
Abstract
In the United States, nearly 800,000 strokes occur each year; 6.6 million survivors of stroke are resident at any given time (Mozaffarian et al., 2015). Decreasing mortality (Mozaffarian et al., 2015), combined with increasing life expectancy (Lakshminarayan et al., 2014), ensures that many stroke survivors will require rehabilitation services for the foreseeable future. Thirty percent to 66% of stroke survivors experience limitations in upper limb function, among several sequelae (Kwakkel et al., 2003). The degree of upper limb limitation (Akyüz et al., 2015) and its successful treatment (Pulman & Buckley, 2013) are major determinants of quality of life after a stroke for both stroke survivors and caretakers, mandating continued research to maximize upper limb recovery, especially of the hand, where outcomes have been underwhelming (Lum et al., 2012; Pinter et al., 2013).
One strategy to enhance upper limb motor recovery is robotic therapy (Basteris et al., 2014; Blank et al., 2014). Robotic therapy initially focused on the proximal arm (Basteris et al., 2014), but several hand devices have now been developed and tested (Balasubramanian et al., 2010). Robotics are an attractive strategy for poststroke hand rehabilitation because they facilitate large numbers of repetitions through the full joint range of motion while limiting abnormal movements. Equally important is their promotion of active participation during training (Blank et al., 2014; Lum et al., 2012). Active participation is critical for motor recovery after stroke, and robotics promote it in at least three ways: (1) by providing just enough assistance to achieve a target movement while avoiding fatigue and frustration (Lum et al., 2012); (2) by simulating real-world activities through visual, auditory, and haptic feedback; and (3) by detecting and augmenting (i.e., actuating) a stroke survivor’s intention to move.
Detection of intent can occur via electroencephalography, force sensors, or electromyography (EMG; Blank et al., 2014; Lum et al., 2012). No commercially available device uses electroencephalography, but a few use force sensors, including the Amadeo™ (TyroMotion, Graz, Austria), InMotion™ Hand Module (Bionik Laboratories, Toronto), and the Manovo Power™ module of the Armeo Power (Hocoma, Volketswil, Switzerland). The Hand of Hope™ (HoH; Rehab-Robotics, Hong Kong), used in this study, uses surface EMG to trigger actuated movement at the fingers. EMG-triggered robotic devices may hold an advantage over force sensors because the latter require some degree of volitional movement, whereas the former can detect the intent to move even with minimal force generation or detectable motion (Blank et al., 2014).
The HoH detects electrical activity in the extensor digitorum and flexor digitorum superficialis through surface EMG sensors placed on those muscles (Figures 1A and 1B). Once the client achieves a predetermined EMG threshold signal, the device provides active assistance to achieve either a single repetition of mass finger flexion or extension through the entire range of motion. If a client can initiate muscle contraction of the finger flexors or extensors, the device will assist in fully opening or closing the affected hand.
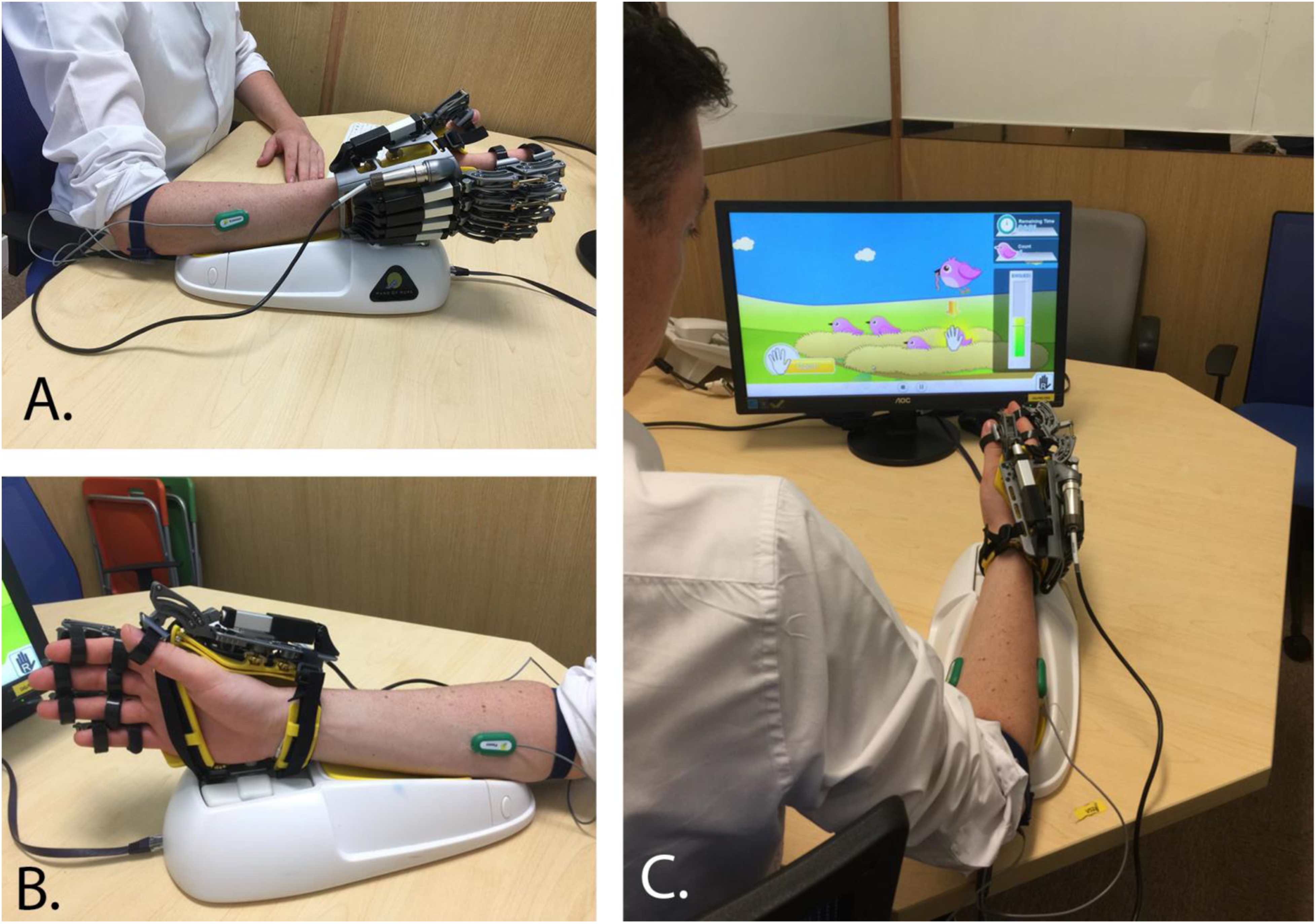
(A) Dorsal view of Hand of Hope with forearm platform. (B) Palmar view of Hand of Hope with forearm platform. (C) Hand of Hope system with video game interface promoting mass hand extension while incorporating proximal reach.
Although a prototype version of the HoH functioned as an exoskeleton, the current commercial version has a forearm platform that supports the weight of the device on a tabletop surface during training and has a videogame interface (Figure 1C). The HoH is an investigational device, not approved by the U.S. Food and Drug Administration. There is minimal published research on the device (Ho et al., 2011; Hu et al., 2013; Tong et al., 2010), and earlier studies did not provide feasibility data or use the commercial version. The aims of this study were to determine the feasibility of using the HoH and to collect initial data on clinical outcomes after 18 treatment sessions.
Method
Participants
The study was approved by an institutional review board, and written consent was obtained from all participants before any intervention. Twelve participants were recruited using study flyers, our departmental stroke research registry, and referrals from outpatient clinicians. Inclusion criteria were at least 6 mo poststroke, some active movement in the affected hand (specifically, the ability to pick up and release a 2.5-cm3 block from a tabletop surface), intact sensation to light touch and pain in the affected hand, full passive range of motion (PROM) in mass flexion and extension, a Modified Ashworth Scale (Katz et al., 1992) score of ≤3 at the finger flexors and extensors, PROM of wrist extension and metacarpophalangeal extension to neutral (90°), intact visual tracking in all directions, and medically stable.
Participants were excluded if they were receiving concurrent occupational or physical therapy for the upper extremity, had joint contractures that prevented proper fit into the HoH device, experienced other neurological or orthopedic conditions affecting motor ability or joint range of motion, received botulinum toxin injections in the affected upper extremity within the previous 3 mo, or had minimal motor impairment (able to perform Stage 6 tasks of the Chedoke Arm Assessment (Barreca et al., 2005). Participant training on the HoH was supervised by a licensed occupational therapist. Outcome measures were completed by research staff not involved in the participants’ training.
Baseline characteristics of participants are outlined in Table 1. Ten of the 12 participants were female, with a mean age of 57 yr (standard deviation [SD] = 10.2, ranging from 39 to 79) and mean time since stroke of 5 yr (SD = 4.0). One participant could not be reached at follow-up despite multiple attempts, resulting in missing data at follow-up. Because of the small sample size and the nonrandom nature of the missing data, we carried all discharge scores forward to serve as this participant’s follow-up scores.
Participant Demographics (N = 12)
Note. M = mean; SD = standard deviation.
Instruments
Using the World Health Organization's (2001) International Classification of Functioning, Disability and Health as a framework, assessments reflecting all three levels of disability (impairment, activity, and participation) were selected to measure clinical outcomes after hand training. The Stroke Upper Limb Capacity Scale (SULCS; Roorda et al., 2011) measures the capacity of the affected upper limb after stroke. Each of the 10 items, arranged in a hierarchical order, are assigned a score of 0 (unable to complete the task) or 1 (able to complete the task) with a maximum score of 10. The SULCS psychometric properties have been well-studied (Houwink et al., 2011; Roorda et al., 2011).
The Box and Block Test is a performance-based assessment of gross manual dexterity for adults after stroke. The total score is the number of 2.5-cm3 blocks successfully transferred from one compartment to another in 1 min. The assessment has strong interrater and test–retest reliability (Platz et al., 2005).
The dynamometer is a valid and reliable assessment of grip strength measured in kilograms (Kitsos et al., 2011). Handgrip strength has been shown to be directly related to activities of daily living for the healthy population (Taekema et al., 2010). Grip strength score is the average of three trials.
The Fugl-Meyer Assessment (FMA; Fugl-Meyer et al., 1975) is a widely used, valid, and reliable (Sullivan et al., 2011) performance-based measure of arm impairment. The FMA assesses proximal and distal movements in and out of synergy patterns as well as strength and coordination of fine motor movements. For this study, the three reflex items were omitted from the final score because they are considered a separate construct from motor impairment (Woodbury et al., 2013), making the maximum score 60.
The Arm Motor Ability Test (AMAT; Kopp et al., 1997) is a reliable and valid assessment (O’Dell et al., 2011) of activity limitation after stroke. It includes 10 functional tasks, such as using a knife and fork, donning a t-shirt, and dialing a phone number, with item scores ranging from 0 (no hand use) to 5 (normal use). The total score is an average of all individual task items. Minimal clinically important difference (MCID) level was established to be a change score of 0.44 or greater (Fulk et al., 2017).
The Stroke Impact Scale (SIS; Duncan et al., 2003) is a stroke-specific questionnaire evaluating participation and quality of life of stroke survivors over eight domains. Each item is rated on an ordinal scale, ranging from 0 (no hand use) to 5 (normal use), and scored independently on a transformed scale, resulting in a total score between 0 and 100. The psychometric properties of the SIS have been extensively studied and established (Carod-Artal et al., 2009; Duncan et al., 2002; Edwards & O’Connell, 2003). The SIS Hand subscale (SIS–H), used for the study, had an MCID of 17.8 points or greater (Lin et al., 2010).
Procedure
Participants completed 18 sessions over 6 wk in an outpatient research lab. The duration and frequency of the intervention paralleled previous upper limb robotics protocols in the literature (Kwakkel et al., 2008). Each session was approximately 60 min and consisted of device setup, calibration of EMG levels, warm up stretching, hand training (biofeedback mode, video games), and a cool down. On average, participants spent 37.01 min per session on actual hand training. In the biofeedback mode, participants were educated on how to initiate opening or closing the hand to trigger the device. Thresholds for the EMG trigger were based on each participant’s calibration at the start of each session. A participant’s calibration was based on his or her EMG levels at rest (minimum level) and with maximum effort (maximum level).
Five video games were used: Four promoted mass extension, and one promoted mass flexion. Each game had four difficulty levels (easiest to hardest): trigger, trigger and reach, maintain, and maintain and reach. In the trigger mode, the hand device was triggered if the participant reached the EMG threshold once. In the maintain mode, the hand device was triggered when the participant maintained active muscle contraction at EMG threshold levels for 3 s. The trigger-and-reach and maintain-and-reach modes incorporated proximal shoulder reaching to different targets in combination with distal hand flexion or extension. Each participant’s training protocol was personalized. Game selection was based on the participant’s ability to successfully complete 50%–75% of trials in that mode. Game difficulty and EMG threshold levels were graded up or down to elicit the most appropriate challenge for each participant.
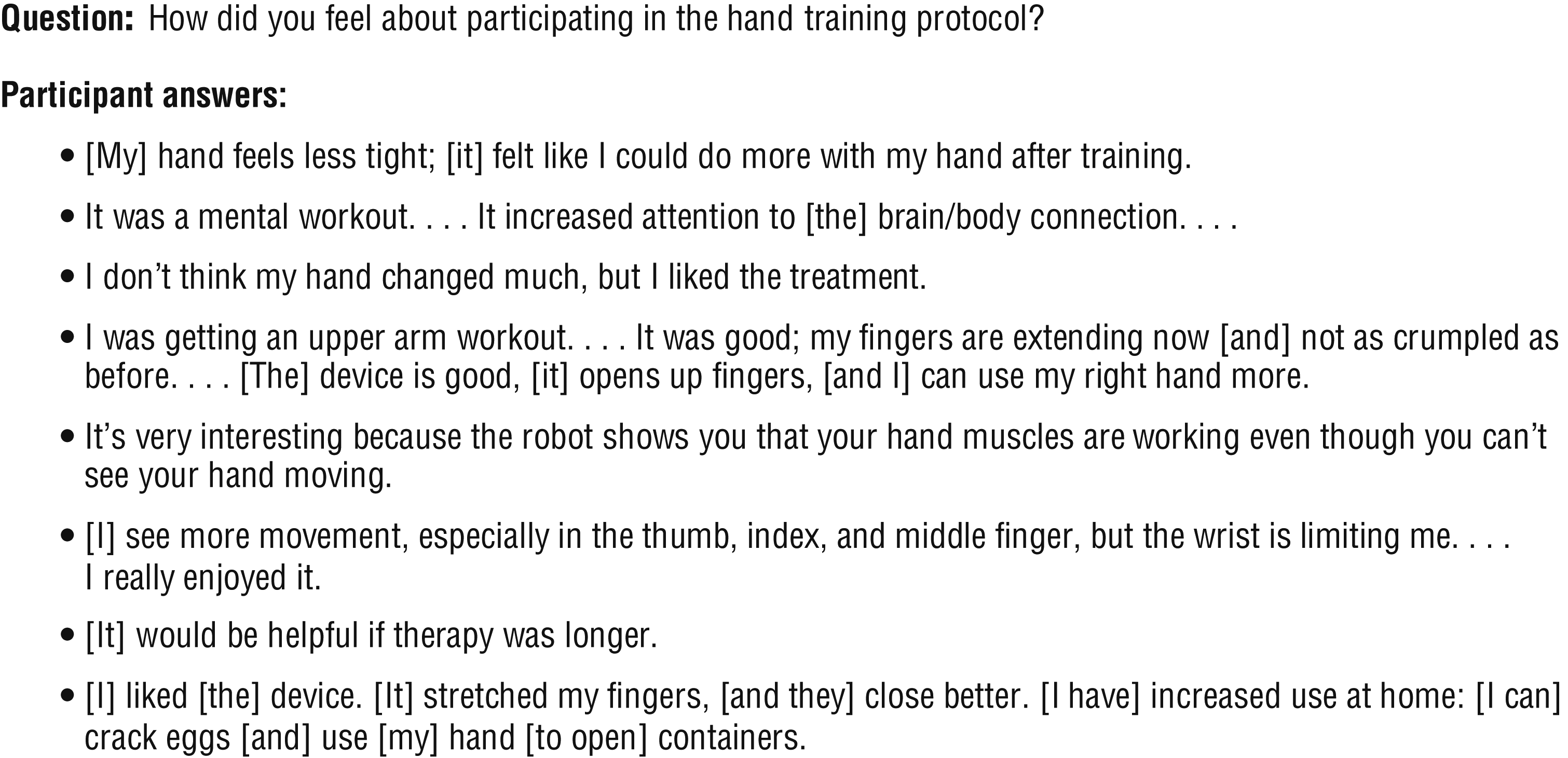
Feasibility was determined by collecting data on participants’ compliance rates, adverse events, and subjective feedback after hand training. Participants were asked an open-ended question (“How did you feel about participating in this hand training protocol?”) at the end of treatment, and responses were recorded (Figure 2).
Participant feedback on hand training.
Statistical Analysis
Descriptive statistics were used to characterize the baseline attributes of participants and outcomes at three time points. With the exception of grip strength, all of the outcomes can be considered ordinal data. The Friedman test, a nonparametric alternative to a one-way repeated-measures analysis of variance, was used to compare group means across the three time points. For outcomes with a significant main effect, post hoc pairwise testing was completed using the Wilcoxon signed-rank test. Given multiple post hoc comparisons, a Bonferroni correction was used.
Results
All participants tolerated and completed all training sessions. The most common adverse event was skin pinching or rubbing near the proximal interphalangeal (PIP) joints on the dorsal side of the hand in 58% of participants. This issue was resolved with positional adjustment of the device, padding over the PIP joint, or use of an isotoner glove to improve fit. Fifty percent of participants reported muscle fatigue at the shoulder, and 25% complained of cognitive fatigue. The fatigue resolved completely in all cases with rest between treatment sessions. We started data collection of subjective participant feedback (see Figure 2) after the start of the trial, resulting in an incomplete data set. Participation in the hand training protocol was viewed positively overall.
Table 2 summarizes group means and standard deviations at all time points and results from the Friedman test. According to initial scores, participants had moderate to severe impairment and activity limitations in the affected arm. Improvements in raw scores from baseline to discharge were seen for all outcome measures, except the SULCS. The Friedman test revealed significant main effects for the AMAT and SIS–H, χ2(2) = 8.227, p = .016, and χ2(2) = 9.707, p = .008, respectively. Post hoc pairwise comparisons indicated that participants significantly improved on the AMAT and the SIS–H from baseline to discharge and maintained these gains at follow-up. A Bonferroni correction was calculated to address multiple comparisons, resulting in a downwardly adjusted significance level of p = .017. If we applied this more stringent p value to our analysis, the results would still be significant for the AMAT (baseline to discharge, p = .013; baseline to follow-up, p = .013) and approach borderline significance for the SIS–H (baseline to follow-up, p = .019).
Outcome Measure Descriptive Statistics and Friedman Test
Note. AMAT = Arm Motor Ability Test; FMA–SE = Fugl-Meyer Assessment shoulder and elbow items; FMA–Total = Fugl-Meyer Assessment total score; FMA–WH = Fugl-Meyer Assessment wrist and hand items; M = mean; SD = standard deviation; SIS–H = Stroke Impact Scale Hand subscale; SIS–R = Stroke Impact Scale Recovery subscale; SULCS = Stroke Upper Limb Capacity Scale.
p < .05 is significant.
Discussion
Our findings indicate that EMG-triggered robotic hand training was well tolerated and safe. No study participants dropped out during treatment, and they had positive feedback about the device and training. Adverse events were reversible and related to device fit at the PIP joint. Device fit seemed to be more problematic for participants with greater spasticity in the finger flexors. The reported muscle and cognitive fatigue resolved fully with rest and could be interpreted positively as an indicator of active participation, previously described as a characteristic of robotics training. It appears to be feasible to implement the HoH device in an outpatient setting for clients with chronic stroke.
Our data reflect improvement in some, but not all, clinical measures. We found significant improvement at the activity and participation levels measured by the AMAT and SIS–H, respectively. Improvements in functional use of the affected arm were achieved at discharge and maintained over 6 wk. Four participants (30%) experienced clinically significant AMAT gains beyond the MCID levels, whereas SIS–H gains did not reach MCID levels. These results were reinforced by positive feedback from participants, including reported increased awareness of the hand and functional hand use at home. This increased awareness may be one possible explanation of why participants demonstrated improvement on activity- and participation-level outcomes at discharge and maintained those improvements at follow-up.
Participants did not achieve significant improvements on distal impairment measures specific to the treatment, such as grip strength and FMA wrist and hand items. Mean baseline upper extremity FMA scores for participants was 20.7, which borders on the moderate to severe level of arm impairment (Woodbury et al., 2013). People with less hand ability have a higher likelihood of coactivating agonist and antagonist muscles during mass flexion or mass extension movements (Chae et al., 2002; Hammond et al., 1988). The use of surface EMGs may have incidentally allowed participants with a tendency for coactivation patterns, especially during mass extension, to falsely trigger the device by general muscle activation of nearby muscles.
The biofeedback mode of the HoH addresses this issue. It provides a visual display of EMG activity on the screen and allows participants to practice isolating and activating the correct muscle group when triggering the device into mass flexion or extension. Unfortunately, there were intermittent technical difficulties with the biofeedback mode during the study, which affected 5 participants. It is possible that we did not provide adequate training in biofeedback mode for all participants, which may have contributed to our study results. Alternatively, participants may have experienced improved movement at the fingers, but our outcome measures may not have been sensitive enough to capture these changes. Finally, because of the small sample size and increased heterogeneity in clinical populations, we may have committed a Type II error.
Study Limitations
Several limitations to our study are worth noting. Although improvements in functional measures for a group with moderate to severe impairment were encouraging, increasing the sample size and including a control group would increase the validity of the findings. With no control group, we are unable to rule out that improvements were due to factors other than the robotic hand training. We did not designate primary and secondary outcome measures a priori, which lead to the statistical testing of several outcome measures and increased the chance of a Type I error.
Our results cannot be generalized to people with mild arm impairments or to those in the acute or subacute phase after stroke. The duration of each treatment session was 60 min; however, we did not control for number of repetitions completed, which can vary depending on the participant’s level of arm impairment. Finally, a direct measurable method for digit extension may be a more appropriate inclusion criteria for this type of device. Our criterion of picking up and releasing a 2.5-cm3 cube was included to demonstrate at least some active movement of the affected hand; however, participants with absent active finger extension may have been included because relaxation of the finger flexors in combination with wrist flexion can be sufficient to release a small cube.
Future Directions
The next logical step would be to conduct a larger, randomized, single blind trial using a dose-matched control group receiving conventional upper limb therapy. Based on our study results, we estimated the effect size of the AMAT by calculating Cohen’s d coefficient for dependent samples from initial to discharge time points (Cohen, 1992) and the clinically relevant improvements that participants achieved. On the basis of these two factors, we determined that the effect size is most likely in the medium effect range (d = 0.5). Using G*Power software (Faul et al., 2007), we conducted a power analysis using the AMAT as the primary outcome in an independent two-group design. Sixty-four subjects per group would be required to demonstrate an effect size of 0.50 (medium effect), with power at 0.80 and significance level at .05.
Given that data suggest better outcomes with intensive therapy early in the rehabilitation course (Krakauer et al., 2012) and the critical importance of hand function after stroke, further study of the HoH device in the acute rehabilitation hospital setting should be considered. According to our observations, participation in this type of intervention may increase use and awareness of the affected arm, which may provide longer lasting benefits when clients return home.
Implications for Occupational Therapy Practice
Our study results have the following implications for occupational therapy practice:
Robotic training may provide a viable option for people with moderate to severe arm impairment to actively participate in rigorous training of the distal hand.
It was feasible and safe to implement a robotic hand training protocol for people with moderate to severe impairment in an outpatient setting.
Participants achieved significant gains of the affected arm at the activity and participation levels after EMG-triggered robotic hand training, with 30% achieving clinically significant gains for functional tasks.
Conclusion
It was feasible and safe to implement a 6-wk hand training protocol using an EMG-triggered hand robot for people with chronic stroke in an outpatient setting. Participants with moderate to severe impairment achieved significant gains in actual and reported functional use of the affected arm, with 30% achieving clinically significant improvement on performance of functional tasks. Our study results reinforce the idea that the integration of robotic technologies can be motivating and promote active participation during treatment of clients with pronounced impairment who typically have less treatment options for the hand. Further study using an EMG-triggered hand device, such as the HoH, is warranted in a larger clinical trial.