
Abstract
The leading causes of visual impairment that affect older adults in the United States are age-related macular degeneration, diabetic retinopathy, and glaucoma (Wicker, 2015). In 2015, 3.22 million people in the United States had low vision, a number estimated to increase to 6.95 million by 2050 (Varma et al., 2016). Low vision is defined as visual acuity loss in the better-seeing eye to 20/70 or less that is not correctable by glasses, medicine, or surgery (National Eye Institute, 2015).
Low vision can significantly limit a person’s ability to perform activities of daily living (ADLs) and instrumental activities of daily living (IADLs; Crews & Campbell, 2001). Improvement in ADLs and IADLs can be realized with low vision rehabilitation (LVR; Binns et al., 2012). The extent and effectiveness of improvement of visual ability with rehabilitation has been shown to vary (Binns et al., 2012; Liu et al., 2013) depending on the outcome measures used to evaluate the client’s visual ability and the type of intervention strategies applied (Liu et al., 2013).
To be clinically meaningful, outcome tools measuring visual ability must be valid and reliable, which can be achieved by using patient-reported outcomes (Margolis et al., 2002). Some of the existing visual function questionnaires (Khadka et al., 2013; Liu et al., 2013) were developed to measure constructs of quality of life or emotional well-being rather than ADL or IADL performance. In LVR, occupational therapy practitioners focus on training clients to perform visually dependent ADLs or IADLs (Copolillo et al., 2007). Occupational therapy practitioners providing low vision services mostly rely on subjective assessments to measure outcomes (Copolillo et al., 2007). In a systematic review, Liu et al. (2013) reported that a lack of effectiveness of occupational therapy in LVR could be due to the use of outcome measures that confounded the construct of well-being with ADL or IADL performance.
Occupational therapy practitioners strive to use person-centered approaches, and the use of self-report measures can eliminate practitioner bias from the assessment process (Che Hamzah et al., 2011; Stelmack et al., 2006). Self-report measures also provide the clients’ perspective of their abilities. The Low Vision Independence Measure (LVIM) is a self-report measure that was designed to capture the clients’ perspective on difficulties they have with ADLs and IADLs affected by visual impairment.
The original 52-item LVIM (Smith, 2013) was developed by first soliciting input from a focus group of participants in an occupational therapy LVR program and the researchers involved in the study (Smith, Thomas, & Dow, 2009). The literature was also reviewed to confirm inclusion of visually dependent activities that coordinated with the Occupational Therapy Practice Framework: Domain and Process (2nd ed.; OTPF–2; American Occupational Therapy Association, 2008) at the time the LVIM was developed. (We later went through the same process with the OTPF–3; AOTA, 2014.) To be consistent with occupations named in the OTPF–2, items were divided into eight subscales (Smith, 2013).
The content validity of the LVIM was established by incorporating the recommendations of six content experts, including two optometrists practicing in LVR, two occupational therapists working with low vision clients, and two occupational therapy educators who taught low vision courses and provided rehabilitation services to low vision clients. The LVIM’s test–retest reliability was established using the Pearson product-moment coefficient of correlation, with coefficients for the eight subscales ranging from .82 to .96 (Smith, Glasson, et al., 2009). The item content of the LVIM was further modified by adding new items and rewording others for clarity based on 10 low vision therapists’ recommendations who pilot tested it with clients (Smith, 2013). Because the goal of LVR is to increase the client’s visual ability, the purpose of this study was to evaluate the measurement validity of the LVIM to measure visual ability.
Method
Study Design
A cohort design was used with data obtained at the initial evaluation of participants.
Participants
Thirteen occupational therapists working in outpatient or home health and experienced in LVR gathered data from 93 participants. Twelve collected data from participants after obtaining their informed consent with a form approved by the institutional review board. One therapist did a historical chart review to collect data. All participants met the following inclusion criteria: low vision due to an eye disease, such as but not limited to, diabetic retinopathy, age-related macular degeneration, cataract, or glaucoma; identified by the treating therapist as having good potential for rehabilitation; and a new client of the treating therapist. Participants who were currently receiving rehabilitation for any other health condition or were not fluent in English were excluded.
Instruments
Participant Trait Survey.
Data were collected on participants’ gender, age, race and ethnicity, geographic location, diagnosis, and duration of low vision condition.
Low Vision Independence Measure.
The LVIM is a self-report outcome measure designed to measure a client’s visual ability from difficulty ratings of visually dependent ADLs and IADLs (Smith, 2016). The eight LVIM subscales are based on occupations identified and named in the OTPF–3 (AOTA, 2014): self-care (eight items), food preparation (nine items), home management (six items), communication (seven items), financial management (five items), leisure (seven items), shopping (five items), and mobility (five items). The level of item difficulty for participants is rated on a 4-point ordinal scale: 1 = unable, 2 = very difficult, 3 = moderately difficult, and 4 = not difficult. If an activity is not relevant to a participant, he or she can choose “not applicable,” and the item response is not scored or is treated as missing data. LVIM administration takes approximately 15 min (Smith, Glasson, et al., 2009).
Data Collection
Occupational therapists who agreed to join the study were oriented to the procedures and provided with forms to collect data. They recruited participants from their caseload, obtained informed consent, completed the participant trait survey, and administered the LVIM.
Data Analysis
Descriptive statistics were generated for participant demographics using SAS (Cary, NC) Version 9.4. We used Mplus Version 7.4 software for factor analyses (Muthén & Muthén, 2015) and WINSTEPS Version 3.93.2 software for Rasch analysis.
Tests of Unidimensionality.
To assess the unidimensionality of the LVIM, we used confirmatory factor analysis (CFA) and principal component analysis (PCA) of Rasch residuals. Visual ability has been found to be a single theoretically constructed variable for people with low vision (Massof, 2007). We hypothesized that the LVIM is a composite variable consisting of two factors: (1) visual field or scotoma related, which affects spatial orientation, mobility, visual–motor activities, and ability to arrange and use transportation, and (2) visual acuity related, which is essential for activities that require the visual ability to discern details such as reading.
To test the two factors, we used a CFA model with a parceling approach because of a low person–item ratio (Little et al., 2002; Velozo et al., 2013). We randomly selected items for three visual field or scotoma parcels (out of 28 total items, 9 items in two parcels and 10 items in one parcel) and three visual acuity parcels (each parcel consisting of 8 of 24 total items; Table 1). The CFA factor model was estimated by the sample variance covariance matrix using the maximum likelihood method (Bentler, 1990; Hu & Bentler, 1999).
Confirmatory Factor Analysis Model Factor Loadings
Note. M = mean; SE = standard error.
The PCA of Rasch residuals was conducted to confirm the unidimensionality assumption of each measurement factor. The criteria of the PCA of response residuals being greater than 50% of the variance is explained by the Rasch model, and the first contrast in the residuals explains <5% of the variance in eigenvalue units (Linacre, 2017; Tabachnick et al., 2001).
Rasch Modeling.
We performed a Rasch analysis with the Andrich (1979) rating scale model to estimate interval measures from ordinally scaled LVIM item responses. Measurement validity was evaluated by statistically testing the hypothesis that the distribution of differences between empirical observations and the expectations of axiomatic measurement theory across observers, items, and response criteria is consistent with a single measurement variable and a single source of random disturbances in the observation of that variable (Massof, 2011).
Fit Statistics.
Once we had unidimensional factors, we examined their psychometric properties. The item fit to the Rasch model was examined using fit statistics. For the rating scale, the mean square (MnSq) fit item values should range between 0.6 and 1.4 with standardized scores (ZSTD) less than 2.0 (Wright et al., 1994).
Differential Item Functioning.
We conducted differential item functioning (DIF) tests with linearly invariant estimations (person or item) of the Rasch model (Hambleton, 1991; Reeve et al., 2007) because DIF can adversely influence the validity and reliability of measurement for between-group comparisons (Holland & Wainer, 2012; Wu, 2010). Although visual ability is affected by aging (Owsley, 2011), we hypothesized that the vision items of the LVIM do not demonstrate DIF across age groups (younger than 85 yr vs. older than 85 yr). We used the Rasch–Welch t test to examine the magnitude of DIF and to evaluate DIF contrasts (Zwick et al., 1999) based on the following criteria: greater than .64 logits for a moderate to large DIF, .43–0.64 logits for slight to moderate DIF, and less than .43 logits for negligible DIF. In addition, the significance of DIF was determined at an α value of .05 with two-sided tests (Linacre, 2017; Zwick et al., 1999).
Rating Scale Function.
We evaluated how frequently a response category was chosen and whether the response categories were ordered and increased with participants’ functional reserve. An observed count of 10 or more in each response category helps to obtain useful precision and avoid underutilization (Bond & Fox, 2007). Average functional reserve measures should increase as the frequency of the observed count increases (Bond & Fox, 2007). Outfit mean square should be less than 2.0 (Linacre, 2002).
Targeting and Reliability.
Rasch measurement can determine whether each item “fits” the singular dimension in an instrument (Bond & Fox, 2007). Both person measures (ability) and item measures (required ability) are expressed as logits in the Rasch analysis. The items should be well targeted to the distribution of participants with low vision. Separation reliability coefficients indicate the precision of variance in the distribution of measures that can be attributed to true differences between the participant and items and can be interpreted on a scale of 0 to 1 (Bond & Fox, 2007). A value close to .90 is considered high (Portney & Watkins, 2009). A reliability coefficient of .8 indicates three strata of person groups, and .9 indicates four strata of person groups (Fisher, 1992).
Results
Of the 93 participants, 27 were from Illinois, 15 from Virginia, 12 from Louisiana, 12 from Texas, 10 from Indiana, 7 from New Jersey, 5 from Oklahoma, and 5 from Pennsylvania. Participants included 68 females (73.1%) and 25 males (26.88%) between the ages of 30 and 96 (mean = 78.90, standard deviation [SD] = 12.10). The majority of participants were Non-Hispanic White (86.5%), with 5.6% Non-Hispanic Black, 5.6% Hispanic, 1.1% Asian/Pacific Islander, and 1.1% American Indian or Alaskan Native. The average length of visual impairment was 10.40 yr (SD = 12.53, range = 3 mo to 63 yr). The most frequently reported primary visual disorder diagnosis was macular degeneration (n = 59), followed by glaucoma (n = 13), visual field deficit (n = 9), other (n = 9), diabetic retinopathy (n = 2), and cataracts (n = 1).
Tests of Unidimensionality
The CFA two-factor model criteria demonstrated high factor loadings on each factor (Portney & Watkins, 2009; see Table 1) and excellent fit: root mean square error of approximation = .072, standardized root mean square residual = .034, comparative fit index = .989, and Tucker–Lewis index = .980 (Table 2). In addition, each factor structure fit the Rasch model based on the PCA of Rasch residuals. The visual field or scotoma factor explained 54.0% of the variance, with the first contrast explaining 4.8%. Similarly, the visual acuity factor explained 59.2% of the variance, with the first contrast explaining 4.1%. In addition, the consecutively smaller contrasts for each factor explained less than 5% of the variance (visual field or scotoma = 3.2%–4.2%; visual acuity = 3.3%–3.7%).
Confirmatory Factor Analysis Model Fit Criteria and Goodness of Fit
Note. CFI = comparative fit index; RMSEA = root mean square error of approximation; SRMR = standardized root mean square residual; TLI = Tucker–Lewis index.
Fit Statistics
Table 3 presents the order of item difficulty and fit statistics. The visual field or scotoma factor demonstrated four misfit items—SC1 Shaving or applying makeup (infit MnSq = 2.15, outfit MnSq = 2.15), SC2 Identifying toiletries (infit MnSq = 1.43, outfit MnSq = 1.99), HM23 Repairing clothing (infit MnSq = 1.68, outfit MnSq = 1.99), and MO48 Using the stairs (infit MnSq = 1.47, outfit MnSq = 1.55)—with greater than 2.0 ZSTD for these items. The visual acuity factor demonstrated two misfit items—CO24 Requesting assistance (infit MnSq = 2.15, and outfit MnSq = 3.35) and CO28 Determining the time (infit MnSq = 1.91, outfit MnSq = 1.58)—with greater than 2.0 ZSTD for these items. When we removed these misfit items from each factor, all remaining items of the now revised LVIM fit the Rasch model.
Fit Statistics, Item Difficulty Hierarchy, and DIF of the Visual Field/Scotoma and Visual Acuity Domain
Note. A higher measure (Logits) indicates a more difficult task; df = degree of freedom; DIF = differential item functioning; M = mean; MnSq = mean square; SD = standard deviation; SE = standard error; ZSTD = standardized score; — = not applicable.
Differential Item Functioning
Table 3 presents the DIF analysis results. The two factors demonstrated no DIF across age groups (less than 85 yr, n = 28, vs. greater than 85 yr, n = 51). Although six items of the visual field or scotoma factor and five items of the visual acuity factor demonstrated moderate to large DIF, the DIF contrasts were not statistically significant (all ps > .05).
Rating Scale Function
The two factors had observed counts in each response category exceeding 10. Average functional reserve measures were shown to increase consecutively from –0.99 to 2.40 for the visual field or scotoma factor and from –1.74 to 2.01 for the visual acuity factor in the response categories, indicating that the thresholds are ordered. The outfit MnSq for all categories was close to 1 (less than 2.0) in the two factors, indicating that the observed responses for the LVIM were close to the response expected by the Andrich model.
Targeting and Reliability
A person and item map compares person and item measure distributions (Figure 1), and Table 3 presents the item difficulty hierarchy of the two factors. In the visual field or scotoma factor, the most challenging items were FP9 Reading recipes (2.07 logits) and MO49 Crossing streets (0.88 logits), and the easiest items were SC3 Brushing teeth or cleaning dentures (–1.85 logits) and HM20 Washing dishes (–1.28 logits). In the visual acuity factor, the most challenging items were LE38 Reading books, newspapers, magazines (1.60 logits) and SH46 Determining expiration dates (1.50 logits), and the easiest items were SH47 Paying for items (–1.32 logits) and FM31 Identifying coins and paper money (–1.19 logits).
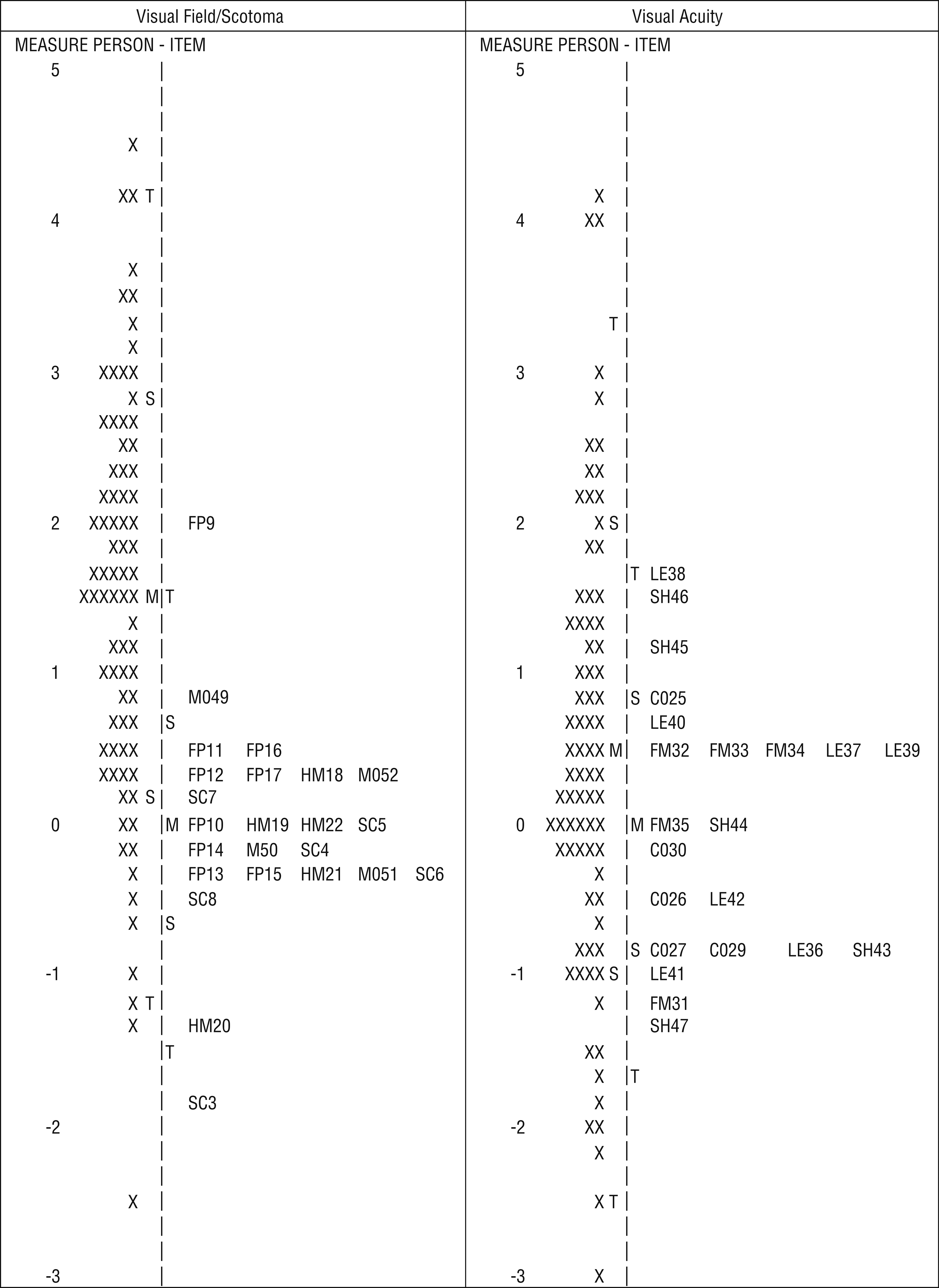
Person and item map for the visual field/scotoma (left) and visual acuity (right) domains.
Although the visual field or scotoma factor had a mismatch between the mean of person measures (1.48 logits, SD = 1.35) and the mean of item difficulties (0.00 logits, SD = 0.71), person measures had a high separation reliability (R 2 = .87; i.e., 87% of the observed variance represents real differences in ability between people, and 13% can be attributed to estimation error) and a high person strata value (3.91, indicating four distinct measurement groups in the sample). In the visual acuity factor, the gap between the mean of person measures (0.46 logits, SD = 1.46) and the mean of item difficulties (0.00 logits, SD = 0.85) was less than 0.50 logits, with a high person reliability of .90 and a high person strata value of 4.40. In addition, the two factors had no high ceiling or floor effects.
Discussion
The purpose of this study was to evaluate the measurement validity of the LVIM using Rasch analysis and factor analysis for unidimensionality, rating scale function, and targeting and reliability. When the four misfit items are dropped from the visual field or scotoma factor and the two misfit items were dropped from the visual acuity factor, the revised LVIM has good psychometric properties (item fit, DIF, rating scale function, precision, and reliability). Its rating scales appropriately measure visual ability with no collapsing of categories necessary because the category thresholds were ordered and increased in an expected order. The reliability and person strata of the two factors demonstrated overall measurement precision, with the two factors demonstrating high person measure separation reliability coefficients. Moreover, the revised LVIM can estimate stable visual ability (visual field or scotoma and visual acuity) across the age groups on the DIF test.
The issue of visual ability consisting of two factors has face validity because occupational performance of vision-dependent ADLs and IADLs is aided by both visual fields (peripheral vision) and visual acuity (central vision). The construct of visual ability consisting of two measurement factors found in this study is supported by previous studies on visual function questionnaires. For instance, Massof et al. (2007) examined the Activity Inventory and concluded that visual ability is a composite variable with at least two dimensions: mobility and reading. Stelmack et al. (2007), following a Rasch analysis on the Veterans Affairs Low Vision Visual Functioning Questionnaire–48, came to the same conclusion. In addition, Velozo et al. (2013) investigated the construct of the Self-Report Assessment of Functional Vision Performance and determined that the CFA confirmed two dimensions of reading and mobility.
Most items of the original LVIM (46 of 52 items) met the Rasch model. Items that misfit the Rasch measurement model may require additional skills, such as cognition to complete the activities described in the items, whereas other items such as shaving or applying makeup may have been too easy for our participants.
Study limitations include the small sample size for the factor analysis and Rasch modeling and to evaluate DIF. The sample was relatively homogeneous (mainly White females). We expect that item measure precision and DIF results could be improved by increasing the participant sample size. Future research should be done with larger samples to validate results and longitudinally to measure the responsiveness of the revised LVIM to LVR.
Implications for Occupational Therapy Practice
This study has the following implications for occupational therapy practice:
The eight subscales of the LVIM align with occupations named in the OTPF–3 (AOTA, 2014).
Subscale items are tasks or activities required to perform subscale occupations.
The revised 46-item LVIM is a valid measure of occupational therapy outcomes.
Conclusion
The LVIM was developed to measure outcomes of interventions routinely addressed in LVR. The revised LVIM can be used as a reliable and valid outcome measure in LVR.
Footnotes
Acknowledgments
We thank Robert W. Massof for his valuable suggestions for the final article.