
Abstract
Provision of powered wheelchairs (PWCs) to promote independence for people with limited mobility is dependent on a variety of factors, including user characteristics (e.g., cognitive and perceptual abilities, diagnosis, prognosis), features and programming of the PWC, and the living environment (Karmarkar et al., 2012; Mortenson et al., 2013). To operate a PWC safely, people must be able to negotiate the environment (e.g., avoiding obstacles, engaging with others, and anticipating others’ actions) and recognize when assistance is needed (Canning & Sanchez, 2004). To access a PWC through a clinical practitioner, the user typically must demonstrate competence during a device trial (Mortenson et al., 2005). After the trial, training may be offered to address limitations in driving ability. In a study investigating guidelines for PWC use in residential care, a majority of respondents felt that more in-depth training was required to determine suitability for PWC use (Mortenson et al., 2006). However, training is often constrained by clinician time and availability of evidence-based approaches.
Evidence-based protocols to guide clinicians in PWC training are limited. The Wheelchair Skills Program contains training suggestions and skill progression for 30 powered mobility skills (Kirby et al., 2016). However, this protocol does not address “soft” driving skills, including navigating the social environment (e.g., negotiating right of way) and driving-related judgment. Driving to Learn consists of guidelines that focus on training needs of children or adults with severe cognitive impairments; however, the focus is on PWC use as a therapeutic tool rather than a means of mobility (Nilsson & Eklund, 2006).
For trainers not using systematic protocols, a survey suggests many follow a similar progression. Basic skills, such as driving in a straight line and stopping, are practiced first in an open environment. More complex skills, such as navigating an elevator, are initially attempted in quiet environments or simulated spaces until the person demonstrates competence. After a trainer is confident that the person can perform the skill safely in a simple environment, it will be attempted in more complex or realistic environments (Smith et al., 2017).
Training in PWC use is typically based on trial-and-error methods, in which trainers identify errors made during a task and provide interventions to address difficulties or errors made by the learner (Smith et al., 2017). Interventions may include verbal or physical (hand-over-hand) instructions to overcome the error or reprogramming the PWC motors and joystick to compensate for specific challenges. However, trial and error may not be optimal for learners with memory-related cognitive impairments. Trial-and-error methods are thought to interfere with the creation of memories for people who have difficulty forming explicit (knowledge-related) memory, including those with dementia (Baddeley & Wilson, 1994).
Cognitive impairments associated with dementia affect 56% of people older than age 80 yr and living in residential care, where many residents may benefit from PWC use (Chambers et al., 2016). Reducing error during learning through error-minimized or errorless learning strategies—including modeling, cued learning, forward and backward chaining, and spaced retrieval—may facilitate procedural learning for people with cognitive impairments (Kessels & Hensken, 2009; Mount et al., 2007). Advances in technology provide an opportunity to explore the potential for error-minimized training through training protocols more suited to their learning needs.
Because of limitations in existing training protocols and clinical time available, people with cognitive impairments may not receive training to address specific driving and learning needs (Mortenson et al., 2013). Moreover, trainers may be hesitant to engage in PWC training with these people because of concerns that they will not be able to respond effectively to safety issues. As a result, people with cognitive impairments may not be given the opportunity to demonstrate their potential abilities with PWCs. Novel interventions allowing clinicians to provide low-risk PWC assessment and training may address this challenge.
The CoPILOT (Collaborative Powered mobility Innovative Learning OpporTunity, a prototype technology developed in collaboration with the University of British Columbia, McGill University, and University of Toronto) remote is a novel teleoperation device that provides the trainer with the opportunity for shared control of a PWC. Shared control over a PWC allows simultaneous control between the user (driver) and the clinician (trainer) without the need to switch between modes on the wheelchair. With the shared-control remote, the trainer can override the PWC user’s speed and direction remotely as needed and can perform emergency stop maneuvers, providing increased control. Moreover, data regarding driving behavior (i.e., collisions and near-miss events) and interventions by the trainer (i.e., emergency stops or adjustments to speed and direction) may be collected electronically and used to inform training or prescription decisions.
These features may change the dynamic between the trainer and the PWC user in the training and assessment process. Similar technology is used in vehicle driver training for cars and pilot training. For these devices, overriding controls of the driver provides opportunities for skill demonstration and reduces risk by allowing the trainer to assist the learner when there is undue or unanticipated risk or difficulty. Despite the potential benefits of using shared control, there appears to be no published evidence demonstrating this approach for potential PWC users. The objective of this study was to explore clinicians’ perceptions about how a shared-control teleoperation device for PWCs could be used in a clinical setting and developed further for use during training.
Method
This article includes data collected as part of a larger qualitative study on the design of the CoPILOT remote and training program. Sequential semistructured interviews were the primary means of data collection. Ethical approval was obtained from the Behavioral Research Ethics Board of the University of British Columbia.
Participants and Settings
Participants were included who were occupational therapists or physical therapists with at least 2 yr experience providing powered mobility. Participants were recruited purposively for maximum theoretical variation in expertise (i.e., length of time practicing, practice settings, years of experience) and populations served (i.e., level of care, diagnoses).
Data Collection
We collected data using two semistructured interview guides (Figure 1). The first interview focused on the participant’s perceptions of the utility of shared-control technology. A verbal explanation of shared-control teleoperation was provided after questions regarding perceptions of the technology based solely on the description. A minimum of 2 wk after the initial interview (no longer than 4 wk), a second interview was conducted with a subset of participants who were provided an opportunity to observe operation of the device and to experience driving the PWC using the shared-control remote. Because of constraints with moving the PWC, participants were included for the second interview if they were able to attend the in-person observation and experience to provide feedback. Open-ended questions were used to elicit perceptions of the prototype and to explore the potential use of the technology in practice.
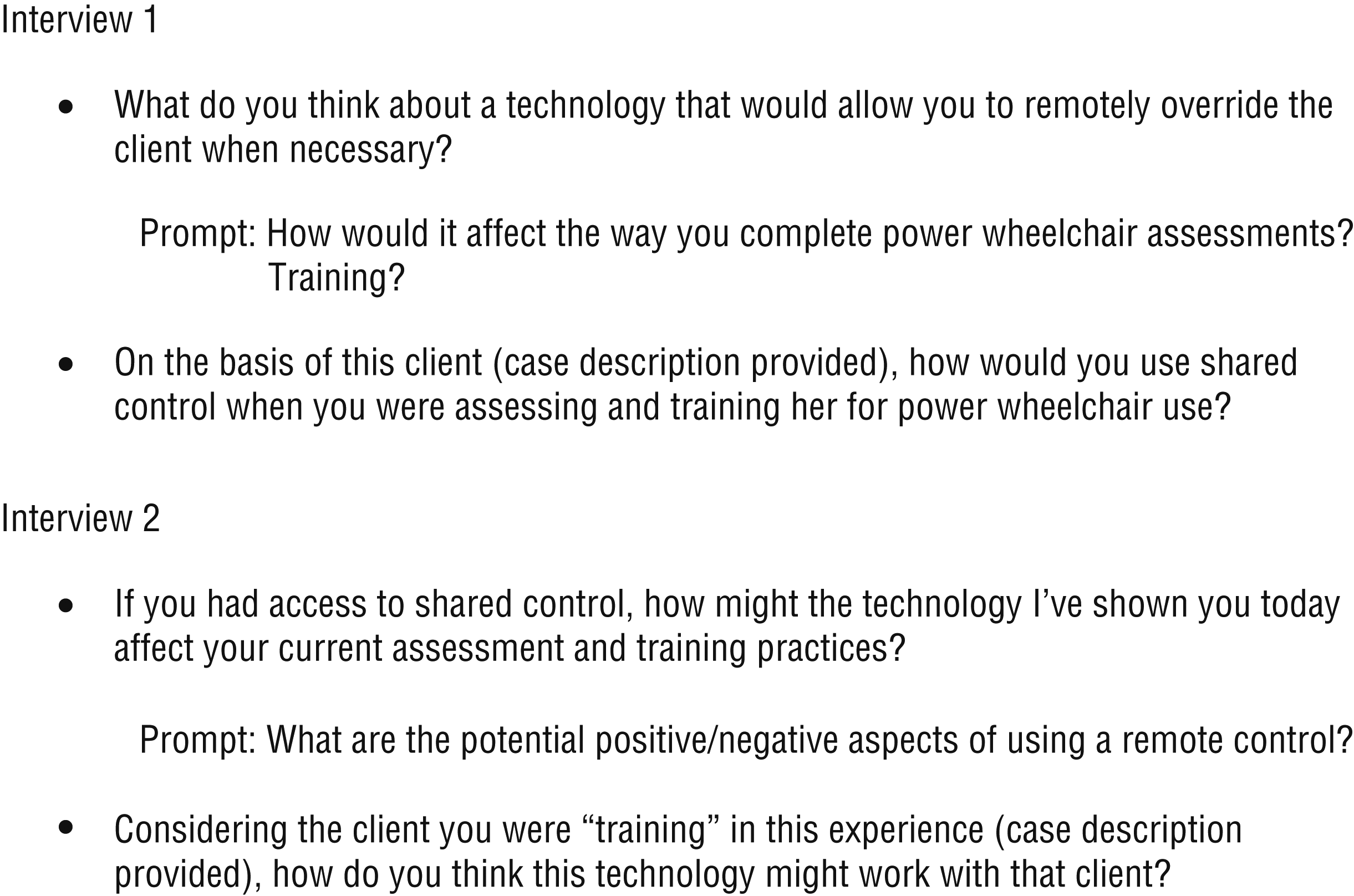
Sample interview questions.
A clinician experienced in PWC provision and conducting qualitative research, including semistructured interviews, and an engineer with experience in usability testing and product development strategies conducted the interviews. This method provided both insider and outsider perspectives and an opportunity for in-depth probing of both clinical and technical questions.
Analyses
Interviews were audio recorded and transcribed verbatim, and line-by-line coding was performed with each document. Codes were developed independently by two trainee investigators (Smith and Rismani) using an inductive process and were then aggregated into themes. Initial codes were grouped into preliminary categories, discussed by two investigators (Smith and Mortenson), and revised accordingly. Preliminary categories were then reevaluated to ensure consistency with the data and to address overlap. Final themes were reviewed to ensure that they were exclusive and represented conceptual areas related to the clinical utility of PWC shared control.
Trustworthiness
To support trustworthiness of the data and analysis, we used strategies including member checking, triangulation, and reflexive discussion (Morrow, 2005). Member checking was used in initial interviews to confirm understanding and in follow-up interviews to confirm that the preliminary analyses aligned with the participants’ perceptions. We performed triangulation of informants and investigators by engaging informants from multiple practice settings and client populations through purposive sampling (Kuper et al., 2008), by using multiple interviews in an iterative process (Kuper et al., 2008), and by conducting frequent debriefings between interviewers and supervisors. Interpretation was guided by one investigator’s experience as an occupational therapy practitioner with experience in the field (Shenton, 2004) and an alternative perspective from an engineer working outside the clinical field (the second author) who could question assumptions made during the data collection and analysis process.
Because the research team was optimistic about the potential of the new technology, the guides were created to avoid leading questions in the interviews and were probed for cases that diverged from our expected outcomes. To address the potential impact of one investigator’s familiarity with the culture of the participants, we used reflexive discussion to establish a mutual understanding of the data and presented both convergent and divergent data in our reporting. Although there is some expectation of subjectivity within qualitative data analysis, reflexive discussion and analysis help to limit the potential of undue influence of a single perspective (Morrow, 2005).
Results
As reported in Table 1, 15 clinicians participated in the first interview, and 10 of these clinicians participated in the second interview. The majority were female (n = 12) and were occupational therapists (n = 14), with clinical experience ranging from 3 to ≥20 yr. Participants worked in a range of practice environments, and approximately half worked in residential care. Areas of practice varied, including neurology, older adults, acquired brain injury, spinal cord injury, and developmental disabilities.
Participant Demographics
Note. ABI = acquired brain injury; F = female; M = male; PWCs = powered wheelchairs; SCI = spinal cord injury.
Length of time practicing and years working with people in PWCs were rounded to the nearest 5-yr interval to protect participant anonymity.
This participant was a physical therapist; all other participants were occupational therapy practitioners.
The analysis identified two overarching themes. The first, “a big enabler,” described how shared control provides opportunities to train people who may otherwise be denied access to powered mobility. It included three subthemes: reducing training-associated risk, enabling alternative training and assessment approaches, and necessary clinician training and practice. The second theme, “changing the learner experience,” described how shared control may promote success in skill development by changing the learning experience. This theme included four subthemes: reducing anxiety, stress, and frustration; building confidence through success; changing the training relationship; and mitigating drawbacks to shared control.
A Big Enabler
All participants felt that shared-control technology would provide new opportunities for clients and trainers in the assessment and training process. One of the benefits described by participants was the potential for the technology to be “a big enabler,” giving people who might not otherwise be afforded the opportunity a chance to try it. Natalie, an occupational therapist with considerable experience working with older adults in a long-term care setting, described this challenge:
There are people we write off pretty quickly. They can’t see well enough, they don’t have enough . . . discrete control, they can’t stop . . . .I think it would enable a population of people that you would be afraid to . . . give an opportunity [to try power mobility].
Caitlin, another experienced occupational therapist working in long-term care, described how this opportunity may give the learner a better understanding of his or her own capabilities: “[Shared control would be able to] give them [new PWC users] the ability to just try it out. They might even realize themselves that it’s just not a good idea.” Thus, she suggested that both trainers and new PWC users may benefit from learning more about the PWC user’s driving capabilities.
All participants described the potential of the shared-control remote to reduce training-associated risk for the PWC user, the trainer, and others in the environment. This subtheme was summarized by Rebecca, an occupational therapist with experience with older adults living in the community, who noted, “I always struggle with assessing people in a crowded situation. Because I need to know they’re safe . . . but in order to figure out if they’re safe, I have to potentially put people at risk.” The opportunity to reduce risk for multiple stakeholders was identified as a primary positive outcome of the use of the shared-control technology. Related to reduction in risk, all the participants interviewed thought that the shared-control remote would allow them to provide training in more complex, real environments earlier in the training process. As Natalie described,
It would be beautiful in the summer time, and I’m a little uncomfortable with them going somewhere, and [we] stick indoors. But wouldn’t it be nice to be able to go outside? . . . [Then it would be possible to] . . . progress somebody into [the] real world a bit quicker and then be able to really start to see what they are capable of.
Roger, a community occupational therapist working with adults, described how shared-control technology might help address the challenging realities that he encounters during training and assessment: “Getting into busier environments with noises and bright lights and dogs that bark, and all that kind of stuff, that’s the meat and potatoes of life, right? So I can really see how someone is doing with those extra challenges.” Rebecca also noted the benefits of practicing in a real environment:
Right now I do that [simulated crowded or busy environment] with a lot of dining room tables and chairs. Which is not the same thing as little old ladies and walkers. People react differently . . . people aren’t chairs; they move, they’re unpredictable.
For these participants working in the community, without access to “safe” learning spaces, complex environments were a daily reality. Jennifer, an occupational therapist working in acquired brain injury in community care, addressed the challenges she faced:
I don’t really have a choice [about where to train someone]. I’ve done a little bit in their foyer and in their driveway or whatever it is that we have, but then we have to venture out, and we have to deal with these busy areas, so that would certainly make it easier. I think that would give both myself and the client more confidence.
Increasing confidence for the trainer and the learner was also identified as part of the changing the learner experience theme.
Various features of the technology were perceived to enable alternative training and assessment approaches. Two-thirds of participants described how being able to get further away from the client, or to be able to observe the client from a different perspective, would be beneficial for their assessment and training processes while allowing the trainer to maintain safety. Roger indicated that it would be helpful to gather additional information about the client’s driving capabilities by seeing the client from a different perspective:
I am rarely in front of the chair when [the client is] operating, but being in front of the chair gives me a good sense of where they’re looking . . . and what they’re attending to. That gives me a lot of information.
The capacity to be further away from the chair also provided him with an opportunity to “get an understanding of what the client might do if you weren’t around,” an opportunity that he indicated was rarely afforded in traditional PWC assessments.
Participants discussed the potential for the technology to enable training approaches that are not possible without remote override or operation. For example, trainers could use the technology to teach specific skills using collaborative training techniques. Natalie shared a specific example of how the shared-control remote could be used to train a PWC user to navigate an elevator:
Let’s say a person is lining themselves [up] to go [into an elevator]. I could move the joystick a little bit, I could give a verbal prompt . . . and then the person could successfully navigate rather than having to totally take over for them.
Caitlin, an occupational therapist working in residential care, discussed the benefit of being able to provide sequential learning experiences: “In the beginning stages, maybe it’s just better that they get used to a chair and not have to worry about a collision.” The complexity of the tasks required of the client could then increase over time while allowing the learner to stay in a familiar environment. Other participants spoke about the opportunity to demonstrate challenging tasks to allow the client to feel the correct movement.
Participants identified opportunities to use data, which could be collected by the technology during the training and assessment process, to inform their assessment and to justify their clinical decisions. Rebecca noted, “it might be useful to see how many times I have to assume control. Then that could be useful, especially in justifying to [residential care] facilities that this person can . . . learn, can use their power wheelchair.” Elizabeth, an occupational therapist in residential care who indicated that she was often hesitant to trial clients with powered mobility, stated that “[these data] would impact me. Maybe there [would be] more people in a chair that I would try than otherwise. People who I had more doubts about.” Data collection was seen as a starting point for intervention and education. Chris, an occupational therapist working in inpatient rehabilitation, thought that it “might provide me with more information to make adjustments to the chair,” a strategy he commonly uses to ensure safe and competent driving experiences in the early stages of learning.
For shared-control technology to provide benefits in a clinical environment, participants also stressed the fact there would be a necessity for training and practice for the clinician to operate the controller successfully. After an experience using the prototype device, 1 participant noted that it was “a bit nerve wracking when I was trying to control it.” This outcome was particularly true for participants who were less familiar with remote controlled and video game technologies. Chris, who had substantial experience with joystick-based gaming, stated that “I have more familiarity with the . . . controller than some clinicians, so I think that puts me at more of an advantage. I don’t really have to look at the controller to know what I’m pressing.” Jillian, who had less related experience, noted,
I would need to work with it fairly regularly to be comfortable enough to . . . be in a crowd . . . and be confident that I could control the chair for them. I think it would take a bit of practice on my part.
All participants identified training and practice as a strategy to mitigate the challenge of working with a novel technology.
Changing the Learner Experience
Most participants anticipated the positive impact that a shared-control device could have on a client’s psychological state during training. Eleven of the 15 participants described the potential for the technology to reduce training-related anxiety, stress, and frustration. Anxiety was perceived as having a negative impact on learning. Jennifer, a community occupational therapist working with people with acquired brain injury, noted that “people don’t learn well when they’re anxious or have panic and things aren’t going well.” Elizabeth, who worked with older adults, described being able to provide an opportunity for their “mind [to be] in a state of being able to take in information.” For those clients who were intimidated by the prospect of using a PWC, Chris thought that a reduction in stress might “make clients maybe a bit more willing to learn . . . knowing that I have control of the chair at all times.” Natalie elaborated on this concept, describing the experience of an older adult PWC user with no previous experience with the device:
There is all this new learning, and so it’s frightening . . . and then you have a bad, bad bump, and then they don’t want to do it anymore. Or it gets disheartening or frustrating. And so because you . . . can’t get out of their room, you can’t get to the places where they want to be. The total time that they are in the chair, they have not had any success.
These unsuccessful experiences were seen to be detrimental to learner progress and motivation, which might affect training outcomes.
All but 3 of the participants described how shared-control technology could help to build confidence through successful experiences, which may promote learning. Jennifer focused on the importance of success in learning:
If we don’t have success then . . . we can’t move onward from where we are, right? Because you just keep having failure, and failure, and failure, and so how do you get to that point where you start demonstrating some success?
Success was seen as promoting engagement in training, with participants noting that the technology would allow them to take more managed risks. Agnes, an occupational therapist working in residential care, felt that this concept was important to maintaining engagement because “with more risk always comes more reward . . . and if . . . there’s this perceived risk, and they’re successful, then they’re willing to continue to try and to stay engaged in the process.” Sarah, who also worked in residential care, noted,
If you can make those things of what could be considered a difficulty skill easier, successful, then the confidence is built sooner. And I think that’s a big part of successful wheelchair training, is the client developing the confidence to do it.
Although participants did describe opportunities to build confidence, Agnes noted the potential for a client to develop “way more confidence than they should have” from training in a reduced-risk environment.
Confidence was not only related to the client’s experiences but also to the trainer’s own confidence and willingness to engage in training. Jillian noted that the technology “would just give confidence, really, to both me and the person I was training. I think it could give a little bit more confidence with that process of . . . reducing the risk of harm.” Increased confidence for both the trainer and the learner was identified as having potential to change training outcomes.
Shared-control technology was seen as an opportunity to change the relationship between the clinician and the client. Natalie felt that this could be accomplished by allowing the trainer “to still be there and support [clients] but [give] them a little more room.” Rebecca described how the device would allow them to “walk beside her [the client] and have a more normal relationship with somebody in a wheelchair.” Moreover, Jillian described situations in which the client might be stuck in a tight space and how the device would allow her to come to the client’s aid: “It would help . . . maintain the dignity within the process.” Most participants felt that the change in the nature of the relationship could have a resultant impact on learning.
Participants also identified the importance of mitigating drawbacks to using shared control, including the client’s potential difficulty understanding the behavior of the chair when the trainer was overriding. Chris questioned whether
they are going to necessarily make that correlation between them [the chair’s action and the trainer’s input], or are they just going to do it the same way the next time because that’s what they did [when the chair produced that action]? How are they going to be able to relate what the therapist is doing to what they [the client] are doing?
Eleanor, an experienced occupational therapist in residential care, stated that “if they thought they were going this way, when all of a sudden they’re going some other way, they wouldn’t want to learn. They would need some good feedback on why that’s happening.” Participants stressed the importance of communication and feedback between the trainer and the client to mitigate this drawback. Challenges providing feedback to the client represent potential limitations to the technology.
Two participants who worked in community settings described the importance of preventing reliance on the shared-control system when trying to develop independent driving skills. Specifically, it would be important to carefully consider when to wean the client off the assistance. As Jennifer stated, “If a person feels some sense of security with me being there, well, I’m not going to be there once the chair’s delivered.” Rebecca indicated that “it would be easy to take too much control away from the client. The therapist would have to really be aware . . . to let the client get to the point where they are correcting their own mistakes.” The perceived need to allow the client to make mistakes was the most commonly cited concern by participants.
Discussion
Shared control is a novel approach to powered mobility training and is, therefore, a unique contribution to the field. Participants were generally positive about the potential uses of shared-control teleoperation for clients in PWCs. They also identified opportunities to enhance the assessment and training process as well as the client’s experience.
People with cognitive impairments may be denied powered mobility on the basis of a presumed inability to learn or to drive competently. In residential care, as many as one in two residents require a wheelchair for daily mobility (Shields, 2004). Given the number of people with cognitive impairments living in residential care (Chambers et al., 2016), it is reasonable to assume that many of those who require a wheelchair for mobility also experience some cognitive impairment. Offering an opportunity to try powered mobility to people who experience both conditions may improve their overall health and quality of life. Although there is limited evidence on learning powered mobility in this population, a few studies have demonstrated capacity for learning the required skills among older adults with cognitive impairments (Hall et al., 2005; Mountain et al., 2010).
Learning to drive is not without risk because of challenges in the client’s environment (Mortenson et al., 2006). Safety is frequently maintained through proximity of the trainer, who may intervene by removing the user’s hand from the joystick or by turning off the chair (Kirby et al., 2016). This proximity can be difficult to maintain in tight environments or at higher speeds. In addition, learners rarely experience driving without a trainer nearby until the trainer is confident in their abilities. Therefore, training may not adequately prepare clients for an independent driving experience. Shared control may help to ensure safety in the assessment and training process and permit a more in-depth understanding of a user’s capabilities.
When learning procedural skills, there is evidence that transfer of learning to new environments may be difficult for people with Alzheimer’s disease or related dementias (Bier et al., 2008). Therefore, learning in the environment where the skill will be used, rather than simplified or simulated environments, may be important for success. Shared control can facilitate safe opportunities to increase complexity within an ecologically valid environment.
Shared control may provide opportunities for alternative training and assessment approaches, including skill demonstration, increasing complexity of skills over time, and providing targeted feedback to the user. These concepts show similarity with the principles of errorless learning, which have been shown in a literature review to have beneficial effects on learning procedural skills in people with mild cognitive impairment and dementia (de Werd et al., 2013). Many of the techniques used in errorless learning (e.g., modeling and demonstration; cueing to the correct response; stepwise, graded, or chained learning) focus on providing successful experiences of task completion and are similar to alternative training approaches identified by the participants (de Werd et al., 2013). Therefore, in future studies, researchers may explore a potential clinical role for shared control in facilitating errorless learning approaches.
Clinical outcomes in powered mobility training are also likely to be influenced by the experience of the client throughout the training process. Experiences of anxiety, stress, and frustration associated with learning a new skill may impair learning. Studies have shown that anxiety interferes with processing effectiveness and retention, both of which are required for successful learning (Eysenck, 1979; Eysenck et al., 2007). Shared control may provide opportunities to reduce training-associated anxiety and frustration while providing opportunities for success using error-minimized training techniques.
One potential barrier to the adoption of shared control as a training tool is the challenge of introducing new technologies into a clinical setting. In a study of technology use and acceptance, rehabilitation therapists found that clinicians were more likely to adopt technologies that enhanced their job performance or client’s outcomes (Liu et al., 2015). These factors may override the concerns associated with learning and training on the new technology. Although participants were positive about the potential utility of shared control in training, the familiarization of the trainer with the technology will be important to provide competent care. Future research focused on the efficacy of shared control in a clinical setting, as well as client and clinician perspectives of the technology, will provide evidence about the use of shared control as an assessment and training tool for PWC users and increase the likelihood of adoption.
Limitations
This study has two main potential limitations. First, the findings represent only the perceived clinical utility of the technology and not the clinicians’ experiences using it in practice. Second, the interpretation of the data was influenced by the experience and expectations of the investigators in addition to our research knowledge. To address this limitation, we used strategies to enhance trustworthiness of the data and analyses, including collaboration between a clinician and an engineer to minimize discipline-specific bias and to identify complementary understanding. Sampling for maximum variation addressed concerns with sample size by ensuring that participants represented a range of experience.
Implications for Occupational Therapy Practice
The findings of this study have the following implications for occupational therapy practice:
Shared-control training may provide participation opportunities for people who would be otherwise unable to mobilize independently.
Shared control may reduce risk in powered mobility assessment and training.
Shared control may facilitate alternative training approaches, which are well aligned with occupational therapy approaches including grading and chaining.
In the implementation of technologies to support powered mobility training, occupational therapy practitioners will require training and practice to ensure competence in service delivery.
Conclusion
Shared control may have the potential to broaden the scope of therapeutic intervention by reducing risk and facilitating alternative training approaches. Participants identified the potential for positive psychological impacts on learning, practical implications on the training process, and potential risks of device use. Future research should focus on the use of shared-control technology in practice, with novice PWC users, to address both outcomes associated with training as well as client and clinician perceptions of the shared-control technology.
Footnotes
Acknowledgments
This study was supported by a grant from the Canadian Occupational Therapy Foundation. Emma M. Smith is supported by a Canadian Institutes of Health Research Fellowship. Emma M. Smith, W. Ben Mortenson, Alex Mihailidis, and William C. Miller are supported by AGEWELL NCE. W. Ben Mortenson is also supported by a Canadian Institutes of Health Research New Investigator Award.