, 2009) to assess quality (Table 3, at the end of this article) and the criteria developed by the Cochrane Methods Group to assess risk of bias (Higgins et al., 2011; Table 4, at the end of this article). Discrepancies were discussed until consensus was reached. Finally, evidence within the themes described in the Results section was evaluated according to the number of studies and level of evidence using the guidelines from the U.S. Preventive Services Task Force (2016). Consistent results from 2 or more Level I randomized controlled trials (RCTs) or 1 Level I systematic review or meta-analysis were considered strong evidence. Consistent results in 1 Level I study plus 2 or more lower level studies were rated as moderate evidence. When only 1 Level II or consistent results in multiple lower level studies were found, these intervention areas were considered as having limited evidence. Lack of evidence supporting an intervention and poor-quality or conflicting evidence were rated as insufficient evidence.
Results
The final set of 20 articles consisted of 10 Level I, 5 Level II, and 5 Level III studies. They were grouped and divided into two broad categories: physical activity (n = 10) and psychoeducational (n = 10) interventions.
Physical Activity Interventions
The physical activity interventions were classified into the following subthemes: supervised aerobic training (n = 4), supervised aerobic training in conjunction with a home-based exercise program (n = 5), and home-based-only exercise programs (n = 1).
Supervised Aerobic Training.
The 4 studies included in this subtheme (1 Level I, 2 Level II, and 1 Level III) involved aerobic exercise on a treadmill and on a bicycle ergometer. The Level I study (Abrahão et al., 2016) and 1 of the Level II studies (Bogdanovic et al., 2015) found improvements in function but not depression postintervention; group differences were also found favoring aerobic training over strength training for function. The other Level II study (Carvalho et al., 2005) reported notable improvements in depression and function in the intervention group compared with the control group. The Level III study (Clarke-Jenssen et al., 2005) with 6 participants found that they all had improved function and fatigue and no increase in disease symptom severity postintervention, but the changes were not statistically significant.
Supervised Aerobic Training in Conjunction With a Home-Based Exercise Program.
This theme included 4 RCTs and 1 Level II study. Three Level I studies compared supervised aerobic training with another condition in addition to usual care. Although participants in all 3 studies showed considerable improvements in fatigue, and participants in 2 reported improvements in function, there were no notable group differences. There were also no increases in disease activity. Thus, supervised aerobic training did not appear to be superior to range of motion and strengthening (Ramsey-Goldman et al., 2000), relaxation (Tench et al., 2003), or a home-only exercise program (Avaux et al., 2016). The fourth Level I study, in which the intervention was conducted over 12 mo, also found no group differences compared with usual care (Boström et al., 2016). However, the one Level II study did find group differences for function, but the sample size was small (n = 18; Perandini et al., 2014).
Home-Based Exercise Program.
One Level III study examined the effectiveness of a 10-wk, home-based Wii Fit exercise program (Yuen et al., 2011). Individualized instruction was provided at home along with visits from one of the researchers every 3 wk and weekly telephone monitoring. At postintervention, there were notable decreases in fatigue, anxiety, total pain, and weight but not in depression or sleep quality.
Psychoeducational Interventions
The psychoeducational interventions used in the articles were classified into the following subthemes: education and self-management (n = 6) and cognitive–behavioral therapy (CBT; n = 4).
Education and Self-Management.
One Level I study, 2 Level II studies, and 3 Level III studies evaluated the effects of education and self-management programs. The Level I study, which included both people with SLE and their partners, reported considerable improvements favoring the intervention for communication, coping, social support, self-efficacy, fatigue, mental health, and physical function (Karlson et al., 2004). Two studies that evaluated self-management education programs based on the Arthritis Foundation Self-Management Programs (1 Level II and 1 Level III) reported improvements in fatigue, depression, coping skills, and self-efficacy compared with usual care (Drenkard et al., 2012; Sohng, 2003). Drenkard et al. (2012) also found improvements in physical function and cognitive symptom management.
Similar findings were reported in a nonrandomized Level II study (Haupt et al., 2005) that evaluated an education self-management intervention. At 6 mo postintervention, the intervention group showed notable improvements for depression, anxiety, overall mental burden, and quality of life but no improvement in disease activity compared with the waitlist control group. Two Level III studies evaluated interventions led by occupational therapists. One study (Harrison et al., 2005) evaluated an 8-wk cognitive strategy education intervention led by an occupational therapist. The intervention, consisting of psychosocial support and strategy training with real-life situations, resulted in improvements in the areas of metamemory, functional coping, and self-efficacy. The other study assessed a fatigue management intervention (O’Riordan et al., 2017). The 6-wk program, led by an occupational therapist, found considerable improvements for physical function, self-monitoring, skill acquisition, and depressive symptoms but no improvements in self-efficacy or activity participation.
Cognitive–Behavioral Therapy.
This theme included 3 Level I studies that evaluated the effectiveness of CBT interventions and 1 Level I study that assessed mindfulness-based cognitive therapy. CBT uses cognitive techniques to help people become more aware of negative thinking and respond to challenging situations more effectively. Two RCTs (Navarrete-Navarrete, Peralta-Ramírez, Sabio, et al., 2010; Navarrete-Navarrete, Peralta-Ramírez, Sabio-Sánchez, et al., 2010; Solati et al., 2017) evaluated the same 10-wk CBT intervention. Both studies reported that the intervention groups showed notable improvements in physical role function, vitality, general health, mental health, social function, and pain postintervention and at the 15-mo follow-up compared with the control group.
The third Level I study compared the effects of a biofeedback-assisted CBT intervention with a symptom-monitoring support system condition and a usual medical care group (Greco et al., 2004). The biofeedback-assisted CBT intervention demonstrated considerable reductions in pain, depressive symptoms, and perceived stress levels as well as increased self-efficacy compared with the symptom-monitoring support system intervention and usual medical care group. Benefits were sustained at 9-mo follow-up for self-efficacy and stress but not for depressive symptoms (Greco et al., 2004). Mindfulness-based cognitive therapy also resulted in notable improvements at follow-up for psychological symptoms of depression, anxiety, social function, and psychological function but not for physical function on the 36-item Short Form Health Survey (SF–36; Solati et al., 2017; Ware & Sherbourne, 1992).
Methodological Quality and Risk of Bias
Of the 20 studies included in the review, we rated only 8 studies as having good methodological quality using the PEDro scale; 5 studies were fair, and 7 studies were poor (see Table 3, at the end of this article). Because of the types of interventions included (exercise, education, CBT), it was not possible to blind the participants or the interventionists for the RCTs (Level I) or the non-RCTs (Levels II and III). Moreover, in the non-RCTs, random and concealed allocations were not achievable because of the study designs, which further lowered the PEDro scores. The assessment of bias also supported the PEDro methodological scores in that only 1 study had sufficient blinding of participants, 12 studies reported blinding of outcome assessment, and 14 studies had poor descriptions of randomization methods or allocation concealment. Intention-to-treat analyses were not described.
Full details of the risk for bias for the studies included in the review are reported in Table 4 (at the end of this article). Although neither the PEDro scale nor the risk-of-bias criteria specifically evaluated the quality of the outcome assessments used in the reviewed studies, the SF–36 (an assessment with strong psychometric properties) was an outcome in 16 of the 20 studies. Other well-validated scales, such as the Fatigue Severity Scale, Beck Depression Inventory, Hospital Anxiety and Depression Scale, and the Measures of Disease Activity for SLE, were also included as outcomes. See Katz (2011) for descriptions of the psychometric properties of these outcomes.
Discussion
In this systematic review, we examined the evidence for physical activity and psychoeducational interventions within the scope of occupational therapy practice for people with SLE. Although few studies have examined the effectiveness of nonpharmacological interventions for this population, the findings from this review are promising. Five Level I studies, 3 Level II studies, and 2 Level III studies on physical activity interventions showed benefits for depression, fatigue, exercise tolerance, and function and no exacerbation of disease activity. However, because 4 of the studies had fewer than 20 participants, there appears to be only moderate evidence for physical activity for people with SLE.
Our review also found moderate evidence for self-management and educational interventions. One Level I study, 2 Level II studies, and 3 Level III studies reported considerable improvements in coping skills and fatigue (Drenkard et al., 2012; Karlson et al., 2004; O’Riordan et al., 2017; Sohng, 2003) as well as social support and couples’ communication (Haupt et al., 2005; Karlson et al., 2004). Moreover, the cognitive intervention investigated in a Level III study was also shown to be beneficial in improving problem solving and self-efficacy (Harrison et al., 2005). Because of the prevalence of cognitive dysfunction and the effect on daily life (Petri et al., 2012; Robinson et al., 2010), the positive effects of the cognitive intervention suggest that cognitive interventions for people with SLE should be investigated further.
Four Level I studies provide strong evidence for CBT. These studies all found improvements in pain, depression and anxiety, perceived stress, quality of life, and function (Greco et al., 2004; Navarrete-Navarrete, Peralta-Ramírez, Sabio, et al., 2010; Navarrete-Navarrete, Peralta-Ramírez, Sabio-Sánchez, et al., 2010).
Although fatigue was an outcome in several of the studies on both physical activity and psychoeducational interventions, only 2 studies (O’Riordan et al., 2017; Yuen et al., 2011) evaluated fatigue as a primary outcome. Fatigue is another symptom that affects participation in daily life in people with SLE (Sutanto et al., 2013), but only the study by O’Riordan et al. (2017) specifically focused on fatigue management. Specific fatigue interventions were found to be effective for people with other rheumatic diseases such as rheumatoid arthritis (Cramp et al., 2013) and neurological conditions such as multiple sclerosis (Lee et al., 2008). These interventions might be useful for people with SLE.
Limitations
Limitations of the studies included in the review were the small sample sizes, participants’ gender, and the heterogeneous types and lengths of interventions within any one theme. Only 1 study included in the review had more than 100 participants; 14 studies had fewer than 50 participants. Most studies did not include a proportion of men (10% of people with the diagnosis) representative of the actual population of people with SLE. Indeed, in 8 studies, 100% of the participants were women. In addition, the short intervention periods and limited follow-up in the studies (10–12 wk) made it difficult to predict long-term outcomes, which subsequently made it difficult to directly compare interventions or see any effects of the variations in the interventions, patient demographics, length of interventions, and postintervention follow-ups. Most studies were conducted outside the United States, which may limit generalizability to the U.S. health care system. Another limitation of the review is that we did not include gray literature; thus, we may have missed relevant and important studies (Benzies et al., 2006).
Implications for Occupational Therapy Practice
Most studies in this review were not conducted by occupational therapy practitioners, but the interventions are within the scope of occupational therapy practice. However, the complexity of SLE and the effect of SLE on participation in daily life and work suggest that occupational therapy has an important role in the management of this disease. The results of this review have the following implications for occupational therapy practice:
Occupational therapy practitioners could encourage people with SLE to include physical activity as part of their daily routine, such as aerobic exercise to improve function, fatigue, pain, and depression.
Because cognitive deficits are commonly reported in people with SLE, occupational therapy practitioners might want to assess functional cognition and its effect on occupational performance to provide appropriate interventions.
Occupational therapy practitioners can use a variety of psychoeducational interventions, such as CBT, self-management, and education, to improve psychosocial functioning, pain, fatigue, functional cognition, and occupational performance.
Future occupational therapy research could evaluate the effectiveness of energy conservation principles and compensatory strategies to manage fatigue and cognitive deficits.
Occupational therapy practitioners should identify client-centered goals with people with SLE and help modify tasks or provide adaptive skills training to best meet their goals.
Most studies did not include client-centered outcomes or measures of participation. Future research needs to evaluate the effectiveness of client-centered interventions on participation in meaningful occupations. Assessments such as the Canadian Occupational Performance Measure (Law et al., 2014) could be used to identify goals and as a basis for individualized interventions.
Few studies specifically evaluated occupational therapy as an intervention or included occupational therapy as part of an intervention. More well-designed RCTs are needed with occupational therapy as the sole intervention or as a specific intervention component.
Occupational therapy practitioners can help develop services to assist people with SLE to stay active. They can also refer clients to online or community-based support programs to access social support and educational resources.
Practitioners can help themselves and their clients learn more about SLE by consulting the following websites: the Lupus Initiative (http://thelupusinitiative.org/patients-caregivers/), the Lupus Foundation of America (https://www.lupus.org/), and the Arthritis Foundation (https://www.arthritis.org/about-arthritis/types/lupus/). All these websites contain education and resources for people with SLE, their families and caregivers, and health professionals. In addition, the Lupus Initiative has resources for educators and students at http://thelupusinitiative.org/educators-students/.
Conclusion
We conducted a systematic review of interventions within the scope of occupational therapy practice for people with SLE. Moderate evidence was found to support physical activity, self-management and educational interventions, and CBT. Few studies were conducted by occupational therapy practitioners. Because of the effect of SLE on participation in daily life and work, future studies should investigate occupation-based interventions.1
Footnotes
Acknowledgments
We thank Marian Arbesman, Deborah Lieberman, and Ingrid Hendrix for their support and assistance with this review.
Search Strategy for the Systematic Review on Systemic Lupus Erythematous
Database: Ovid MEDLINE(R) <1946 to May Week 4 2014>
Search Strategy:
Suggested citation: Poole, J. L., Bradford, J. D., & Siegel, P. (2019). Effectiveness of occupational therapy interventions for adults with systemic lupus erythematosus: A systematic review (Appendix). American Journal of Occupational Therapy, 73, 7304205020. https://doi.org/10.5014/ajot.2019.030619
*
Indicates studies included in the systematic review.