
Abstract
According to the Diagnostic and Statistical Manual of Mental Disorders (5th ed., or DSM–5; American Psychiatric Association [APA], 2013), children with autism spectrum disorder (ASD) are characterized by persistent impairments in social communication and interaction and restricted, repetitive patterns of behavior. Previous studies have shown that these social impairments can plausibly be explained by deficits in acquisition of theory of mind (ToM; Astington & Gopnik, 1991; Baron-Cohen et al., 1985; Leekam, 2016; Wellman, 1990). Because play is a main occupation of children, researchers have suggested that impairment in ToM may be associated with deficits in pretend play and with the reduction or absence of playfulness in children with ASD (Chan et al., 2016).
ToM is the ability to understand and infer the mental states (e.g., feelings, beliefs, desires, and intentions) of self and of others (Adolphs, 2001). It is a type of social cognition that enables people to explain, predict, or decide on corresponding behaviors (Jones et al., 2018; Premack & Woodruff, 1978), and it can be considered a prerequisite ability for the establishment of reciprocal communication and social interaction (Baron-Cohen et al., 1985). ToM helps children understand and distinguish emotional states and complex social information, and it also helps them to develop more complicated social skills, such as collaboration and metacognition (Preckel et al., 2018; Sally & Hill, 2006). ToM is essential for the development of interpersonal skills and for social development (Mazza et al., 2017; Wellman, 1990). Therefore, it is important for clinicians to consider ToM in planning interventions, as well as in monitoring the progress of children with ASD and evaluating the effects of intervention.
When environmental factors are considered, children’s ToM can be measured according to their capacity and performance (World Health Organization [WHO], 2006). The International Classification of Functioning, Disability and Health (ICF; WHO, 2006), defines capacity as what a child can do in a standard environment and performance as what a child actually does in his or her daily environment (Hutchins et al., 2016). The gap between capacity and performance reflects the difference between the impact of standard and daily environments and thus provides a useful guide as to how the child’s environment can be modified to improve performance (WHO, 2006).
Hutchins et al. (2016) proposed two additional constructs: explicit ToM and applied ToM. Explicit ToM is defined as ToM knowledge that is conceptual, operational, logical, and calculable in a limited experimental context. By contrast, applied ToM is defined as the ability to use ToM knowledge to successfully address ToM dilemmas in real-world day-to-day contexts (Hutchins et al., 2016). The ability to use logic to determine others’ mental state is no guarantee that one can or will apply the principles in daily life (Hutchins et al., 2016). Although the terms explicit and applied are not synonymous with capacity and performance as defined in the ICF, they draw on them. Because capacity and performance differ in concept and clinical utility, assessing both constructs could help users comprehensively understand a child’s ToM functioning.
Although ToM capacity and ToM performance are two different constructs, they are complementary. The ability to perform ToM well in a standardized context does not guarantee that a child can or will apply ToM skills in a day-to-day context (Hutchins et al., 2016). For example, a child who is able to perform a standardized task (e.g., from a storybook) designed to tap the understanding that people are happy when their desires are satisfied may, according to the child’s caregiver, be unable to translate this capacity into daily contexts because the child does not exhibit such behavior (e.g., recognize that others are happy) when interacting with others. Therefore, simultaneously assessing capacity and performance allows clinicians and researchers to gain insight into how capacity and performance are interrelated and to increase their understanding of children’s ToM function.
Previous studies have primarily focused on separately examining ToM capacity and performance in children with ASD (Baron-Cohen et al., 1985; Hutchins et al., 2016; Moran et al., 2011; Tager-Flusberg, 2007). To the best of our knowledge, only one study (Hutchins et al., 2016) has simultaneously examined both capacity and performance in boys with ASD and boys with attention deficit hyperactivity disorder (ADHD). However, the purpose of Hutchins et al.’s (2016) study was to examine the ToM profiles of children with ASD and children with ADHD and compare them with those of typically developing children. The study did not directly investigate the association between ToM capacity and ToM performance in children with ASD. A lack of knowledge regarding the relationship between capacity and performance in children with ASD make it difficult to ascertain whether children fail to perform ToM because of the complexity of their everyday environments or because of their ToM capacity. As a result, clinicians may not be able to focus interventions effectively.
In addition to external environmental factors, internal personal factors, such as the severity of autism traits and verbal comprehension, may affect a child’s capacity to use ToM in daily contexts. Several studies have demonstrated links between ToM capacity and severity of autism or verbal comprehension, providing preliminary evidence that greater severity of autism-related symptoms and lower verbal comprehension ability are associated with lower ToM capacity (Happé, 1995; Leekam & Perner, 1991; Ozonoff & Miller, 1995). However, these studies primarily focused on examining the associations between ToM capacity and the severity of autism traits or verbal comprehension.
Despite the fact that application of ToM occurs in daily social interactions, little research has examined the predictive power of the severity of autism and verbal comprehension on the ToM performance of children with ASD. Both ToM capacity and ToM performance are directly related to ToM functions. Thus, if children with ASD were able to use their ToM capacity in daily contexts, that capacity could possibly be equivalent to ToM performance. However, this is not often the case. Accordingly, factors other than ToM capacity (i.e., severity of autism traits and verbal comprehension) might cause the discrepancy between ToM capacity and performance. It is important to identify and verify such factors because doing so could assist in the development of therapeutic interventions for children with ASD to diminish the gap between ToM capacity and ToM performance.
The purpose of this study was therefore twofold: (1) to examine the discrepancies and associations between ToM capacity and ToM performance in children with ASD and (2) to verify the role of autism severity and verbal comprehension in predicting ToM performance when controlling for ToM capacity in children with ASD.
Method
Participants
We conducted a cross-sectional study between January 2015 and March 2016. Children with ASD between ages 3 and 12 yr were recruited from three hospitals and six pediatric rehabilitation clinics in southern and northern Taiwan. Participants were included if they had a diagnosis of autistic disorder or Asperger’s syndrome based on the criteria of the fourth edition, text revision, of the DSM (APA, 2000) or a diagnosis of ASD based on DSM–5 criteria made by a trained psychiatrist or pediatrician (APA, 2013). Participants were excluded if they were unable to follow orders or complete the procedures, had an uncorrected hearing or visual impairment, or had symptoms associated with organic brain dysfunction (e.g., seizures, cerebral palsy) or a chromosomal abnormality (e.g., Down syndrome).
To determine the proper sample size for the study, we conducted a literature review of cross-sectional studies and consulted with a statistician before data collection. On the basis of the literature and the statistician’s input, we determined that the minimum sample size for the cross-sectional study should be at least 50 to obtain an acceptable power of .80 (Astington & Jenkins, 1995; Pourhoseingholi et al., 2013; Salah El-Deen & Mahdy, 2017).
This study was approved by the institutional review boards of National Cheng Kung University Hospital (Reference No. B-R-104–094) and Chi Mei Medical Center (Reference No. CMNCKU10421). Written informed consent was obtained from each child’s caregiver and from children ages 7 or older.
Measures
Theory of Mind Inventory–2–Chinese Version.
We used the Theory of Mind Inventory–2–Chinese version (ToMI–2–C) to assess the children’s ToM performance (Jiang, 2016; Prelock et al., 2016). The ToMI–2–C contains 58 statements that belong to one of three empirically derived subscales (i.e., Early, Basic, and Advanced) that reflect a developmental progression in ToM development. For example, the Early subscale assesses ToM performance of sharing attention and affect recognition intentionality, which typically emerge in late infancy and toddlerhood. The Basic subscale assesses ToM performance of false beliefs and appearance–reality distinction, which typically emerge in the preschool years. The Advanced subscale assesses ToM performance of sarcasm, second-order false beliefs, idiomatic language, white lies, and humor, which typically emerge in late childhood but continue into adolescence (Prelock et al., 2016).
Responses for each statement are scored on a scale ranging from 0 (definitely not) to 20 (definitely) and averaged, with higher values reflecting greater degrees of certainty that the target child actually applied ToM across the range of the content surveyed (Hutchins et al., 2008). We adopted a cut score of 13 for determination of whether the child had or had not developed each ToM stage (i.e., not developed or early, basic, or advanced ToM; Prelock et al., 2016). For example, if a child’s score on the Early subscale fell below 13, indicating that the child had not yet developed ToM in the early stage, the child’s ToM performance was considered not developed (Prelock et al., 2016). The ToMI–2–C has been reported to have high test–retest reliability (.81) and internal consistency (.96). It also discriminates between age-matched children with ASD and typically developing children (t = 8.172, p < .01; Jiang, 2016).
Theory of Mind Task Battery.
We used the Theory of Mind Task Battery (ToMTB) to assess the children’s ToM capacity (Hutchins et al., 2008). The ToMTB consists of nine tasks in which children respond verbally to questions about a picture. The 15 test questions are organized into nine tasks that are arranged in order of ascending difficulty and in Early, Basic, and Advanced subscales. The tasks are variable with regard to content and complexity, ranging from the ability to identify facial expressions to the ability to infer second-order false beliefs (Hutchins et al., 2008). The tasks include memory control questions that must be passed in order for credit to be given on the test questions. Each question is scored as pass (1) or fail (0), with a possible total score of 15 (Hutchins et al., 2008). To compare scores on the ToMI–2–C and the ToMTB, we linearly transformed the cut score for the ToMTB; thus, a ToMTB cut score of 3 was needed to attain a certain ToM developmental stage (i.e., not developed or early, basic, or advanced ToM). The psychometric properties of the ToMTB have been well established. It has been reported to have a test–retest reliability of .94 and an internal consistency ranging from .91 to .94 (Hutchins et al., 2008; Jiang, 2016; Lai, 2016).
Social Responsiveness Scale, Second Edition.
We used the Social Responsiveness Scale, Second Edition (SRS–2), to assess the severity of autism symptoms (Constantino & Gruber, 2014; Gau et al., 2013). The SRS–2 consists of 65 items that can be divided into five subscales for clinical intervention (Social Awareness, Social Cognition, Social Communication, Social Motivation, and Restricted Interests and Repetitive Behavior). The SRS–2 is completed by caregivers. The items are scored on a 4-point Likert-type scale ranging from 0 (never true) to 3 (always true) according to the frequency of each behavior to quantify autistic traits. The raw SRS–2 score can be converted to a T score (mean = 50, standard deviation [SD] = 10), with higher scores indicating greater social impairment (Constantino et al., 2003). A T score of 60, 1 SD above the mean, is currently the SRS–2 cutoff for a diagnosis of autism traits. Standard scores ranging from 60–75 indicate mild to moderate autism traits; a score of 76 or higher falls in the severe autism trait range (Roberts et al., 2010). The Chinese version of the SRS–2 (Constantino & Gruber, 2014; Gau et al., 2013) has good reliability and validity. Its internal consistency is reported to range from .94 to .95. The test–retest reliability of the SRS–2 ranges from .75 to .85, and its convergent validity with the Chinese version of the Social Communication Questionnaire in Gau et al. (2013) ranged from .61 to .87.
Verbal Comprehension Index.
We assessed the verbal comprehension of children ages 4–6 yr and those older than age 6 yr using the Verbal Comprehension Index (VCI; Chen et al., 2009) of either the Wechsler Preschool and Primary Scale of Intelligence–Fourth Edition (WPPSI–IV; Wechsler, 2012) or the Wechsler Intelligence Scale for Children–Fourth Edition (WISC–IV; Wechsler, 2003), respectively. The WPPSI–IV is intended for use with children ages 2 yr, 6 mo–7 yr, 7 mo (Wechsler, 2012); we used the VCI Information and Similarities subtests. The WISC–IV is used to assess children ages 7 yr–16 yr, 11 mo; we used the VCI Vocabulary, Similarities, and Comprehension subtests. An index score ranging from 40 to 160 can be obtained, with scores of 90–109 considered average. The VCI was individually administered to the children.
We used the Chinese versions of the WPPSI–IV and WISC–IV in this study. Both have been reported to have good psychometric properties. The split-half reliability of the Chinese version of the WPPSI–IV ranges from .86 to .96, and test–retest reliability ranges from .72 to .89. It has good construct validity (Chen & Chen, 2013). The average reliability coefficient for Chinese version of the WISC–IV is .94, and test–retest reliability ranges from .89 to .93 (Chen et al., 2009; Wechsler, 2003).
Procedures
Before the study, the assessor (an occupational therapist) familiarized herself with the measures. Before formal recruitment began, the assessor practiced several times with an experienced occupational therapist (Kuan-Lin Chen) and completed a pilot study under supervision. The experienced occupational therapist has been working in pediatric occupational therapy as a clinician, educator, and researcher for 16 yr. The assessor was allowed to begin formal recruitment once the experienced occupational therapist approved her assessment skills. The assessor administered all the assessments. Data for each participant were collected in one visit. Depending on the child’s age, the VCI of either the WPPSI–IV or the WISC–IV was administered before the child was assessed with the ToMTB. The caregivers completed the basic information sheet, the ToMI–2–C, and the SRS–2.
Statistical Analysis
Descriptive statistics were used to describe the chronological age, severity of autism, and verbal comprehension of each participant. We examined agreement between the developmental stages of the ToMTB and those of the ToMI–2–C using χ2. In addition, we also calculated Pearson correlation coefficients to examine the relationship between ToM capacity (i.e., what the ToMTB assesses) and ToM performance (i.e., what the ToMI–2–C assesses). We considered r > .75 to indicate a strong correlation; r = .50–.75, a moderate correlation; r = .25–.50, a mild correlation; and r ≤ .25, a weak correlation.
We conducted a hierarchical regression model with a stepwise method to examine the significant predictors of ToM performance after controlling for ToM capacity. Therefore, in the first step of the regression model, the ToMTB was entered as a control variable, and the SRS–2 and VCI, as well as their two-way interaction, were entered in the second step. A two-sided p ≤ .05 was considered statistically significant. For the multivariate linear regression, we also checked the data for multicollinearity by means of the variance inflation factor (VIF). A VIF >10 is considered indicative of serious multicollinearity (Kutner et al., 2005). Data were analyzed with IBM SPSS Statistics (Version 17.0; IBM Corp., Armonk, NY).
Results
One hundred six participants were enrolled in the study. Of the 106 participants, 2 were excluded because they were unable to complete the ToMTB memory control questions, which left 104 participants who met the study’s inclusion criteria. The participants’ mean age was 77.6 mo, and 86.5% of the participants were boys. As shown in Figure 1, most children with ASD had ToM capacity in the early stage and ToM performance in the not developed stage. In addition, the children’s mean VCI score was 93.6 (SD = 23.2), and their mean SRS–2 score was 76.6 (SD = 10.3), indicating that, on average, participants were in the average range of verbal comprehension with high autism severity (Table 1).
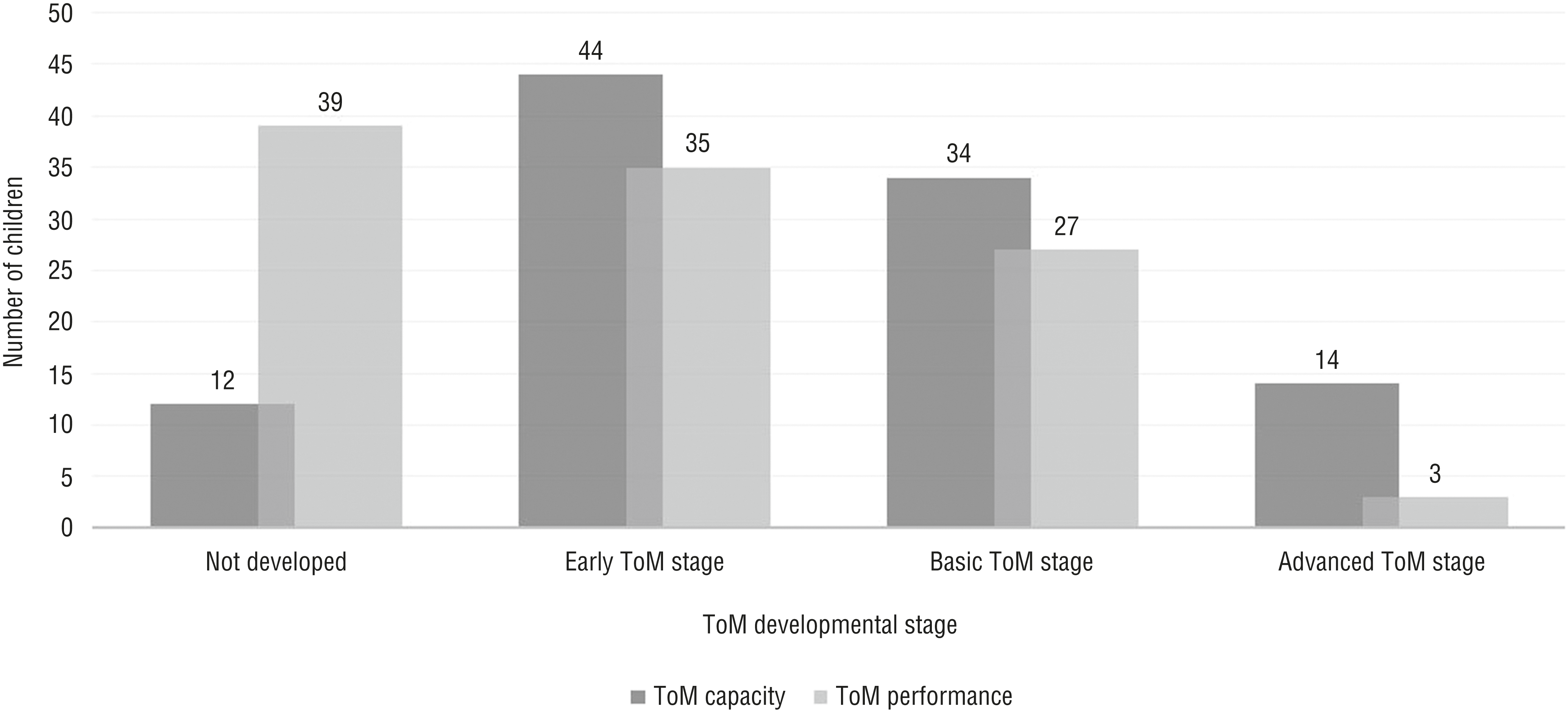
Developmental stages of ToM capacity and ToM performance in children with autism spectrum disorder.
Participant Characteristics (N = 104)
Note. — = not applicable; M = mean; SD = standard deviation; SRS–2 = Social Responsiveness Scale, Second Edition; ToMI–2–C = Theory of Mind Inventory–2–Chinese version; ToMTB = Theory of Mind Task Battery; VCI = Verbal Comprehension Index of either the Wechsler Intelligence Scale for Children–Fourth Edition or the Wechsler Preschool and Primary Scale of Intelligence–Fourth Edition.
To determine the differences between ToMTB and ToMI–2–C scores, we calculated the number of children with ASD at each developmental stage and compared their ToM capacity and ToM performance (Figure 1). The χ2 test showed that the number of children with ASD in the developmental stages of ToM capacity and performance were significantly different, χ2 = 104.594, p < .001. ToMTB and ToMI–2–C developmental stages disagreed for 75 children with ASD (72%). Of these 75 children, 74% had a ToM capacity developmental stage higher than their ToM performance developmental stage. That is, 18, 17, and 3 children with ASD were in the early, basic, and advanced ToM capacity stages, respectively, but their ToM performance had not yet developed. Thirteen and 4 children with ASD were in the basic and advanced ToM capacity stages, respectively, but their ToM performance was in the early developmental stage. Six children with ASD were in the advanced ToM capacity stage, but their ToM performance was in the basic developmental stage.
The ToMI–2–C was significantly and positively correlated with the ToMTB and the VCI (rs = .613 and .566, respectively, p < .01). In addition, the ToMI–2–C was significantly and negatively correlated with the SRS–2 (r = −.344, p < .01). The ToMTB was significantly correlated with the VCI (r = .667, p < .01). No significant relationship was found between the ToMTB and the SRS–2 (r = .05, p = .608). In addition, the VIFs were all <1.803 and therefore considerably lower than the recommended threshold of 10, suggesting that multicollinearity did not exist.
The results of the hierarchical regression model are summarized in Table 2. After controlling for ToM capacity, both the SRS–2 and the VCI made significant (p = .026) additional contributions to the prediction of children’s ToM performance. Both the SRS–2 and the VCI collectively accounted for an additional 16.4% of the variance in the ToMI–2–C. The SRS–2 × VCI interaction was not a significant predictor of performance on the ToMI–2–C.
Hierarchical Regression Analysis of the Chinese Version of the ToMI–2–C in Children With ASD (N = 104)
Note. — = no data; ASD = autism spectrum disorder; CI = confidence interval; SRS–2 = Social Responsiveness Scale, Second Edition; ToMI–2–C = Theory of Mind Inventory–2–Chinese version; ToMTB = Theory of Mind Task Battery; VCI = Verbal Comprehension Index of either the Wechsler Intelligence Scale for Children–Fourth Edition or the Wechsler Preschool and Primary Scale of Intelligence–Fourth Edition.
p < .05. **p < .01.
Discussion
Assessment of ToM capacity and ToM performance could provide clinicians with a clearer understanding of ToM functions in children with ASD. Our comparison of stages of development showed that ToM capacity and ToM performance differed from each other, supporting our hypothesis that the child’s capacity in a standardized context does not indicate that the child can apply ToM skills in a daily context. In addition, we found a significant positive correlation between overall score on ToM capacity and ToM performance. Our results also confirmed that both severity of autism traits and verbal comprehension were two significant predictors of ToM performance, aside from the influence of ToM capacity. This study fills important gaps in the previous research and furthers understanding of the relationship between ToM capacity and ToM performance in children with ASD.
The results of this study showed that for close to three-quarters (72%) of the children in our study, disagreement existed between the developmental stage of ToM capacity and that of ToM performance. Of this 72%, 74% of the children with ASD were found to have a higher ToM capacity developmental stage than their ToM performance developmental stage. Only 12 children with ASD had not yet developed ToM capacity; however, 39 children with ASD had not developed ToM performance (Figure 1). These results could imply that those children might have difficulty generalizing their ToM capacity to daily life. Caregivers in our study reported that even though their children succeed on ToM tasks, they have difficulty using their ToM skills in everyday life. This discrepancy between ToM capacity and ToM performance developmental stages provides useful information that clinicians could use to probe for more details and identify the possible underlying causes of difficulty in performing ToM.
It is worth noting that about 27% of the children with ASD had a higher ToM performance developmental stage than their ToM capacity developmental stage. We propose two possible reasons for this. First, the unfamiliar environment in which the children with ASD were assessed could have affected their performances on the ToMTB tasks. It has been reported that, in unfamiliar environments, children with ASD may be unable to process a lot of information and thus may have difficulty concentrating on the tasks (Kasari et al., 2013). However, according to the caregivers’ ToMI–2–C reports, the children in our study were able to demonstrate their ToM skills in their daily environments. On the basis of our findings, then, to truly understand the ToM function of children with ASD, it is essential to assess both ToM capacity and ToM performance.
Second, social motivation may account for the discrepancy between ToM capacity and ToM performance (Kasari et al., 2013). The children may have had the ToM capacity but may not have been motivated to use it in a laboratory context. If this is the case, it is possible that the ToM capacity of the children with ASD in our sample could increase when they are motivated. This issue is particularly important for early intervention because it could indicate that ToM abilities are present but not automatically activated in children with ASD. However, because we did not directly measure social motivation, we cannot state with certainty that the ToMTB scores (assessing ToM capacity) of children with ASD could be increased by social motivation. Future studies are needed to examine the role of social motivation in ToM functioning.
Because no single measure can perfectly capture the complexity of ToM, we used the ToMTB and ToMI–2–C to simultaneously assess ToM capacity and ToM performance of children with ASD, in light of the fact that environmental factors may influence the ToM function of children with ASD (Hutchins et al., 2016). Both measures cover a wide range of ToM content areas and vary in conceptual complexity. In addition, although the ToM concepts assessed by the two measures are not identical, they overlap considerably, which makes comparison of these two ToM functions much more straightforward. For example, both measures have an Early subscale intended to capture the ToM skills that emerge in typical development between ages 1 and 3 yr, a Basic subscale intended to assess the ToM skills that emerge in the preschool years (ages 3–5.5 yr), and an Advanced subscale to assess the ToM skills that emerge in later childhood (ages 5.5–8 yr; Hutchins et al., 2016). The discrepancy in the results for ToM capacity and ToM performance developmental stages could be useful in clinical reasoning and intervention, which may result in better treatment outcomes. Therefore, we strongly suggest that the ToMTB be used in conjunction with the ToMI–2–C to facilitate comparison and comprehensively measure all aspects of ToM function in children with ASD.
We found that ToMTB scores were significantly and positively correlated with ToMI–2–C scores, indicating that children with better ToM capacity may have better ToM performance, and vice versa. Indeed, the emerging ToM capacity of children with ASD may serve as a foundation for them to use their ToM skills to attribute states of mind and predict others’ actions and thus adjust their behavior accordingly (Pellicano, 2007), which may greatly enhance their ToM performance in daily contexts. Likewise, improving ToM performance could expose children with ASD to social situations that might drive advances in ToM capacity. The resulting information regarding the ToM capacity and ToM performance of children with ASD could be useful to clinicians in developing an appropriate intervention, which may result in better intervention outcomes.
After controlling for ToM capacity, the results of our regression analysis showed that SRS–2 score contributed to the predictive power of ToM performance. This result suggests that the children with ASD in our study who exhibited less severe autism traits had better ToM performance. It has been observed in clinics that children with more severe autism-related symptoms tend to be less able to understand others’ intentions. For example, children with ASD might have difficulty recognizing when someone needs help (an early ToM skill). The autism traits measured by the SRS–2 concern the core features of ASD—social communication and interaction, restricted interests, and repetitive behavior (Constantino et al., 2003)—all of which affect children with ASD when performing ToM in daily contexts. The results of our study provide further understanding of how severity of autism traits affects ToM performance in children with ASD.
Moreover, we also found that the verbal comprehension of the children in this study was a strong predictor of ToM performance. This finding indicates that children with better verbal comprehension may have better ToM performance. Because children’s verbal comprehension involves not only verbal reasoning but also knowledge of word meanings, both of which are needed in social contexts (Constantino et al., 2003), it is critical to improve the verbal comprehension of children with ASD so that they can understand the minds of others and predict their behaviors. Overall, our findings have important implications for early interventions targeting verbal comprehension, which would greatly support the application of ToM performance.
Three limitations of the current study are acknowledged. First, all the children with ASD in this study were verbal, so the findings cannot be generalized to nonverbal children with ASD. Second, the cross-sectional study design did not allow us to draw causal inferences from the data. Future studies that include nonverbal children with ASD and that examine the longitudinal relations between ToM capacity and ToM performance are needed to confirm our cross-sectional findings. Third, even though parents can be reliable reporters, they are also subject to bias and subjective rating when it comes to rating their children’s behaviors. Thus, a cautious interpretation is recommended. Future studies comparing direct testing by an examiner with responses obtained through a caregiver survey are needed.
Implications for Occupational Therapy Practice
Knowledge of the predictors of ToM performance could guide clinicians to more effectively improve ToM performance in children with ASD. Our study has the following implications for occupational therapy practice:
It is important to assess ToM capacity and ToM performance simultaneously in children with ASD to help practitioners gain a comprehensive understanding of a child’s ToM functioning.
Enhancing the ToM capacity of children with ASD could promote their ToM performance.
Both severity of autism traits and verbal comprehension were significant predictors of ToM performance, independent of the influence of ToM capacity.
Conclusion
Our study provides insight into a possible difference and association between ToM capacity and ToM performance in children with ASD. Enhancing the ToM capacity of children with ASD would be beneficial because ToM capacity is significantly correlated with ToM performance. In addition, we found that both autism severity and verbal comprehension were important predictors of ToM performance even after controlling for ToM capacity. Knowledge of the predictors of ToM performance could guide clinicians to more effectively improve ToM performance in children with ASD. Our findings provide useful information that could help clinicians in the process of planning ToM interventions.
Footnotes
Acknowledgments
We are thankful to the caregivers and children for participating in the study. We are grateful for assistance from the Department of Rehabilitation, Country Hospital, Division of Rehabilitation, Der Shang Clinic, and Department of Child and Adolescent Psychiatry, Kaohsiung Municipal Kai-Syuan Psychiatric Hospital. This research was supported by Ministry of Science and Technology Grants 103-2410-H-006-060, 104-2410-H-006-065, 104-2811-H-006-009, and 105-2410-H-006-047-MY2 awarded to Kuan-Lin Chen.