
Abstract
Eating is a uniquely social and cultural experience. The varied ways different cultures eat largely determine the diets of young children in those cultures. As Segal (2014) described it, food is a vehicle for many nonbiological functions with symbolic social and economic meanings. For mothers and fathers, feeding is an opportunity to exercise their parental roles. The family is the first and most fundamental socioenvironmental context in which children establish their eating patterns. Parents influence eating through their child-feeding strategies. They select the family diet, model eating behavior, and provide direct instruction on when, where, and how to eat (Anderson et al., 2005; Johnson & Birch, 1994). These child-feeding strategies often occur within a conditioned cultural context (Heaton et al., 2005). Awareness of clients’ cultural practices and habits is necessary for occupational therapy practitioners to design and implement effective feeding intervention strategies.
People of Latino origin are the largest ethnic minority in the United States. According to the National Vital Statistics Report on U.S. births (Hamilton et al., 2016), 23% of U.S. resident births in 2015 were among Latino-origin groups. In this study, the term Latino-American describes a person living in the United States who identifies racially or ethnically as Latino or who racially or ethnically identifies with people from Mexico, Central America, South America, or the Caribbean (Rivera et al., 2010). This broad definition of Latino-American recognizes and honors the diverse ethnic and racial experiences of Latino-Americans.
There is a pressing need for health professionals to better understand feeding practices in this population from a broader cultural perspective. Limited data are available on the feeding practices of Latino-Americans. Most studies have focused on parental behaviors known to influence early childhood weight issues (Crawford et al., 2004; Martinez et al., 2014). Some studies reported Latino-American mothers as tending to promote hearty, high-calorie meals so that children can become “big and strong” (Cartagena et al., 2015; Garcia, 2004; Lindsay et al., 2011). Other studies reported Latino-American mothers as being more likely to be indulgent in feeding practices, making few rules for or demands on children (Chaidez et al., 2011). These diverse findings could be a result of the diversity of Latino-American culture (Brotanek et al., 2009; Bryant, 1982; Bunik et al., 2006).
Our goal was to better understand feeding behaviors and attitudes of Latino-American mothers of young children. This study’s primary objective was to gather information to identify and describe common cultural beliefs that influenced feeding practices of a small group of Latino-American mothers with young children in the greater New York metropolitan area. Further, we explored the sources of recommendations they received on how, what, and when to feed their young children.
Method
Design and Procedures
We used grounded theory to understand participants’ perspectives on feeding their young children (Bogdan & Biklen, 2007; Corbin & Strauss, 2015; Creswell, 1998). Under supervision from two authors (Tsu-Hsin Howe and Jim Hinojosa), second-year graduate students collected data using open-ended, semistructured, in-depth, face-to-face interviews (Kvale, 1996; Spradley, 2016). Before data collection, the students engaged in a research seminar that included training in interviewing techniques and cultural considerations. They were given a list of topics and suggested open-ended questions related to the objectives of the research so they could incorporate them into interviews. The primary interview questions were as follows: “What are your daily feeding routines?” “How does your cultural upbringing influence your feeding practices?” “What do you like or find most challenging about feeding your child(ren)?” “How do you decide how, when, and what to feed your child(ren)?” This interview guide ensured that the same general areas of information were covered in each interview while allowing interviewers a degree of freedom and adaptability (Turner, 2010).
Interviews were conducted in English at participants’ homes at a time convenient for each family. Each interview lasted about 1 hr, and each participant was interviewed twice over a period of 1 mo. All interviews were audio recorded. Interviewers took abbreviated field notes about the context and participants’ body language. During data collection, the interviewers met with investigators (Howe and Hinojosa) weekly to review the interview process, receive feedback on interview techniques, and reflect on potential biases.
Participants
Participants were recruited using snowball sampling. The graduate student interviewers initially contacted two acquaintances each about participating in the study. They asked these contacts whether they knew other potential participants, who were, in turn, asked whether they knew potential participants, and so forth. Sampling stopped when 12 Latino-American mothers agreed to participate. To participate in the study, potential participants were required to self-describe as Latino-American, have at least one child younger than age 5 yr, be able to communicate well in English, and be willing to share their feeding experiences. Child younger than age 5 yr was used as the cutoff for recruitment because we believe children’s feeding behaviors are influenced most by their parents during the earliest stages of development. The Institutional Human Research Ethics Committee of New York University provided permission to conduct the study.
Trustworthiness and Methodological Integrity
Steps were taken to ensure trustworthiness and account for potential researcher bias. As part of the course assignment, graduate student interviewers were required to explicitly state their biases and beliefs about Latino-Americans. A discussion of these biases highlighted their views about their own ethnic background and about Latino-American culture. Open discussions of the interviewers’ perceptions of participants were an essential part of data collection. One of the researchers (Hinojosa) had a Latino-American background and oversaw the data collection process to ensure that information was not misinterpreted or lost.
After data were collected and transcribed, we asked participating families to review the transcripts and provide feedback. We also shared with participants the themes we developed and solicited their reactions. Although it is almost impossible to mask all researcher bias, we consciously considered the effects of our prejudices and worldviews. Further, the research was conducted in accordance with the protocol approved by the institutional review board, and all participants provided informed consent before the interviews began.
Data Analysis
Interview observation notes, audio recordings, and transcriptions were analyzed. Data included child-feeding tactics, habits, and routines, as well as the families’ general feeding experiences. Four transcripts were reviewed to ensure consistency with the corresponding audio recordings. The qualitative data analysis software ATLAS.ti Version 6.2 (Scientific Software Development, Berlin, Germany) was used for coding, text retrieval, data management, and content analysis. Coding qualitative data involves labeling units of data (lines, sentences, or paragraphs) and aggregating units into categories. Themes generated from the original study questions were used as categories (Hannon et al., 2000). Major themes emerged after abstraction and logical analysis.
Authors Howe and Hinojosa independently reviewed the data to code and identify major categories and then reviewed coding agreements and disagreements to reach a consensus, thus increasing the reliability of study findings. After discussing discrepancies in coding and categorization, the authors identified or redefined category definitions. In summarizing the data in this article, we use participants’ exact words when possible. In addition, we present disconfirming evidence—that is, the data not consistent with the theme we defined—as a means of increasing credibility (Creswell & Miller, 2000).
After completion of thematic analyses, all interview data were combined into one file. From this file, a word cloud was created to visualize the frequency of words used in the interview responses (Figure 1). Words representing food groups (starch, fruits, vegetables, meat) were then added to the actual interview words in an attempt to show the frequency of mention of various foods. The more frequently a word was used in the interview responses, the larger the word appears in the word cloud. Figure 2 represents the frequency of words extracted from the interviews.
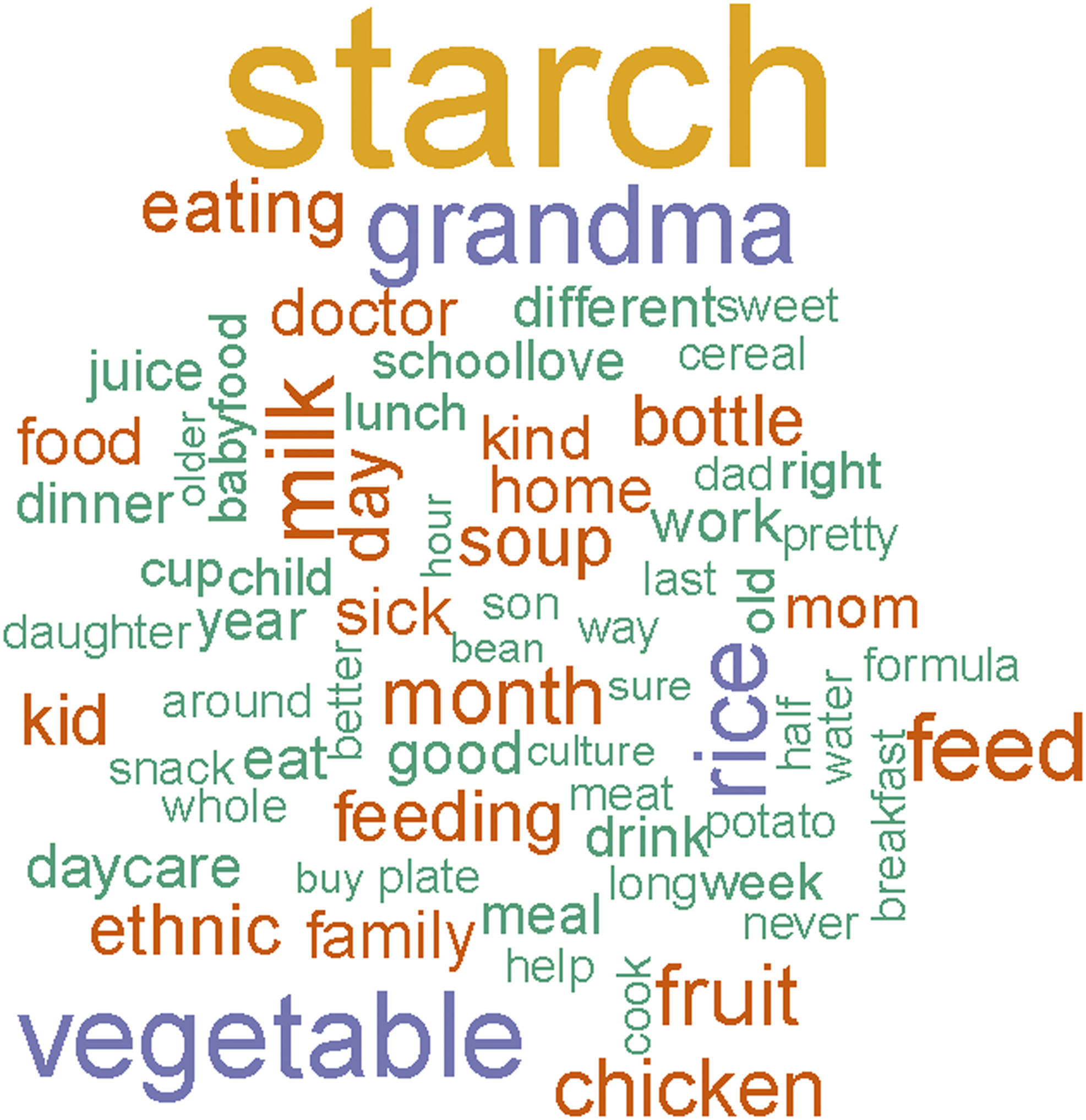
Word cloud: Visualization of word frequency in interview responses.
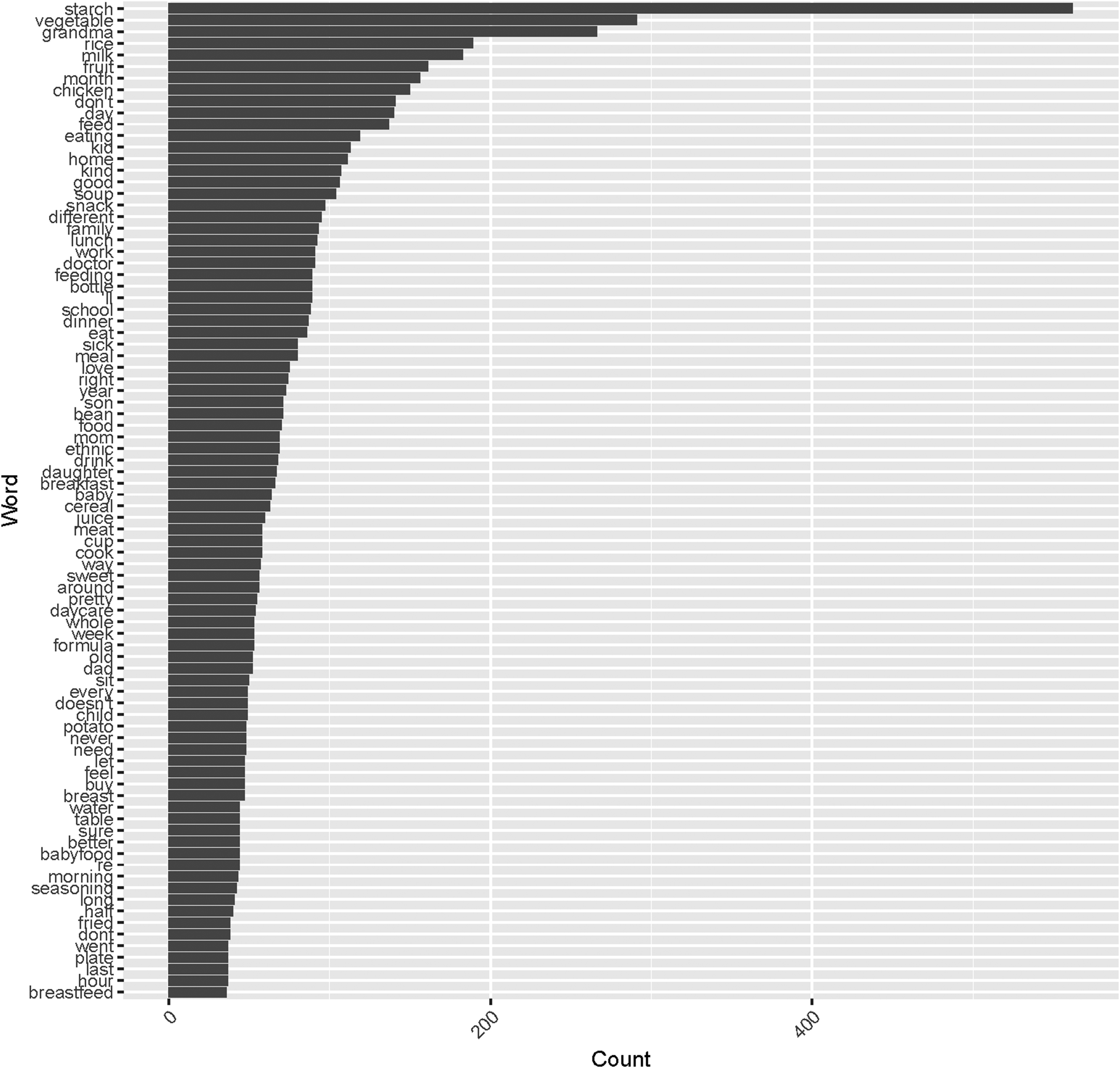
Words used in interview responses, by frequency.
Results
Table 1 provides detailed background information on the 12 participating families. Nine were two-parent families and 3 were single-parent families. Only 1 family lived with extended family; the rest lived in nuclear family households. Children of 5 families attended day care on weekdays, five children were cared for by their grandmothers, and three children stayed home with their mothers. All mothers except one held a full-time or part-time job outside the home.
Cultural Background of Participating Families
Interview content included feeding practices and habits and the recommendations mothers considered when feeding their young children. Four major themes emerged from the interviews. The first theme, “Grandma knows best,” relates to decisions about food progression—determining what foods and when and how to introduce them to their young children. The second theme, “I want my child(ren) to be healthy,” addresses the mothers’ beliefs about health and healthy food. The third theme, “always soup and always rice,” relates to the food choices mothers made for their children, including preparation methods (e.g., store-bought vs. homemade, seasonings, ingredients). The fourth theme, “mealtime is family time,” reveals the mothers’ perceptions of the value of mealtimes.
Theme 1: “Grandma Knows Best”
Most participants identified their mothers as the first person they contacted when seeking advice about feeding their children. Some participants shared, “Grandma knows the best,” “She’s just kinda watching out for her,” and “Who else to give you the best advice than your own mother?” When participants were asked who decided when, what, and how to feed their children, 2 responded, “It was my mom—it was all my mom” and “Grandma tell me when she thinks I need to give my babies food, and Grandma tell me what to feed them.”
When asked about seeking advice from doctors about feeding, 2 mothers responded, “No doctors; they scare the crap out of you about everything” and “We try Mom’s old-school remedies; if doesn’t work, we resort to the doctors.” The participants tended to second-guess or disregard medical advice. For example, 1 participant shared, “They [the doctors] told me not to give him water before 1 year old, but I gave him chamomile tea anyway.”
When faced with conflicting recommendations from physicians and family, the mothers tended to rely on their family’s advice. As 1 mother summarized,
I [would] really rather get information from my mother. The doctor doesn’t always say everything. They always tell you to avoid certain things but not everything. You know they also tell you that not to feed babies solids until they are certain age, but we give it to them anyway. We know that they’ll be OK.
Other mothers made similar statements, particularly in regard to decisions about feeding babies solids. One said, “Grandma said she is hungry, she needs more than just milk, so I started to give her food in addition to breast milk.” Others stated, “My family wanted my child to be eating solid at a young age [1–2 mo]” and “My family told me to put cereal in her bottle.”
Theme 2: “I Want My Child(ren) to Be Healthy”
The mothers unanimously expressed a strong desire to feed their children healthy food. When asked to describe what foods she considered healthy, 1 participant stated, “Vegetables, fruits, meats, of course, and lots of milk.” When asked, some participants elaborated on the importance of milk—for example, “Because they need it [milk] for their bones; they are growing, you know. They need strong bones.”
The mothers seemed to place more emphasis on healthy children than on healthy food. All mothers expressed a clear desire for their children to be robust. One mother stressed the point, saying, “You don’t want them to be these fragile little things!” The mothers believed that a healthy child is “chubby, but not fat.” One mother elaborated, stating, “According to the doctor, he is like 5 pounds overweight or something, but I don’t know if he’s just a big kid, because he doesn’t really look overweight to me. He’s always been heavy.” These beliefs were reinforced by grandmothers and older relatives. The mothers reported hearing comments from their grandmothers or older relatives such as “You are not feeding her enough . . . she looks weak to me,” “They are skinny,” and “Oh my god, look, she is losing her cheeks.”
The expressed cultural perception that skinny is not healthy could explain the mothers’ reported leniency in feeding habits. Most mothers allowed their children to eat snacks as often as they liked. Some mothers explained that children in general are always hungry and should have the freedom to decide when they are full: “When she is hungry, she goes to the refrigerator and takes whatever she wants.” “Throughout the day, they have some snacks. I let them have chips, yogurt. They will have fruit, and they will eat their little junk, too.” “Chips, goldfish, crackers, just stuff.” “Snacks all the time.”
Theme 3: “Always Soup and Always Rice”
The mothers reported specific food choices and preparation techniques that were affected by cultural influences. When the mothers were asked what they fed their children, soup and rice were the two most common answers. One stated, “It’s always soup and always rice.” Soup and rice were given to children at very young ages. One mother shared, “They [family members] were giving him soup at 3 months old.” Another stated, “I started supplementary food around 2, 2½ months. I added it in the bottle.” When asked to describe what supplementary food she gave her child, the mother responded, “soup, rice, mashed potatoes.” The preference for feeding soup and rice to young children relates to the general cultural preferences for those foods. As one mother said, “We pretty much eat white rice or rice with everything.” Others talked about the cultural belief that soup is healthy: “When we are sick, we drink soup” and “Soup is like brain food; like if you eat enough soup, you won’t ever get sick.”
Participants shared their preferences for homemade meals: “I prefer cooking at home; I do not believe in prepackaged food or microwavable [food].” “A home-cooked meal is showing love to your family, to your child.” “I wanna keep it that way, it’s better; homemade food is the best.” “I homemade cook about 6 days out of a week. Usually I make rice, beans, chicken; some days soup.” They also described ethnic influences on food preparation: “The way I prepare the food, that’s from Grandma—Brazilian way of cooking.” “I learned a lot of my cooking from my mom and my sister and my mother-in-law.” “Peruvians love hot sauce.” “We always seasoned our food.” “[We put] garlic in everything.” “We use sofrito” (i.e., sauce used as a base in Latin American cooking). “He is supposed to eat more beans, red beans, lentil beans, white beans . . . they are good for protein.”
Theme 4: “Mealtime Is Family Time”
The mothers placed a high value on family mealtime. They considered togetherness during mealtime as a symbol of a unified family, an important tradition in Latino-American culture. The mothers reminisced about their past family mealtime experiences and felt those experiences contributed to fond childhood memories. All mothers expressed a strong desire to replicate similar experiences for their own children: “When you sit down with your father, your mother, you feel good . . . because you see the family’s union.” “The most important thing for me when I stay at the table with my family and see my kids eating something, you know, I see my family.” “I like we all sit at the table together at dinner.”
Changes to Latino Cultural Feeding Practices
In addition to the four identified themes, we also observed that despite these mothers’ positive feelings about cultural influences on their feeding practices, some made attempts to change common practices. When they became aware that culturally influenced choices or practices were unhealthy, they tried to change them to promote better outcomes for their children. These changes were reflected in disagreements these mothers described regarding feeding: “We’re Americanized, you know, so we were like, ‘no, no, we’re not doing that.’” “She [Grandma] drives me insane about feeding. We’ll have a big argument all the time.” “She [Grandma]’ll be like, ‘She didn’t eat anything,’ and [I’ll say,] ‘But she has a little stomach; she doesn’t need a ginormous plate that we eat.’”
Word Cloud Visualization Analysis
As depicted in Figures 1 and 2, “starch” was the food category most frequently mentioned in the interviews. Starch-related terms, such as rice, potato, and cereal, appeared to be the most common foods these mothers chose to feed their children. Vegetables, milk, fruit, chicken, and soup were also used frequently.
Discussion
Interviews were conducted with 12 Latino-American mothers residing in the greater New York metropolitan area. Despite their heterogeneous ethnic backgrounds, these mothers provided responses that revealed common themes regarding feeding practices. The findings of this study can help increase a general understanding of the ways culture might play a role in mothers’ decisions about how, when, and what to feed their children.
In this study, we learned about the influences that relatives and others have on maternal feeding practices. These influences were highlighted by the first theme, “Grandma knows best”; the mothers addressed the importance of their own mothers, mothers-in-law, and grandmothers in their feeding decisions. This finding confirms Bryant’s (1982) conclusion that social networks strongly influence infant feeding practices of Cuban, Puerto Rican, and Anglo families in Florida. The mothers in our sample, like those in Bryant’s study, listened to members of their social network to determine when to start feeding their children solid food.
Paternal and maternal grandparents have been found to play an essential role in determining feeding practices (Lindsay et al., 2011; Losch et al., 1995), and this influence is not unique to Latino-American culture (Abel et al., 2001; Bezner Kerr et al., 2008). Bezner Kerr and colleagues (2008) reported that grandmothers in Malawi held powerful positions in extended families and communities in general. They often imposed their child care opinions on younger mothers, and their ideas about early child feeding often differed from conventional Western medicine. Abel et al. (2001) reported similar observations in a cross-cultural study of infant care practices in New Zealand.
Mothers of different racial and ethnic backgrounds engage in diverse feeding practices (Hughes et al., 2005; Papaioannou et al., 2013). Maternal perceptions of a child’s weight and health status can be socially and culturally influenced. In our study, the mothers reported that they preferred “chubby” babies and wanted their children to be strong and robust. These findings are in line with reports from other researchers that Latino-American mothers perceive heavier children as healthier (Crawford et al., 2004; Lindsay et al., 2011; Reifsnider et al., 2006).
Several studies have examined health beliefs surrounding weight (Crawford et al., 2004). Crawford and colleagues (2004) explored beliefs and attitudes toward early childhood weight issues in Latino-American mothers. They presented 43 Latino-American mothers with a set of photographs of children aged 3–4 yr of various shapes and sizes ranging from underweight to overweight. Mothers in the study consistently reported that “a heavier child looked healthiest because her hair was ‘healthy and shining,’ her skin was ‘full of life,’ and she had a ‘very happy expression’” (Crawford et al., 2004, p. 390). Lindsay et al. (2011) reported that within Latino-American culture, a child’s weight reflects parenting skills; having a “skinny” child is a sign of bad parenting and poor health.
In our study, the mothers focused on giving their children healthy food, as described in the “I want my child(ren) to be healthy” theme. The mothers seemed to think they were making healthy feeding decisions, but their strategies were not always consistent with the beliefs of health care providers—for example, some mothers reported allowing their children to snack whenever they wanted. Similar parental feeding practices have been observed in other studies (Evans et al., 2011; Sherry et al., 2004).
The theme “always soup and always rice” includes the mothers’ descriptions of their children’s diets. Latino-American young children are frequently fed rice, potatoes, soup, and beans. Whereas Mennella et al. (2006) reported in their study of feeding practices in Mexico that fruit was the predominant choice of first food for infants, in our study rice cereal in children’s bottles was the most common first supplementary food. The mothers in our study also stressed the importance of milk. Brotanek and colleagues (2009) reported a similar observation; they described the belief of Mexican-American parents that toddlers should be given as much milk as they want because milk is a good nutritional supplement in case they do not eat enough of the right foods. Brotanek et al. further proposed that this belief might contribute to the high prevalence of bottle-feeding past age 15 mo among Mexican-American parents, a practice associated with excessive milk intake and iron deficiency in toddlers.
In the literature, four parental feeding styles have been classified using dimensions of responsiveness and demandingness: authoritative, authoritarian, indulgent–permissive, and uninvolved–neglectful permissive (Blissett, 2011; Papaioannou et al., 2013). Chaidez et al. (2011) reported that the indulgent–permissive feeding style was dominant among the Mexican-American mothers they studied. That is, in determining what to feed their children, these mothers tended to cater to the child’s preferences. Moreover, in deciding when to feed their children or how much they should eat, most of the mothers based responses on their interpretations of their children’s cues. The mothers in our study reported similar behavior, especially in regard to snacks.
As captured in the theme “mealtime is family time,” all mothers in the study recognized and appreciated the value of family mealtime. This finding reflects the traditional Latino-American emphasis on the family as the single most important social unit. Latino-Americans consider midday and evening meals important family and social events (Clutter & Zubieta, 2009).
Limitations
This study has several limitations. The Latino-American mothers recruited for this study were exclusively from the greater New York metropolitan area and may not share beliefs with other Latino-American groups around the country. In addition, the qualitative approach necessarily limits generalizability. Despite intensive training, it may have been impossible to mask all bias that the researchers and graduate student interviewers might have had. The snowball sampling recruitment method and the fact that interviews were conducted only in English limited the pool of potential participants and may have affected the scope of described phenomena. Moreover, our sample size was small, and only mothers were included; the views of other family members were not represented. Conducting bilingual interviews and including major social network members (e.g., grandmothers) in a larger sample will be considered in future studies. We also acknowledge that Latino-Americans are a heterogeneous ethnic group, and feeding practices may vary widely depending on country of origin. We intend to further explore feeding practices, taking into consideration factors such as country of origin and food acculturation.
Implications for Occupational Therapy Practice
The findings of this study have the following implications for occupational therapy practitioners who provide early feeding interventions:
Practitioners need to recognize cultural influences on feeding practices to interpret feeding evaluations in context. For example, when a mother reports she has introduced supplemental food to her young child, the practitioner should clarify how the supplemental food was given (e.g., spoon vs. bottle) and not assume the child has certain oral–motor skills.
It is essential to avoid using stereotypical or misinterpreted information when designing and implementing targeted feeding intervention strategies. Understanding cultural influences on feeding practices promotes family-centered, meaningful interventions that are sensitive to maternal needs.
Practitioners can use our findings as a resource when choosing or introducing food during feeding interventions. The inclusion of culturally relevant foods promotes implementation of interventions by mothers and family members.
Child feeding, and the people involved in decision making about child feeding, cannot be addressed in isolation. When working with Latino-American families, practitioners must consider the multifaceted role grandmothers play in child feeding and household social relations. Grandmothers are influential members of immediate social support networks. Practitioners should consider their perspectives when recommending feeding practices and planning interventions. Moreover, practitioners must remain alert to the inherent conflicts within extended families and potential distrust of medical institutions (Bezner Kerr et al., 2008).
Conclusion
Understanding the range of perceptions and influences Latino-American mothers identify as affecting feeding practices is vitally helpful to health care providers. Consideration of cultural beliefs and practices surrounding infant feeding and well-being is important to successfully deliver health services to a diverse population. Understanding cultural influences on feeding practices promotes family-centered, meaningful interventions that are sensitive to maternal needs. Recognition of cultural influences contextualizes information for health care providers and can be used to design and implement effective targeted feeding intervention strategies that avoid stereotyping or misinterpreted information.
Footnotes
Acknowledgments
The authors thank participating families and New York University graduate students in the Department of Occupational Therapy for making this project possible. This study is exempt from clinical trial registration.
Jim Hinojosa passed away while this article was in press. He is greatly missed.