
Abstract
Falls are undeniably a significant public health concern. Although people at risk for falls are often identified using one set of criteria, recent research has highlighted differences in risk factors for indoor and outdoor falls. Contrary to indoor falls, predictors of outdoor falls include male gender, younger age, high levels of leisure time physical activity, and a fast gait speed (Kelsey et al., 2010; Li et al., 2006). Outdoor falls are just as likely to result in serious injuries as indoor falls, with a resulting loss of function (Kelsey et al., 2012), and therefore warrant equal attention in clinical practice.
To date, fall prevention programs have largely focused on risk factors for indoor falls and have included elements such as exercises to improve balance and strength and home modifications (Kelsey et al., 2012; Li et al., 2006). Evidence-based programs that prevent falls, increase falls self-efficacy, or both include Otago, an exercise program (Thomas et al., 2010), and multifactorial programs that address indoor risks and some outdoor risks, such as Matter of Balance (Tennstedt et al., 1998) and Stepping On (Clemson et al., 2004). Although risks for indoor falls are actively addressed with training and home modifications (Chase et al., 2012), outdoor falls are more likely to be precipitated by environmental causes (Li et al., 2006). To fill this gap, the development of an effective outdoor fall prevention program is warranted.
Common locations of outdoor falls include streets, curbs, sidewalks, parks, and parking lots (Kelsey et al., 2012; Nyman et al., 2013). Stairway falls are also common and are associated with a disproportionate risk of serious injury and death (Jacobs, 2016). Identified causes of outdoor falls include physical conditions of the neighborhood environment, such as uneven surfaces (Bergland et al., 2003; Li et al., 2006). Although walking is the most common activity performed at the time of an outdoor fall, other activities include getting in or out of a car, opening and closing doors, carrying items on level and uneven surfaces, and vigorous physical activity (Chippendale & Raveis, 2017; Kelsey et al., 2012). Outdoor falls have also been attributed to behaviors such as rushing, overexertion, and wearing multifocal lenses (Chippendale & Raveis, 2017; Lord et al., 2002; Nyman et al., 2013).
In addition to studies that highlight cause and location of outdoor falls, a recent survey of older adults in one U.S. city examined knowledge of outdoor fall risks and strategies used for outdoor fall prevention. Results revealed several unmet educational and training needs. For example, fewer than 30% of respondents identified recreational areas as locations that pose risks, and more than 40% felt that stairs did not increase their risk of falls (Chippendale & Raveis, 2017).
To fill the gap in knowledge and practice regarding outdoor fall prevention, the Stroll Safe program was developed. The purpose of this study was to assess the feasibility of the program and to use the findings to plan a larger scale study. A feasible program was determined by the successful recruitment (100%) and retention of the majority of participants (75% or more), no adverse events, and predominantly positive feedback from program participants.
The overarching framework that guided the development of the Stroll Safe program is the Ecological Perspective (National Cancer Institute [NCI], 2005). Outdoor fall prevention is related to multiple levels of influence, including intrapersonal (e.g., knowledge, beliefs), interpersonal (e.g., peers), and community-level (e.g., neighborhood features) factors. The content and delivery of the program also draws from the Health Belief Model (NCI, 2005) to promote changes at the individual level.
Method
Design
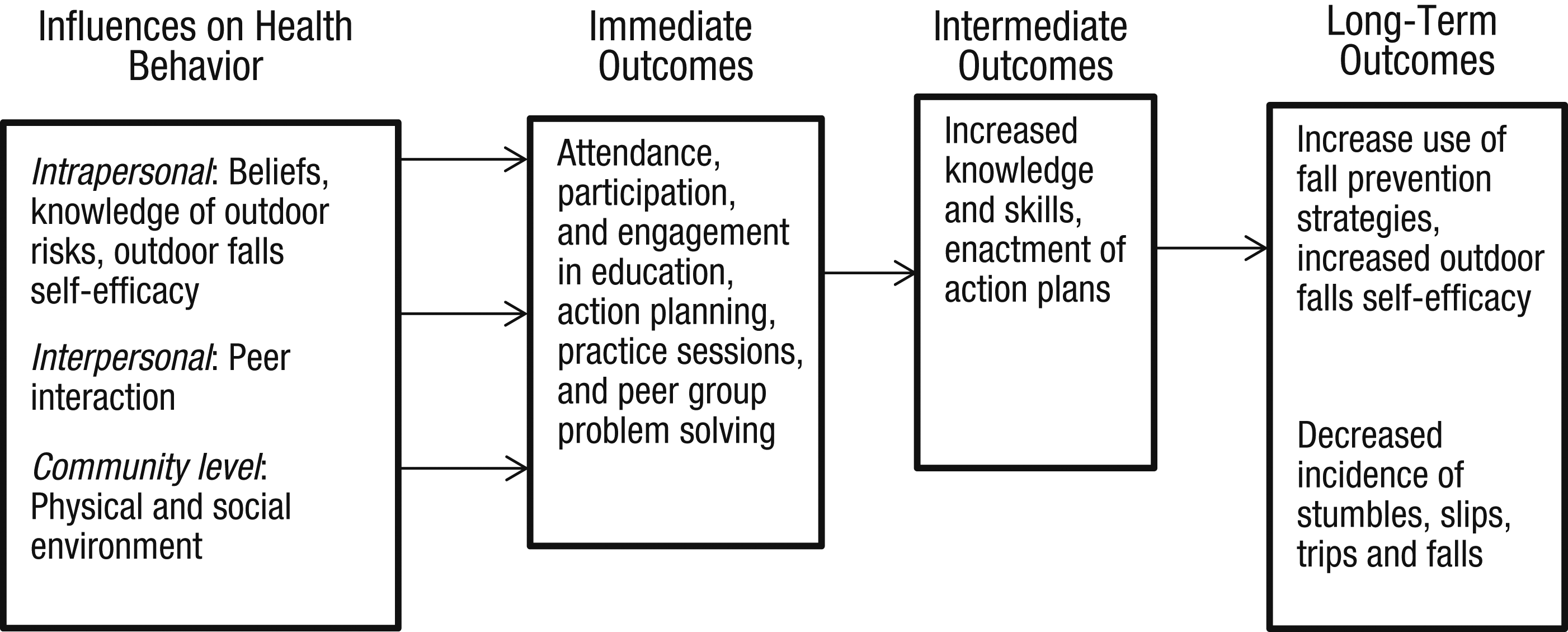
A quasi-experimental control group design was used (N = 24). Consistent with Tickle-Degnen’s (2013) suggested guidelines, a process, resource, scientific, and management assessment was conducted. Whereas the Ecological Perspective (NCI, 2005) and the Health Belief Model (NCI, 2005) were used to inform the intervention itself, Program Theory (Funnell & Rogers, 2011) was used to organize the process evaluation. Figure 1 depicts expected outcomes at each stage of the program.
Process evaluation.
Participants
Inclusion criteria were age 55 yr or older; English speaking; cognitively competent (Montreal Cognitive Assessment [Nasreddine et al., 2005] score > 24); able to ambulate outdoors independently with or without an assistive device; able to travel independently to the program site; and have sustained a trip, slip, stumble, or fall outdoors in the past year. Adults with an acute health condition that would interfere with participation in the program (e.g., recent fracture, untreated mental illness) were excluded.
Analyses
Feasibility was assessed quantitatively using retention rates and attendance records and qualitatively using a fidelity assessment, reflective log, and an audio-recorded focus group. The scientific assessment included descriptive statistics to examine participant characteristics and to explore trends pertaining to changes in strategy use; number of trips, slips, and falls; and level of concern about falling from baseline to program completion and at a 2-mo follow-up. Cohen’s d was calculated to ascertain effect sizes. The transcribed focus group was analyzed by extracting significant statements that pertained to program strengths, limitations, and suggestions for improvement. Both the principal investigator and a research assistant analyzed the transcript, and agreement was found between the coders.
Procedure
The study was approved by New York University’s internal review board. Participants were recruited using a two-pronged approach: contacting participants from a prior study and notifying elders from one senior center and one naturally occurring retirement community program site using announcements and flyers. Interested participants were given the choice of receiving written information only in the form of an investigator-developed brochure on outdoor fall risks and strategies to prevent falls (control group) or attending the Stroll Safe program (treatment group). The maximum number of participants for the Stroll Safe program was set at 12. Once the treatment group was full, participants were assigned to the control group.
After giving informed consent, participants completed the cognitive screening. If eligible, participants completed the pretest questionnaires. Participants in both groups were given a monthly calendar with the Stroll Safe logo and stumble, slip, trip, or fall printed at the top, which served as a prompt. Participants were asked to record any stumbles, trips, slips, or falls they experienced outdoors from enrollment through 2 mo after program completion. This information was collected by phone every 2 wk.
At the end of the Stroll Safe program, and then 2 mo after program completion, posttests were administered by trained research assistants. Participants in the treatment group also participated in a focus group, which was led by the principal investigator and took place immediately following the final session of the 7-wk program.
Overview of Stroll Safe
The content of the once a week, 7-wk outdoor fall prevention program is based on the Ecological Perspective (NCI, 2005) and Health Belief Model (NCI, 2005) frameworks; the results of a survey of older adults in one U.S city, which identified gaps in knowledge and use of prevention strategies; and the related literature on outdoor falls (Chippendale & Raveis, 2017; Kelsey et al., 2012; Li et al., 2006; Nyman et al., 2013). The program manual includes preset modules; however, participants were able to voice individual concerns and problem solve solutions during group discussions.
The organizational structure of the program mirrors the evidenced-based Lifestyle Re-Design® program (Clark et al., 2012). Sessions 1, 2, 4, and 5 covered four modules (i.e., one module each week):
Module 1: The built environment: navigating curbs, parking lots, brick/cobbled surfaces, and stairs
Module 2: The social environment: addressing the behavior of drivers, cyclists, and other pedestrians
Module 3: Neighborhood conditions: navigating poor street/sidewalk conditions, icy surfaces and weather conditions, and obstructions
Module 4: Personal factors: overexertion, gait speed, eyewear, and alcohol use.
Each 90-min session included a brief didactic presentation about outdoor fall risks and strategy use by the group leader (i.e., the principal investigator), an occupational therapist. This presentation was followed by group discussion and problem solving regarding outdoor fall risks identified by participants and the group leader. Identified strategies were recorded on a white board and transcribed to create handouts. Each session ended with action planning, during which participants wrote down behavioral changes they will implement in the coming week. Sessions 3 and 6 included outdoor mobility training and practice using strategies covered in the modules. Session 7 (the final one) was a review.
Measures
Fidelity Checklist and Attendance Records.
Attendance was recorded at each session. A fidelity checklist was created, and a trained research assistant listened to each audio-recorded session to assess
Inclusion of key topics in the manual
Reasonable pace and omission of jargon
Active participation and engagement by group members
Balance between information sharing and group discussion, with stronger emphasis on group discussion
Participants’ descriptions of the development and enactment of action plans.
Participant Feedback.
An audio-recorded focus group consisting of treatment group participants provided the opportunity for participants to discuss program strengths and areas for improvement, provide suggestions for content changes, and evaluate the attribution of any behavioral changes to the Stroll Safe program.
Outcome Measures.
Preliminary outcomes were examined using the Falls Self-Efficacy Scale–International (FES–I; Yardley et al., 2005), the Outdoor Falls Questionnaire (OFQ; Chippendale, 2015), and the Falls Behavioral Scale for the Older Person (FaB; Clemson et al., 2003b). Stumbles, trips, slips, and falls were tracked using fall diaries.
Among community-dwelling seniors, the FES–I, which measures concern about falling during several activities, has been shown to have good reliability and validity (Yardley et al., 2005). Scores on the FES–I range from 16 to 64, with a higher score indicating a greater level of concern about falls.
The OFQ is a valid measure of outdoor fall risks and prevention strategies. It has strong internal consistency and test–retest reliability, and it includes demographic information regarding outdoor falls (Chippendale, 2015). The Strategy Use subscale score for the OFQ, used as an outcome measure in this study, has a range of 0–36, with a higher score indicating greater strategy use. The OFQ also includes the Patient Health Questionnaire–2, a two-item measure of depressive symptoms (Kroenke et al., 2003).
The 24-item version of the FaB is a robust and valid measure of protective behaviors used by community-dwelling older adults to prevent falls (Clemson et al., 2003a). As per scoring guidelines suggested by Clemson et al. (2003b), mean scores (range = 1–4, with a higher score indicating the safest behaviors) rather than raw scores were used.
Results
Process Assessment
Approximately 8 wk was needed to recruit 24 participants. Effective recruitment strategies included making an announcement at community sites and then sitting at a table to enable people to ask questions and make appointments to enroll. There were several word-of-mouth referrals, primarily friends who then attended the program together. One interested senior was screened out as a result of an acute fracture, but no potential participants were screened out because of cognitive impairment.
The retention rate was 83%. One participant in the treatment group missed the first session and then dropped out before the second session because of too many prior commitments. Two control group participants were lost to follow-up before the first posttest; 1 dropped out after Week 5 of the program, and the other dropped out after Week 7. Another control group participant completed the pretest and all fall calendar reports but chose not to complete the two posttests. Program attendance for the remaining 11 treatment group participants ranged from four to seven sessions. The majority of participants (82%) attended five or more sessions. The final session was a review session, and all 11 participants attended.
According to the fidelity assessment, the majority of participants were actively engaged in the group sessions, although some were more vocal than others. All of the key topics were covered per the treatment manual. The first session had a stronger focus on information sharing by the group leader. However, subsequent sessions were more balanced between information sharing and group discussion. Each participant was treated like an expert. Some jargon was used by the group leader (e.g., range of motion, acute problem); however, participants asked for clarification as needed. Participants described the strategies that they implemented outside of the sessions. In summary, immediate and intermediate outcomes were achieved (see Figure 1).
Program participants believed the program was valuable. In particular, they believed training in correct use of mobility aids, safe stair-climbing strategies, how to fall safely, and navigating public transit safely was helpful. Instruction in selecting appropriate footwear, use of Yaktrax (Durham, NC; a footwear modification device for snowy or icy conditions), and visual scanning techniques were other identified program strengths. Another identified program strength was that the group sessions had a positive, open atmosphere where people felt comfortable sharing their concerns and ideas and everyone had an opportunity to participate. Participants described being more aware of their surroundings and paying attention more consistently as a result of the program.
Suggestions for program improvement included more discussion about health care services available for health concerns related to fall risk, more training on how to use a mobility device effectively on level surfaces, and less time devoted to filling in the online form to report a problem to the city. Navigating public transit safely and identifying windy locations (e.g., wind tunnels) were concerns shared by several study participants; therefore, these topics may warrant greater attention. Long-term outcomes, including an increase in use of strategies and a decrease in trips, slips, and falls, were realized (see Scientific Assessment section). Consistent with the process assessment depicted in Figure 1, alignment of immediate, intermediate, and long-term outcomes was achieved.
Resource and Management Assessment
Effective quality control measures for research assistants included evaluating their attention to detail regarding accurate data management and listening in on their first few data collection calls. Adding more detail in the treatment manual for community practice sessions and adding specifications for room setup and equipment needs for each module (e.g., floor mat, Yaktrax, foot stool) should facilitate program replication.
For outdoor mobility training, having two occupational therapists for 10–11 participants was the upper limit of what was feasible for therapist-to-participant ratio. Moreover, using experienced therapists who could adapt the training sessions for participants with varying levels of functional mobility and endurance was essential. Calling participants on different weekdays and in the morning and late afternoon was best for reaching them for fall calendar reports. Contamination may have taken place because participants from the senior center described instructing their friends in outdoor fall prevention strategies, some of whom may have been participants in the control group.
Scientific Assessment
There were no adverse events, and the sessions were tolerated well by participants. Characteristics of participants in the treatment and control groups (Table 1) were similar, although the control group was on average older than the treatment group.
Participant Characteristics
Note. ADLs = activities of daily living; IADLs = instrumental activities of daily living; M = mean; PHQ–2 = Patient Health Questionnaire–2; SD = standard deviation.
Strategy use increased for both the treatment and control groups from baseline to the end of the 7-wk program; however, the increase was greater for the Stroll Safe participants (Table 2). In addition, the increase in strategy use scores was maintained at the 2-mo follow-up. Note that this increase occurred even though some strategies covered in the program (e.g., walk now, talk later; how to fall safely) were not captured by the outcome measures used. Total FES–I scores increased slightly for both groups. However, for the question pertaining to level of concern walking around the neighborhood, average score decreased for the treatment group and increased slightly in the control group (see Table 2). Results of the fall calendar reports are presented in Figure 2. A decrease in mean number of stumbles, trips, slips, and falls for both groups is noted, but the decrease was greater for the Stroll Safe program participants.
Comparison of Strategy Use and Level of Concern About Outdoor Falls Scores Between Groups
Note. FaB = Falls Behavioral Scale for the Older Person; FES–I = Falls Self-Efficacy Scale–International; M = mean; OFQ = Outdoor Falls Questionnaire; SD = standard deviation. Time 1 is baseline, Time 2 is at end of 7-wk program, and Time 3 is at 2-mo follow-up.
Level of concern walking around the neighborhood.
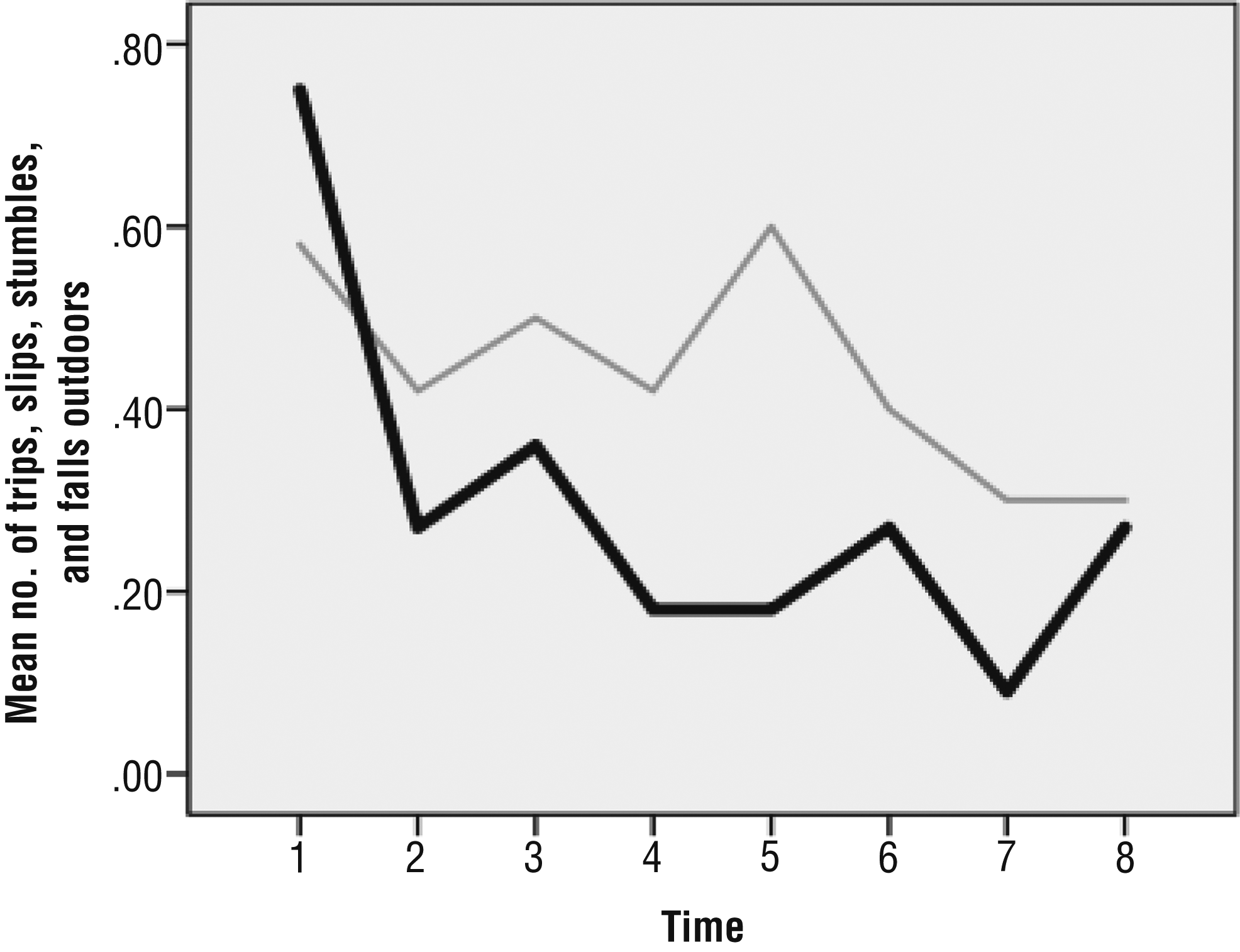
Mean number of outdoor trips, slips, stumbles, and falls for the treatment and control groups.
Discussion
According to the quantitative and qualitative findings, including the successful recruitment (100%) and retention of the majority of participants (83%), a lack of any adverse events, and the predominantly positive participant feedback, the Stroll Safe program appears to be feasible to implement among active, community-dwelling older adults. Feedback was obtained to refine the program and research methodology for a larger study, including considerations for hiring and training of research assistants, staffing, choice of measures, and content of the manual.
Several participants expressed concern about navigation of public transit. Although this activity does not occur exclusively outdoors, it is an important aspect of community mobility and therefore warrants greater attention in the program. Appropriate use of mobility devices on level surfaces as opposed to stairs alone is another needed program addition according to participant feedback and a recent study concluding that a lack of training in proper use of mobility devices is common among older adults (Luz et al., 2017).
The measures selected for this study did not capture some of the prevention strategies addressed in the program. Moreover, several of these strategies were identified as the most helpful components of the program; therefore, additional questions and measures are warranted in a follow-up study to capture full program benefits. A possible addition is the Falls Prevention and Management Questionnaire (Finlayson et al., 2009), which captures additional aspects of fall prevention knowledge. The measures we used were all self-report; therefore, performance-based measures also warrant consideration in future studies.
There appears to be a risk of contamination within sites. Therefore, randomization of sites rather than participants may be most appropriate for a larger scale study. In addition, an increase in the amount of the incentives as the study progresses may help to decrease attrition.
Although the total score for level of concern about falling as measured on the FES–I went up slightly in both groups, level of concern walking around the neighborhood specifically went down slightly for the treatment group but not for the control group. It is possible that an increase in knowledge of hazards increased level of concern about falls. A stronger emphasis on practice of strategies to increase self-efficacy may be needed to counterbalance increased awareness of risks. Although high levels of concern about falls can lead to negative consequences such as decreased activity levels (Liu, 2015), some concern can result in increased attention to fall hazards (Twibell et al., 2015).
The program sessions took place in the lab space at New York University, and several participants commuted for up to an hour. Given the importance of context, and changes in life-space mobility with age (Rantakokko et al., 2016), offering the program in participants’ community of residence is warranted.
Implications for Occupational Therapy Practice
The results of this study have the following implications for occupational therapy practice:
Outdoor fall prevention warrants attention in clinical practice.
The Stroll Safe program warrants further study.
Conclusion
Stroll Safe is a novel program for outdoor fall prevention. Preliminary results reveal program benefits. Findings from this study can be used to modify the program and study methodology to plan a larger scale study.