
Abstract
To address population aging (World Health Organization, 2014), health professionals, including occupational therapy practitioners, need to provide effective interventions. Lifestyle Redesign® (Clark et al., 2012) empowers older adults to regularly perform healthy and fulfilling activities. This preventive occupational therapy intervention involves weekly 2-hr group sessions and monthly 1-hr individual meetings over 6–9 mo.
Lifestyle Redesign has been shown to improve health and to be cost effective (Lévesque et al., 2019). Two randomized controlled trials (RCTs), one with 361 and the other with 460 older Americans, showed positive effects on bodily pain, vitality, social and mental functioning, and life satisfaction (Clark et al., 1997, 2001, 2012), and 90% of participants maintained the improvements after 6 mo (Clark et al., 2001). Health care costs were lower for participants (US$967) than for control groups that did not receive the intervention (US$3,334) or that participated in social activities (US$1,726), but this difference was not statistically significant (Hay et al., 2002).
Quantitative studies on adapted versions of Lifestyle Redesign have reported mixed results. A RCT conducted by the original team showed that a translated and adapted Mandarin version and the original intervention maintained health in older Chinese (n = 12) and English-speaking (n = 29) adults living in Los Angeles (Jackson et al., 2000). A control group of older Chinese adults participating in social activities (n = 35) experienced a decline, but the difference between the groups was not significant. Another study of a 4-mo version involving frail older adults found positive trends in role functioning, pain, and general health in the experimental group (n = 12) similar to those in the control group (n = 12; Horowitz & Chang, 2004). In a third study, 28 older adults who participated in the Lifestyle Matters Program in the North of England showed trends toward improvement in health (Mountain et al., 2008), but the winter may have influenced the results. Another RCT with older adults who had a stroke found a trend toward greater improvements in mental health, bodily pain, physical functioning, and emotional role but no significant difference between the experimental (n = 39) and control (n = 47) groups (Lund et al., 2012).
Two studies on adaptations of Lifestyle Redesign considered social participation. One preexperimental study of the Life of Wellness program found an increase in monthly social or community activities (from 56 to 66%) for middle- and upper-class older adults living in senior apartments (n = 39; Matuska et al., 2003). In a quasi-experimental study of a 4-mo Swedish version, the intervention group showed significant improvements in vitality (p = .01) and mental health (p = .03) but not in other domains (ps = .16–.83) or participation (p = .07; Johansson & Björklund, 2016). No difference was observed between the intervention (n = 22) and control (n = 18) groups, which were not fully matched. Despite a lack of power, these studies showed positive trends in health and social participation in older adults receiving an adaptation of Lifestyle Redesign. To improve the crafting of preventive occupational therapy interventions, further research is needed on adapted programs.
Because Lifestyle Redesign was considered relevant for practice in Quebec (Lévesque et al., 2019), a French-Canadian version was developed. This version was translated by a professional French-Canadian translator and validated by 14 experts. The concepts and themes mostly applied to the French-Canadian culture and context, but adaptations were also required to reflect the health care system and demographics of the population. The publication of the manual is in process. The influence of the French-Canadian version on the health and social participation of older adults, including those with significant communication and mobility disabilities, needed to be explored.
Moreover, to our knowledge, no study has considered the influence of Lifestyle Redesign or its adapted versions on older adults’ leisure and life-space mobility, two outcomes especially important for older adults. Defined as the extent of spatial latitude experienced by a person (May et al., 1985), life-space mobility has been associated with obesity (Bouchard et al., 2007), physical disability (Guralnik et al., 2000), quality of life (Beswick et al., 2008), mortality (Clausen et al., 2007), and health care costs (Liu-Ambrose et al., 2010). Before the French-Canadian Lifestyle Redesign can be widely implemented, it is essential to know more about its effects on older adults. In addition, an in-depth understanding of the experience of French-Canadian older adults with and without disabilities, those primarily concerned with the intervention, is of particular importance for occupational therapy practitioners, who consider clients’ perceptions when working on improving or maintaining their functioning. To address this gap in the literature, this first pilot study aimed to explore the influence of the French-Canadian Lifestyle Redesign on older adults’ health, social participation, leisure, and mobility.
Method
Study Design and Participants
This pilot study used a mixed-methods concurrent triangulation design (Creswell & Plano Clark, 2017) including a preexperimental component with pretest (T1), posttest (T2), and 3-mo (T3) and 6-mo (T4) follow-ups and an exploratory descriptive qualitative clinical study (Miller & Crabtree, 2003). The sample included 16 community-dwelling older adults with and without disability. A sample size of 16 participants allowed detection of a standardized difference of .75 or greater between two means according to paired bilateral t tests based on a significance level of .05 and power of .80 (Machin et al., 2009). This difference was considered sufficient in studies that explored the influence of another intervention on leisure (Levasseur et al., 2016) and life-space mobility (Pigeon et al., in press). This sample size also allowed in-depth exploration and data saturation.
Eligibility criteria were (1) age 65 yr and older, (2) no or mild (group without disability) or moderate or severe (group with disabilities) loss of autonomy, (3) normal cognitive functions, (4) residence in a conventional or residential home for semi-independent older adults, and (5) French speaking. Participants were recruited from a previous study of people attending a day hospital and day center in a Health and Social Services Centre (HSSC) in Quebec (Canada) and from people living in a senior residence. The research ethics committee of the Eastern Townships HSSC approved the study (2015–488).
Data Collection Procedures
Participants were recruited until the predetermined sample size (n = 16 + 3, anticipating possible attrition) was reached. All participants signed an informed consent form and were met individually at home by a research assistant or occupational therapy student specially trained to administer the questionnaires. An experienced research assistant (Maryke Beaudry) conducted the qualitative interviews. At T1, one sociodemographic and eight outcome questionnaires, four of which are reported here and the others elsewhere (Trépanier et al., 2019), were administered in approximately 120 min. At the end of the 6-mo intervention period (T2), participants answered the same outcome questionnaires and, about 1 mo later, had a face-to-face semidirected individual interview lasting about 90 min. All interviews were digitally audiotaped, transcribed, and verified with respect to the wording used by participants. After the first few interviews, two authors (Maryke Beaudry and Mélanie Levasseur) discussed and adjusted the questions for subsequent interviews. Finally, 3 mo (T3) and 6 mo (T4) after the end of the intervention, participants answered the same questionnaires again.
Intervention
The French-Canadian Lifestyle Redesign intervention was led by an occupational therapist who took the University of Southern California 6-hr online introductory training course. This therapist was supervised on a weekly basis by an academic occupational therapist (Mélanie Levasseur) specializing in health promotion and clinical research who was familiar with the intervention (and very involved in the translation). Through this supervision, the intervening occupational therapist received regular feedback on her role and the intervention. Weekly 2-hr group sessions were held over a 6-mo period between August 2015 and March 2016. These sessions were based on 12 modules (e.g., occupation, health, and aging; transportation and occupation) from the second edition of the Lifestyle Redesign manual (Clark et al., 2015) and involved didactic presentations, peer exchanges, reflective exercises, direct experience, and personal exploration (Carlson et al., 1998). Every month, one group outing and individual meetings with the occupational therapist were planned. The meetings aimed to help participants integrate the group session content and engage in personalized meaningful activities. In the group sessions for participants with moderate or severe loss of autonomy, the occupational therapist was assisted by one or two volunteers.
Outcome Variables and Measures
Data on health, social participation, leisure, and life-space mobility were collected with four questionnaires. The 36-item Short Form Health Survey (SF–36) consists of 36 items covering eight domains related to physical and mental health: physical functioning, role physical, bodily pain, general health, vitality, social functioning, role emotional, and mental health (Ware et al., 2000). Higher scores indicate greater frequency of social participation. Widely used in research, including previous Lifestyle Redesign studies, the SF–36 has good psychometric properties, including good internal consistency (Cronbach’s αs of .83–.93 for the eight domains, .94 for the physical component summary, and .89 for the mental component summary; Gandek et al., 2004) and good test–retest reliability, even for testing after 6 mo (correlation coefficients of .60–.90 except for bodily pain, .43; Ware, 2000). The SF–36 is also sensitive to change (Gatchel et al., 1999), with a difference of 5 points in scale scores being clinically significant (Ware et al., 1993).
The Social Participation Scale measures the frequency of participation in 10 community activities and has good internal consistency (Cronbach’s αs of .85–.91; Richard et al., 2009). Higher scores indicate greater frequency of social participation; a difference of 1 point on each activity score is considered clinically significant. The Leisure Profile assesses involvement in leisure activities, attitudes toward leisure, and difficulties that might influence leisure activities; higher scores reflect greater leisure participation. It has acceptable interrater (κ = .21–.80) and test–retest (.41–.60) reliability (Dutil et al., 2007). The Life-Space Assessment (LSA) measures life-space mobility, specifically the range, independence, and frequency of movement over the preceding 4 wk; higher scores indicate better mobility (Baker et al., 2003). The LSA has shown excellent test–retest reliability (intraclass correlation coefficient = .87) and moderate to substantial concordance for 18 of 20 items (κ = .47–.73; Auger et al., 2009). It has good construct validity with observed physical performance and self-reported function (95% confidence interval [.82, .97]) and good sensitivity to change (Baker et al., 2003). Finally, a semistructured interview guide (see Supplemental Appendix A, available at the end of this document) validated by five qualitative research experts and pretested was used to explore the self-perceived effect of the adapted Lifestyle Redesign on participants.
Data Analysis
To foster transferability (Laperrière, 1997), the participants’ sociodemographic characteristics and outcomes were analyzed using descriptive statistics. Scores were compared with the Friedman test followed by the Wilcoxon signed-rank test for all participants and, in an exploratory manner, each group separately. Because of the exploratory nature of this study and the influence of seasonal variations on Quebecers’ health, social participation, leisure, and mobility, changes at any of the postintervention measurement times with p < .05 were considered to be potentially attributable to the intervention.
Interview transcripts underwent thematic content analysis using mix extraction grids (Miles et al., 2014). The data analysis involved (1) verbal data collection, (2) reading of data, (3) division of data into units of sense, (4) organization and reformulation of original data in disciplinary terminology, and (5) synthesis of results. Themes that emerged from the interview content were organized and renamed according to the Human Development Model–Disability Creation Process (HDM–DCP; Figure 1), a model of human development and disability (Fougeyrollas, 2010). The HDM–DCP illustrates interactions among intrinsic personal factors, extrinsic environmental factors, and participation (operationalized as life habits). To increase credibility, reliability, and confirmability (Laperrière, 1997), the first author (Mélanie Levasseur) co-coded one-third of the data, which had first been exhaustively analyzed by a specially trained research assistant (Maryke Beaudry). Levasseur closely supervised the analysis, making adjustments until consensus was reached regarding the participants’ perceptions of the intervention. Additional memos describing the thoughts, questions, and discussions of the research team were used. Analyses were conducted using IBM SPSS Statistics (Version 18; IBM Corp., Armonk, NY) or NVivo (Version 10; QSR International, Melbourne, Victoria, Australia).
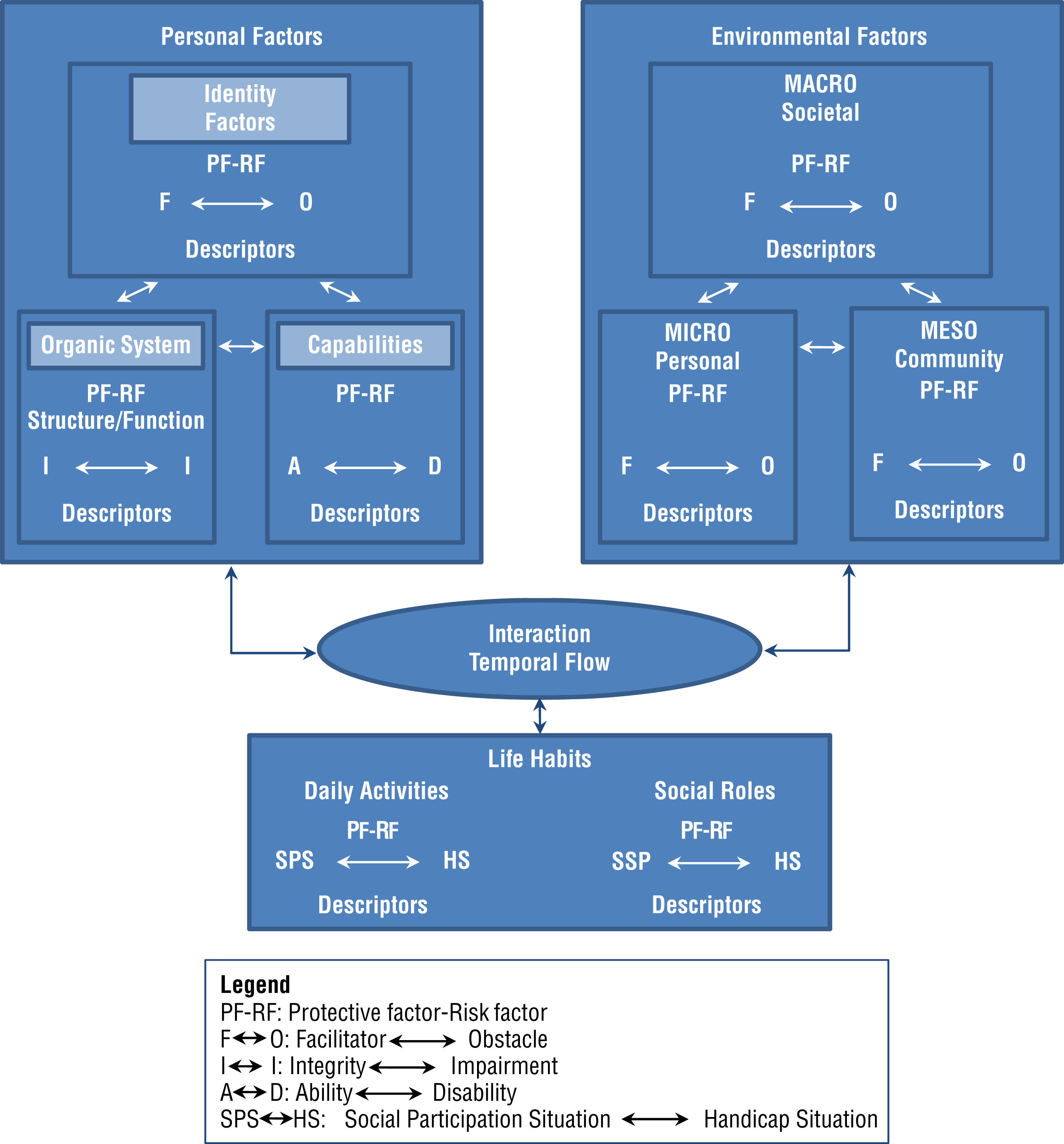
Human Development Model and Disability Creation Process (HDM–DCP) illustrating interactions among intrinsic personal factors, extrinsic environmental factors, and life habits.
Results
For parsimony with respect to the quantitative results, themes presented in this article focus on health, social participation, leisure, and mobility. Although most themes were supported by many participants, because of limited space only one quotation per theme is given as an example. In this section, the participants, operationalization of the intervention, and general impressions of Lifestyle Redesign are described. Then for each variable, the quantitative results for all participants, followed by each group separately, and finally a summary of the qualitative results are presented.
Participants and Intervention
Of the 19 participants assessed at T1, 1 had serious health problems preventing participation in the intervention and 1 died, leaving 17 older adults who completed the program and were interviewed (Table 1). Because 1 participant (Participant [P] 17) had vision and hearing problems that impeded questionnaire completion, only 16 were reassessed. At baseline, the 3 nonparticipants were not different from those who participated except for older age (p < .01), greater loss of autonomy (p = .01), and smaller life-space mobility (p = .047).
Participant Characteristics (N = 17)
Functional Autonomy Measurement System (maximum score = 87; Hébert et al., 1988): <5 = no disability; 5–19 = slight to moderate disability; >19 = moderate to severe disability.
Income categories (in Canadian dollars): 1, ≤$10,000; 2, $10,001–15,000; 3, $15,001–20,000; 4, $20,001–25,000; 5, $25,001–40,000; 6, >$40,000; R, refused to answer or didn’t know.
International Classification of Diseases (10th rev., World Health Organization, 2004) categories: 1, diseases of the eye and adnexa; 2, diseases of the musculoskeletal system and connective tissue; 3, diseases of the circulatory system; 4, endocrine, nutritional, and metabolic diseases; 5, diseases of the nervous system; 6, other.
This participant did not complete the questionnaires.
Participants were aged 65–90 yr (mean [M] ± standard deviation [SD] = 76.4 ± 7.6; median [Mdn] ± semi-interquartile interval [Q] = 74.0 ± 5.8). All were Caucasian, the majority were women (n = 10; 62.5%) and owners (n = 5; 31.3%) or tenants (n = 7; 43.8%) of their dwelling, and nearly half lived alone (n = 7; 43.8%). Half had 12 or more years of schooling (n = 8; 50.0%), and most had family income under CAN$40,000 (n = 12; 75.0%) and rated their health as good or excellent (n = 12; 75.0%; Table 1). Two groups as homogeneous as possible were created, one with 7 participants with disabilities and one with 10 participants without disability.
Five participants with disabilities lived in the same residence where the group meetings were held. The older adults participated in an average of about 25 group meetings with the occupational therapist (M ± SD = 24.3 ± 2.2; Mdn ± Q = 25.0 ± 1.5), which amounted to 90% or more of the sessions and went on an average of four or five outings (e.g., restaurant, market, museum). Reasons for missing group meetings were most often being ill, working, or having an appointment. The participants attended 5–11 individual meetings with the occupational therapist (M ± SD = 6.1 ± 0.6; Mdn ± Q = 6.0 ± 0.0).
Participants reported mostly positive effects from the program, sometimes no effect, but rarely negative effects on their personal and environmental factors and social participation (Figure 2). The program fostered participants’ knowledge about health, social participation, leisure, and mobility. This knowledge stimulated them and, depending on their personal factors and with a safer and mobilized environment, encouraged their efforts to take action. With regard to personal factors, participants reported that the French-Canadian Lifestyle Redesign program modified their vision of themselves and others and empowered them. This vision and empowerment bilaterally influenced their willingness to act, which in turn similarly modified their health and relationship skills. In terms of interaction between personal and environmental factors, by facing challenges and taking action, the participants reported that they improved their social participation, leisure, and mobility. Social participation improvement included increases in health habits, activities in the community or with others, social interactions both within and outside the Lifestyle Redesign program, and, during interactions with others, mobility.
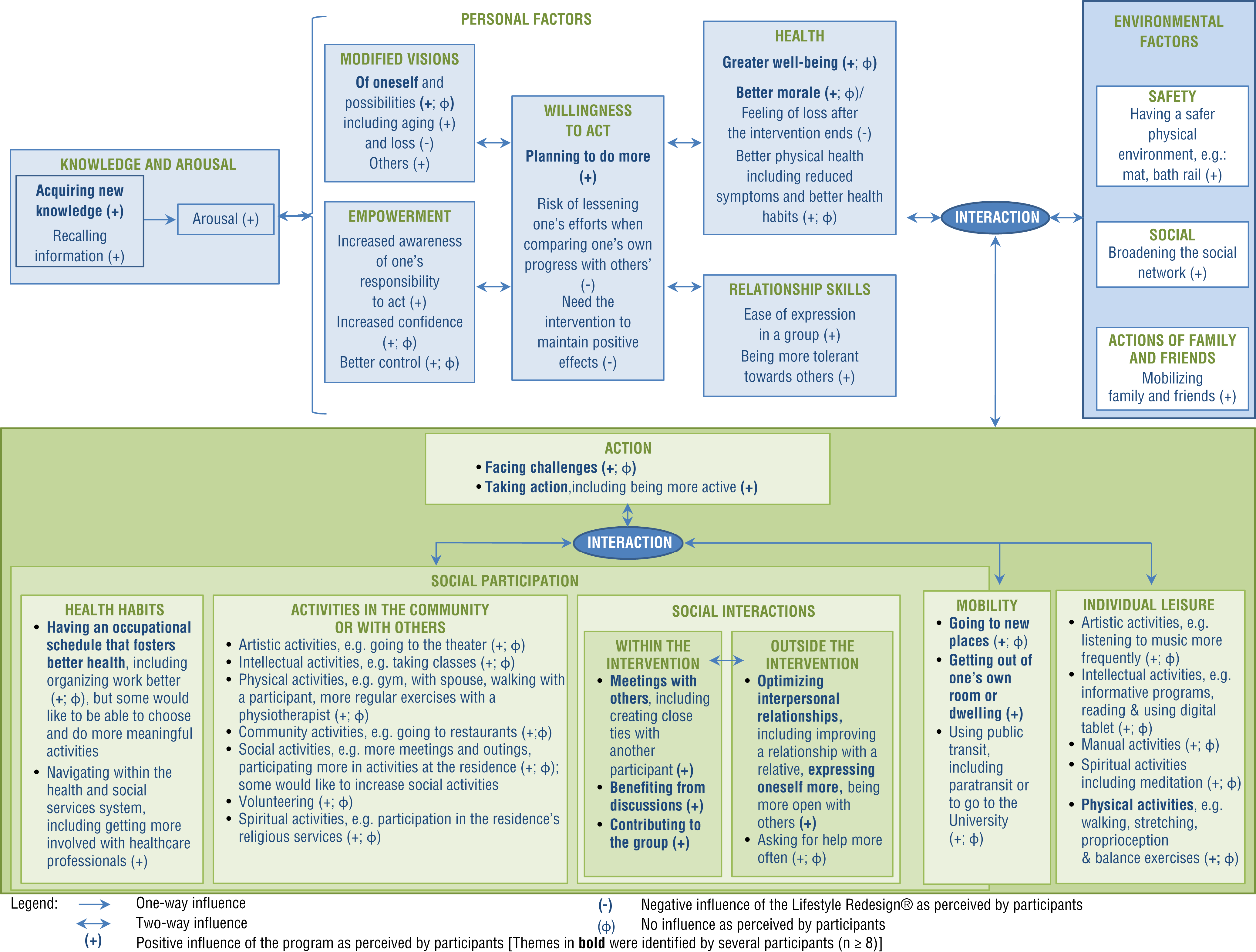
Participant-reported influence of the French-Canadian Lifestyle Redesign® program.
Health
Pre- and postintervention comparisons showed that for both groups as a whole, participants’ health did not change, but the mental component improved between T3 and T4 (Table 2). Surprisingly, physical role decreased between T2 and T3, indicating that participants’ physical health further affected time spent, accomplishment, and difficulties in daily activities. Although not statistically significant, emotional role, absence of pain, social functioning, and mental health scores showed a tendency to increase. According to group results for participants with disabilities, a decrease was observed in the physical component (T2, Mdn ± Q = 29.1 ± 3.0 vs. T3, 25.7 ± 4.0, p = .046), physical functioning (T2, 7.5 ± 8.1, vs. T3, 2.5 ± 6.3, p = .03, and T4, 0.0 ± 3.8, p = .04), and physical role (T2, 75.0 ± 19.5, vs. T3, 31.3 ± 26.6, p = .04) but an improvement in pain (T3, 46.0 ± 12.4, vs. T4, 56.0 ± 13.8, p = .03). In participants without disability, the mental component increased (T3, 54.5 ± 5.0, vs. T4, 57.8 ± 4.3, p = .04), as did general health (T1, 84.5 ± 10.9, vs. T4, 87.0 ± 15.4, p = .048).
Comparisons of Scores on Main Variables Before and After the Intervention (N = 16)
Note. max. = maximum score; Mdn = median; Q = semi-interquartile range; SF–36 = 36-item Short Form Health Survey; T1 = pretest; T2 = posttest; T3 = 3-mo follow-up; T4 = 6-mo follow-up.
Friedman test.
T2 differs significantly from T3 (all differences associated with Wilcoxon signed-rank test).
T3 differs significantly from T4.
T1 differs significantly from T2.
T2 differs significantly from T4.
T4 differs significantly from T1 and T2.
T1 differs significantly from T3 and T4.
The majority of participants reported improved mental health (Figure 2): “I feel better, less depressed” (P12) and “[The program] makes me want to enjoy life again” (P10). Reduction in symptoms (e.g., stiffness) was also reported; one man with disabilities explained that during the group, “My legs hurt, but it was OK. . . . If something interested me and I liked it enough, I didn’t feel the pain” (P11). Participants without disability attributed positive health effects mainly to better health habits, such as increased physical activity.
Social Participation
Social participation did not change significantly after the intervention for participants (Table 2) but increased for those with disabilities (T1, Mdn ± Q = 2.5 ± 7.5, vs. T2, 7.0 ± 11.9, p = .03). Although not significant, a tendency toward improvement was also observed in participants without disability (T1, 21.0 ± 9.0, vs. T2, 26.0 ± 7.4; T3, 27 ± 7.4; and T4, 28.5 ± 6.5; ps = .14–.51).
Several participants reported increased activities in the community or with others (Figure 2); as 1 participant explained, “We take more time. . . . We go to the restaurant, visit people, act like good neighbors” (P10). Others resumed previous activities or started new ones. After an individual session, 1 participant reported, “It induced me to find volunteer work that I like” (P9). Although the program encouraged participants to act—“I do more things now because I order myself to do something; before the program, I just sat here, in my armchair, waiting for time to go by” (P12)—being more active did not always transform into changes in activities. Some participants faced participation challenges, and others struggled with perseverance in experimenting or searching for meaningful activities. Nevertheless, meeting people, benefiting from exchanges with others, and contributing to the group were among the important contributions of the program: “I get a lot out of being with others and being able to chat” (P4). It also helped optimize interpersonal relationships: “[The program] made me want to be more open, to socialize” (P13).
Leisure
Pre- and postintervention comparisons showed that participants’ leisure did not change except for an increase in interest between T1 and T2 (Table 2). Frequency of activities decreased between T2 and both T3 and T4, as did the desire to modify leisure practices between T2 and T4. Impairments increased between T1 and T2 but decreased between T2 and T4 (Table 2). Finally, there were fewer physical environment obstacles at both T1 and T2 than at T4, but social environment obstacles decreased between T1 and both T3 and T4. Results for participants without disability revealed an increase in interest in leisure activities (T1, Mdn ± Q = 23.0 ± 1.8, vs. T2, 25.0 ± 1.4, p = .02) but a decrease in frequency (T2, 21.5 ± 2.1, vs. T3, 19.0 ± 1.3, p = .03). The desire to modify leisure practice also decreased for this group (T1, 17.1 ± 1.3, vs. T4, 15.0 ± 1.1, p = .01; T2, 17.5 ± 1.7, vs. T3, 15.5 ± 1.4, p = .049, and T4, 15.5 ± 1.4, p = .01). Impairments in participants without disability also changed over time (T2, 6.0 ± 3.0, vs. T1, 3.0 ± 2.6, p = .02; T3, 2.5 ± 2.1, p = .02; and T4, 2.0 ± 2.4, p =.03). In participants with disabilities, positive attitudes toward leisure increased after the intervention (T1, 12.5 ± 1.4 vs. T3, 15.5 ± 1.5, p = .04).
Although some participants reported no change in leisure, others planned to do more or actually increased the frequency of activities—for example, physical exercise such as walking regularly (Figure 2): “I started doing it again. I walk for an hour or hour and a half every morning and sometimes in the afternoon” (P5). Although not all participants maintained the activities, they resumed or modified previous leisure activities or tried new ones, including more intellectual stimulation or physical exercise: “[The occupational therapist] showed us proprioception, so I do balance exercises” (P3). Participants also reported trying meditation: “I started exploring it. It feels good, relaxing” (P6).
Mobility
Life-space mobility decreased between T1 and T2, during wintertime, and increased again between T2 and T4 (Table 2). Maximum space mobility with any type of assistance did not change after the intervention except for a decrease in mobility without human assistance between T1 and T2 and a decrease in mobility without any assistance between T2 and T4. A decrease followed by an increase in life-space mobility was also observed in participants without disability (T2, Mdn ± Q = 73.0 ± 8.3, vs. T1, 83.0 ± 7.3, p = .01, and T4, 82.0 ± 6.3, p =.02).
Participants reported that the program resulted in increased mobility (Figure 2): “[The program] got me out of my room” (P17). Several participants visited new places: “There are places where I’ve never been and where I would never have gone, either. . . . I hadn’t been out to eat since my stroke. . . . I went back to the pub twice after [the program] with my children” (P11). Nevertheless, for several participants, travel did not differ after the program, especially if they drove their own car, which allowed them to have good mobility before the program.
Discussion
This pilot study explored the influence of the Lifestyle Redesign program on French-Canadian older adults’ health, social participation, leisure, and mobility. This version of the program seemed to have a beneficial effect on participants’ mental health and interest in leisure and, in those with disabilities, on social participation and attitudes toward leisure. Participants reported positive effects on their health, social participation, leisure, and mobility and on the frequency and quality of their contacts. Discrepancies with previous research might be explained by outcomes that were differently measured and defined by participants or by difficulties in accurately perceiving change (Rocke & Lachman, 2008).
Contrary to the original version (Clark et al., 1997, 2001, 2012) and other adaptations of Lifestyle Redesign (Horowitz & Chang, 2004; Jackson et al., 2000; Johansson & Björklund, 2016; Lund et al., 2012; Matuska et al., 2003; Mountain et al., 2008), the absence of further significant results in the current study might be attributable to the small sample size. Power based on social participation between T1 and T2 was 35.5% and between T1 and T4 was 10.5%. Moreover, although a shorter version of Lifestyle Redesign was found to be feasible with high-functioning participants (Cassidy et al., 2017), 6 mo is a minimal period for this type of intervention, which might partly explain the limited changes in this sample. The present sample was Caucasian and educated, and the majority of participants had high incomes and good health and had been exposed to public health messages concerning the importance of life habits, all factors that might also have contributed to the limited changes. In another qualitative study, however, only a few participants reported that Lifestyle Redesign had not affected them appreciably (Blanchard, 2010).
Although French-Canadian older adults face challenges similar to those of other older adult populations in terms of disability prevention and life expectancy (Organisation for Economic Co-operation and Development, 2018), the experience of French-Canadian older adults might also reflect differences in culture, health habits, and the environment. For example, in working class neighborhoods, the fundamental values are the great importance given to daily life and immediate pleasures, destiny, and resourcefulness; the utilitarian merit assigned to education and scientific knowledge; the focus on concrete knowledge as well as interpersonal and affective relationships; and the importance attached to one’s group and neighborhood, coupled with a mistrust of people from other social backgrounds (Lacourse, 2011). For the less affluent, the body and health are tools whose use is maximized by accepting that they will deteriorate, whereas the wealthy want to preserve them for as long as possible and, consistent with Lifestyle Redesign, practice moderation. Lifestyle habits are perceived by the less affluent as a way to make life easier, and little emphasis is placed on prevention (Lacourse, 2011). A study of health lifestyle outcomes in Canada and the United States found that the inhabitants of eastern Canada were the most healthy and those of the southern United States the most unhealthy (Krueger et al., 2009).
In addition, the Canadian government has safety net policies promoting home care (Ministère de la Santé et des Services Sociaux [MSSS], 2003) and aging at home (Ministère de la Famille et des Aînés & MSSS, 2012), as legislated in the Act Respecting Health Services and Social Services and the Autonomy Insurance Act (MSSS, 2013). These policies are implemented partly through publicly funded HSSCs, which are responsible for providing frontline health care to people in each territory, including home care for older adults. Like the U.S. Medicare and Medicaid programs (Richmond & Fein, 2005), the Canadian health care system is mainly financed through tax revenues. HSSCs coordinate various services for older adults, taking into account their specific situation, needs, and physical and social environment. In partnership with community organizations and social economy enterprises, HSSC programs provide a wide range of services and activities, which might sometimes limit mutual aid between citizens who rely on government assistance.
Finally, winter weather conditions might also have affected the current results. Although summers in Quebec are comfortable and wet with daily high temperatures above 66 °F, winters are cold and snowy with daily high temperatures around 32 °F (Weather Spark, 2018), making travel more difficult.
Health
Contrary to the lack of changes in health found in the current study, previous studies on the original Lifestyle Redesign program showed that it prevented or slowed a decline in health compared with control groups (Clark et al., 1997, 2001, 2012). Moreover, secondary analyses of the second RCT (Clark et al., 2012) showed that higher activity frequency was associated with fewer depressive symptoms through enhanced social connections (Juang et al., 2018). Such mediating mechanisms and the qualitative results from the current study point to the complexity of the effects of this intervention on health. For example, the decreased physical role—that is, the impact of physical health on time, accomplishment, and difficulties in regular daily activities—might be attributable to the participants’ greater awareness of their impairments. Notably, physical role and vitality were especially influenced by Lifestyle Redesign in the first intervention study (Clark et al., 1997).
Social Participation
In line with two previous studies (Johansson & Björklund, 2016; Matuska et al., 2003), the current study found that an adapted version of Lifestyle Redesign tended to increase social participation. According to participants in the current study and in the second original RCT (Blanchard, 2010), the intervention fostered not only social activities and interactions but also personal and environmental factors that are prerequisites to social participation, such as relationship skills and a social network. These benefits were multifaceted and diverse, especially in social support and healthy activity. Other interventions have been shown to foster social participation in older adults (Raymond et al., 2013), including those with disabilities (Levasseur et al., 2016). Nevertheless, maintaining, experimenting with, and searching for activities often require personalized assistance (Piché et al., in press), such as that provided in Lifestyle Redesign.
Leisure
Further assistance might also be needed to modify and maintain leisure activities. Older adults are not always physically and emotionally able to participate in social and leisure activities (Levasseur et al., 2016). Adapting leisure activities to older adults’ capacities often requires the expertise of an occupational therapist and a recreation specialist. Other leisure studies found increased frequency of leisure activities (Chang et al., 2015; Kao & Chang, 2017), including in older adults with disabilities (Desrosiers et al., 2007; Levasseur et al., 2016). Interventions for leisure activities are currently not sufficiently targeted in Quebec community occupational therapy practice (Turcotte et al., 2015). Education focused on the meaning of activities for the client (Dattilo, 2016; Kleiber, 2001; Lee & Payne, 2016) and awareness of the benefits and importance of these activities (Dattilo, 2015, 2016; Kleiber, 2001; Mitchell et al., 2014; Mundy, 1998) appears to be effective in increasing leisure activities (Carbonneau et al., 2011; Kao & Chang, 2017).
Mobility
Because mobility is strongly influenced by the weather, changes in these participants’ mobility over time may be attributed to the winter and, for some, to living in a residence. The participants nevertheless reported an increase in mobility, which sometimes involved changes in the perceptions of members of their network, such as a family member or health assistant who had concerns about them traveling. Such concerns and help from Lifestyle Redesign to overcome challenges in public transportation have previously been observed (Blanchard, 2010). Similarly, one study on personalized assistance improved older adults’ travel habits and increased the number of places they visited as well as their ability to travel alone (Pigeon et al., in press), which is often restricted during aging (Yen et al., 2009).
Participants With Disabilities
The program’s influence differed according to participant characteristics, including medical conditions. In those with disabilities, the decreases in the physical component, functioning, and role and the increase in impairments may be attributed to the need to cope with serious health problems and disabilities that interfere with increasing activities. Such challenges were reported in studies of the original Lifestyle Redesign program (Blanchard, 2010), Lifestyle Redesign adaptations (Horowitz & Chang, 2004; Lund et al., 2012), and other interventions (Levasseur et al., 2016). It is important to adapt the program to the group’s specific needs (Clark et al., 2015), especially for older adults with disabilities and, as discussed by Blanchard (2010), in accordance with participants’ beliefs, values, and predispositions.
End of the Intervention
Because the follow-up was only 6 mo after the intervention, and because the measurements were likely influenced by the weather, it is difficult to judge the sustainability of the changes. Nonetheless, when interviewed 1 mo after the intervention, participants reported that they missed the group, negatively affecting their morale. Those with disabilities needed the assistance of the intervention to maintain some benefits, such as getting out. Consequently, it is important to prepare participants who need social interactions and assistance for the end of the intervention and to allocate the necessary resources to maintain the benefits, as was found for another intervention with older adults with disabilities (Levasseur et al., 2019). Future studies need to document facilitators of and challenges to both the intervention and the sustainability of changes.
Study Strengths and Limitations
Conducted by partners from different fields of expertise, this study is the first rigorous mixed-methods study of Lifestyle Redesign with French-Canadian older adults. The combination of deductive and inductive processes made it possible to provide nuanced explanations, in the participants’ own words, of how the intervention affected them that were not necessarily provided by questionnaire results. The plurality of data sources allowed triangulation of the data, fostering good internal validity (Laperrière, 1997). Social desirability was minimized by providing only a general explanation of the research objectives and by reassuring participants that there were no right or wrong answers. Study limitations include the small sample size and lack of a control group.
Implications for Occupational Therapy Practice
This study has the following implications for occupational therapy practice:
Lifestyle Redesign is a weekly 2-hr occupational therapy group intervention given over a 6-mo period that is designed to promote meaningful and healthy activities.
According to older French-Canadian participants, the translated and adapted Lifestyle Redesign program improved their knowledge about health, social participation, leisure, and mobility, which in turn improved their well-being.
Lifestyle Redesign helped this sample of older French-Canadians face challenges and participate more frequently in leisure and social activities, optimize their relationships, and go to new places.
Conclusion
Lifestyle Redesign is a promising occupational therapy intervention for older community-dwelling French-Canadians that seemed, as reported by participants, to have a beneficial effect on participants’ mental health and interest in leisure and, in those with disabilities, on social participation and attitudes toward leisure. This intervention has the potential to offer occupational therapists an innovative and rigorous intervention to promote meaningful and healthy activities among French-Canadian older adults. In line with strategies to address an aging global population, Lifestyle Redesign can lead to new opportunities for older adults to adopt healthy habits and enhance the social component of their lives. This intervention can also optimize how the needs of older adults are met, including the use of personal and environmental resources.
Further research is needed on innovative interventions fostering community integration and optimization of resources. In addition, more studies on the French-Canadian Lifestyle Redesign program are required using larger samples and experimental designs. It would also be interesting to explore facilitators and challenges to the intervention and its implementation.
Footnotes
Supplemental Appendix A. Semistructured Interview Guide
Acknowledgments
This study was funded by the Quebec Network for Research on Aging and the Canadian Institutes of Health Research (CIHR; Grant 126315) and registered at ![]() (NCT03398642). Free bus tokens were kindly provided by the Sherbrooke Transit Corporation. At the time of the study, Mélanie Levasseur was a Fonds de la Recherche du Québec-Santé Junior 1 Researcher (26815), and she is now CIHR New Investigator (360880). The researchers thank Sarah Ainsley, Jade Bilodeau, Jeanine Blanchard, Charles Boislard, Mélanie Boudriau, Mike Carlson, Mélanie Cauchon, Florence Clark, Céline Lajeunesse, Kevin Lalanne, Alexandra Marchand, Ginette Mercier, Claude Quintin, Stacey L. Schepens Niemiec, Marie-Ève Tardif, Lise Trottier, and Cheryl Vigen, as well as the older adults who participated in the study.
(NCT03398642). Free bus tokens were kindly provided by the Sherbrooke Transit Corporation. At the time of the study, Mélanie Levasseur was a Fonds de la Recherche du Québec-Santé Junior 1 Researcher (26815), and she is now CIHR New Investigator (360880). The researchers thank Sarah Ainsley, Jade Bilodeau, Jeanine Blanchard, Charles Boislard, Mélanie Boudriau, Mike Carlson, Mélanie Cauchon, Florence Clark, Céline Lajeunesse, Kevin Lalanne, Alexandra Marchand, Ginette Mercier, Claude Quintin, Stacey L. Schepens Niemiec, Marie-Ève Tardif, Lise Trottier, and Cheryl Vigen, as well as the older adults who participated in the study.