
Abstract
In stroke rehabilitation, evidence suggests that increased arm movement promotes functional recovery (Nudo et al., 1996). Objective, affordable measures for monitoring upper extremity (UE) use can provide feedback to clinicians and clients on improvements and inform intervention planning. Logs and self-reports (Duncan et al., 1999; van der Lee et al., 2004) have been used to record clients’ efforts but may not be reliable because of possible biases and human error.
Accelerometry is a quantifiable measure of how much people move their arms and hands in everyday functional activities (Bailey et al., 2014). Accelerometers measure movement of acceleration, which is change in speed with respect to time and is measured in gravitational acceleration units (1 g = 9.8 m/s2). Wrist-worn accelerometers work by converting mechanical motion into electrical signals through piezoelectric sensors contained within a device, similar in size to a wristwatch, that can be comfortably worn on the wrist.
Accelerometry is a valid and reliable measure of UE activity that is well established in stroke research (Bailey & Lang, 2013; Lang et al., 2007; Rand & Eng, 2015; Urbin, Bailey, & Lang, 2015; Uswatte et al., 2005, 2006). Uswatte et al. (2000) found initial evidence for the validity of accelerometer recordings in objectively measuring the amount of real-world UE movement as an index of treatment outcome for rehabilitation patients. Overall, accelerometry to measure movement provides an objective, real-world index of impaired arm activity and has good psychometric properties (Uswatte et al., 2005, 2006). This quantitative measurement eliminates the possible reporting biases in self-reports. The use of accelerometry thus provides a more quantitative and accurate measurement of arm movement than client report of use. Although accelerometers have been used in research, little is understood of the utility of the various types of accelerometer for measuring arm recovery in a clinical setting.
The ActiGraph® Bluetooth® Smart wGT3X-BT wireless activity monitor (ActiGraph, Pensacola, FL) is considered the gold standard in UE accelerometry movement analysis for research. The ActiGraph has been shown to be sensitive and to collect accurate data on UE movement for research purposes (André et al., 2004; Bailey et al., 2014; Bailey & Lang, 2013; Lang et al., 2007, 2008; Uswatte et al., 2000, 2005, 2006). However, the ActiGraph might be considered expensive, and interpretation of results (although detailed) might be considered difficult and cumbersome.
A less expensive device that is readily available to consumers from retail and online vendors is the Fitbit® (Fitbit, San Francisco, CA). It yields easily obtained and readily interpretable details of UE movement and might be more feasible in everyday practice settings. The Fitbit Flex™ contains the same microelectromechanical systems and three-axis accelerometer as the ActiGraph. Although the data produced by the Fitbit Flex are not as detailed as ActiGraph data, the more simplified results may be used more readily in clinic settings. To date, no comparison between these two devices has been attempted.
The purpose of this study was to determine the reliability of the Fitbit Flex compared with the ActiGraph Bluetooth Smart wGT3X-BT wireless activity monitor. We also sought to contribute to the clinical utility of accelerometry measurement of UE movement by assessing movement in people without disabilities.
Method
Data were collected at two different sites and analyzed separately. Institutional review board approval was obtained at each site. The studies are referred to as Study 1 and Study 2.
Participants
Study 1.
A convenience sample of 47 participants without UE disability volunteered for Study 1. The participants were 32 women and 15 men ranging in age from 15 to 53 (average 25.7). The majority of the participants were right-hand dominant (n = 43).
Study 2.
A convenience sample of 24 participants consented to participate in Study 2. The participants were graduate students in an occupational therapy program, and none had reported UE disability. Study 2 participants consisted of 23 women and 1 man; 20 were right-hand dominant. Ages ranged from 24 to 42 (average 28.3).
Data Collection Procedures
Study 1.
Participants in Study 1 wore the ActiGraph Bluetooth Smart wGT3X-BT wireless activity monitor and the Fitbit Flex during everyday activities for a 24-hr period. Participants wore both devices on both right and left UEs (Figure 1). Devices were placed at the distal forearms, proximal to the styloid process of the ulna, to allow both proximal (i.e., upper arm) and distal (i.e., forearm) movements to be captured over time (Lang et al., 2007).

ActiGraph® Bluetooth® Smart wGT3X-BT wireless activity monitor, Fitbit® Flex™, and placement of the devices for Study 1.
Study 2.
Participants in Study 2 wore the ActiGraph Bluetooth Smart wGT3X-BT wireless activity monitor and the Fitbit Flex during a self-selected 4-hr period during an active time of the day. Participants wore both devices on their dominant arm.
Participant Instructions.
Participants from both studies were instructed to wear the accelerometers during their regular daily activities without any restrictions and to continue their normal daily activities. Number of steps was recorded by the Fitbit and ActiGraph. Steps were calculated by analyzing acceleration data about frequency, duration, intensity, and patterns of movement. In these studies, the accelerometers were worn on the forearm and thus measured the frequency, duration, intensity, and patterns of movement of the UE, which may have included movement that occurred while walking. The three-axis implementation allows the accelerometer to measure arm motion in all planes of movement. Acceleration in step count for both studies was sampled and analyzed similarly to data in Uswatte et al. (2000).
In Study 1, the number of steps from the ActiGraph and Fitbit was recorded as activity completed within a 24-hr period. This specific measure was the most comparable measurement between the ActiGraph and Fitbit. In Study 2, the number of steps was recorded in 15-min increments for the ActiGraph and Fitbit, totaling 15 pairs of data points for each accelerometer.
Data Analysis
Pearson correlation coefficients were used to relate steps recorded on the Fitbit to steps recorded on the ActiGraph. A paired-samples t test was used to assess difference between the devices.
Results
For both studies, there was a strong positive correlation between steps on the ActiGraph and steps on the Fitbit. Correlations between the two accelerometers (worn on both arms) in Study 1 were r = .873 (n = 47, p < .0001) for the right arm and r = .863 (n = 47, p < .0001) for the left arm (Figure 2). The correlation between the two accelerometers (worn on the dominant arm only) in Study 2 was r = .810, n = 360, p < .0001.
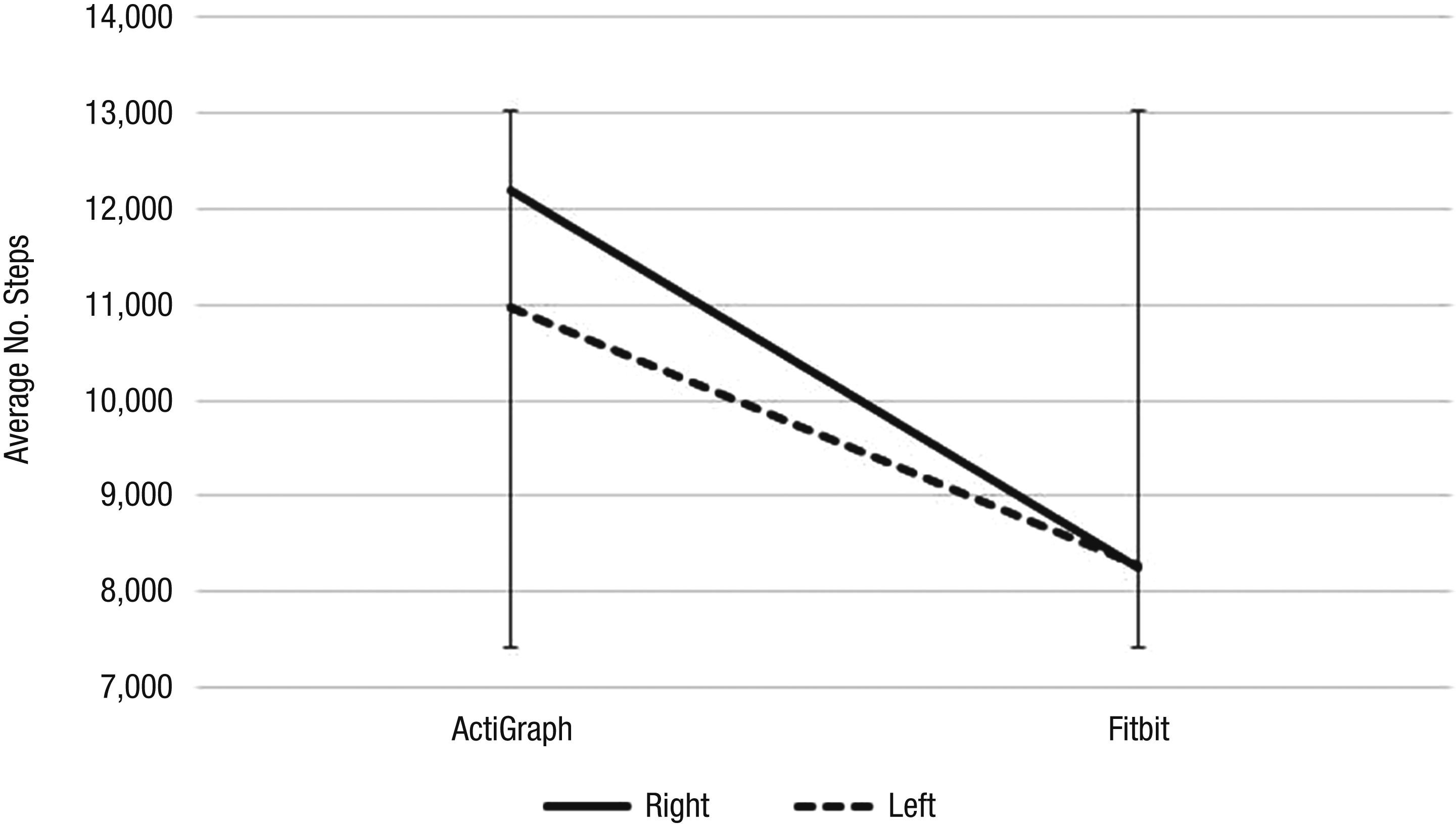
Comparison between sides and accelerometers for Study 1.
In Study 1, a significant difference was found between the number of steps recorded for the right arm on the ActiGraph (mean [M] = 12,203.2, standard deviation [SD] = 3291.8) and on the Fitbit, M = 8,248.7, SD = 3030.3, t(46) = 14.9, p < .0001 (paired sample, two-tailed). A significant difference was also found between the number of steps recorded for the left arm on the ActiGraph, M = 10,978.2, SD = 2,877.9, and on the Fitbit, M = 8,268.0, SD = 3245.7, t(46) = 11.3, p < .0001. In Study 2, a significant difference was found between the number of steps recorded on the ActiGraph, M = 171.91, SD = 143.72, and on the Fitbit, M = 113.88, SD = 175.13, t(359) = 10.58, p < .0001. These preliminary findings indicate that the Fitbit values were notably lower than the ActiGraph values.
Discussion
Activity monitors geared toward consumer use could make accelerometry much more user friendly. The accuracy of various activity monitors has been assessed in regard to stepping activity (Fulk et al., 2014); however, the reliability of various accelerometers, including commonly used and more expensive devices, used for UE movement has not been assessed. In our studies comparing the reliability of the Fitbit Flex to the gold-standard ActiGraph Bluetooth Smart wGT3X-BT, the results suggest that although there is a relationship between recordings on the Fitbit and the ActiGraph, the Fitbit is less sensitive in recording all steps, yielding lower step counts than the ActiGraph. These findings should not be interpreted as one accelerometer being better than the other; rather, clinicians thinking of using accelerometry need to consider the purpose of the tool’s use.
Accelerometry can be used as a quantitative measure of UE movement. Wrist accelerometers provide an objective measure of how much the arm moves (Connell et al., 2014); accelerometry was found in several studies to be a valid and reliable method to determine the amount of hemiparetic UE activity after stroke (Duff et al., 2016). A literature review by Duff and colleagues (2016) found clear examples of how accelerometry could feasibly be used as an outcome measure for functional assessment and as a feedback method for people with UE hemiparesis. The current studies show that an easily accessible and simple accelerometer like the Fitbit can be a way to monitor clients’ UE movement in rehabilitation therapy. Used as an ipsative measure, the Fitbit is an affordable, easy-to-use choice.
The studies presented in this article provide informative data on the clinical utility of the Fitbit compared with the ActiGraph. Although the use of an easily accessible, simpler accelerometer such as the Fitbit is clinically user friendly, our two studies with participants who did not have movement disorders showed that it was not as sensitive as the ActiGraph, which is more commonly used in research. Although the Fitbit did not record the same amount of movement as the ActiGraph, the Fitbit did record movement. In Study 1, on average, the Fitbit recorded 67.6% (right) and 75.3% (left) of the movement recorded by the ActiGraph. In Study 2, the Fitbit recorded 66.2% of the movement recorded by the ActiGraph. That said, the high positive correlations suggest a potential for use of the Fitbit in typical clinical settings.
UE accelerometry has been shown to provide good quantification of real-world upper limb activity and complements results from clinical tests of function when assessing recovery of activity after neurological injury (Bailey et al., 2015). The monitoring of bilateral UE movement with accelerometry in real-world settings might be useful to clinicians and motivating to clients with hemiparesis from stroke as an objective assessment of affected upper limb use or disuse and function (Narai et al., 2016). Note that in general, accelerometry values are different between movement recorded in the clinic and in the free-living environment, which indicates that what the paretic UE does in the clinic may not generalize to normal everyday movement (Urbin, Waddell, & Lang, 2015). In daily life, UE performance can be highly variable, with inconsistencies between change in capacity and change in performance (Doman et al., 2016). These findings may account for some of the variability seen in the participants of the current studies.
Future Research
Further testing comparing certain types of movement (e.g., gross motor vs. fine motor) and different patient populations (e.g., with various diagnoses) will provide evidence of the validity of these devices for recording movement. For example, although some studies have been performed, their results have been limited and evidence is lacking that improvement of motor function after intensive outpatient upper limb interventions continues after the end of therapy (Waddell et al., 2017). The measurement of “steps” from the two accelerometers we studied might benefit from a more refined definition and measurement of UE movement. The number of steps measured in these studies simply means more repetitions, not necessarily more purposeful movements. In addition, measures were taken on a very young sample, who may have been more active and may have had more variability in number of movements than other samples. Data from other patient populations, such as people with stroke and older adults, could yield less discrepancy between devices. However, any type of accelerometer may be of benefit as a motivator to increase movement by providing ongoing feedback to the wearer.
Implications for Occupational Therapy Practice
The results of this study can inform the use of accelerometry in assessing movement of the UE in the following ways:
The more easily accessible and simple Fitbit records data similarly to the ActiGraph, which has been considered the gold standard of accelerometry. The Fitbit may be more clinically accessible and useful than the ActiGraph for measuring UE movement because it is less expensive and easier to use.
The Fitbit is not as sensitive as the ActiGraph. The ActiGraph remains the more precise accelerometer for UE movement. However, the Fitbit may still usefully serve as a gross measure of UE movement. Further research can better inform clinicians on which populations might best benefit from which type of accelerometer.
The Fitbit provides immediate feedback, including number of steps, whereas ActiGraph data must be downloaded to a computer. By providing immediate feedback and programmed reminders, the Fitbit can act as a motivator to encourage movement.