
Abstract
This study examined whether sleep quality is associated with hand function above and beyond what can be explained by the effect of pain and carpal tunnel syndrome (CTS) severity on hand function in clients with CTS. The sample included 53 adults ages 30–86 yr. The Manual Ability Measure–20, Pittsburgh Sleep Quality Index, visual analog scale for pain, and electromyography for CTS diagnosis and severity level were used to measure outcomes. Sleep quality was significantly associated with manual ability after controlling for CTS severity and pain. In CTS care, attention to sleep is significant because it may promote hand function.
Nearly 5 million American workers each year are affected by the often debilitating disorder of carpal tunnel syndrome (CTS; Luckhaupt et al., 2013). CTS occurs when the median nerve is compressed in the carpal tunnel. The median nerve, along with nine flexor tendons, traverses through the carpal tunnel, which is less than 1 in. wide. It is therefore no surprise that CTS is the most common median nerve entrapment neuropathy, affecting 3% of the general population (Atroshi et al., 1999).
Sleep disturbance is considered a health crisis by the Centers for Disease Control and Prevention (2017). Poor sleep quality is associated with “elevated multisystem biological risk” (Carroll et al., 2015, p. 184). The American Academy of Sleep Medicine confirmed that 10% of American adults have chronic insomnia disorder (Heffron, 2014). Insomnia can have many concerning consequences. Heffron (2014) reported that chronic insomnia can increase the risk of developing heart disease or depression. In U.S. service members returning from deployment, insomnia was found to be the most commonly reported symptom on the PTSD Checklist and predicted other symptoms of posttraumatic stress disorder (McLay et al., 2010). American workers with insomnia lose roughly 8 performance days annually, which accounts for $63 million in lost performance (Heffron, 2014).
CTS is related to poor sleep. Pereira et al. (2016) studied 42 patients with CTS and found that greater CTS severity was associated with increased sleep fragmentation and oxygen desaturation. Patel et al. (2014), who investigated the effect of CTS on sleep quality in 66 patients with CTS, reported a correlation between sleep disturbances and CTS. A study by Lehtinen et al. (1996) with 34 participants revealed that those with CTS often experienced fragmented sleep. These studies provide an initial foundation for understanding the relationship between CTS and sleep.
In occupational therapy, there has been renewed interest in the study of sleep. Adolf Meyer (1922), a psychiatrist who influenced the occupational therapy profession, emphasized sleep as an essential part of a healthy and balanced life. However, between Meyer’s time and 2001, in keeping with cultural views of sleep as a form of unconsciousness, the profession did not consider sleep to be an occupation. Renewed interest in sleep as an occupation was rooted in the multidisciplinary theoretical explorations commonly undertaken in the early days of occupational science. From this perspective, Pierce (2001) asserted that “an understanding of the restorative dimension of occupation must be based in an appreciation of the basic, life-giving occupation of sleep” (p. 253). Pierce and Summers (2019) persisted in stressing sleep as an occupation and a requirement for health, recently stating, “Sleep disorders are disruptions to the largest and most health-impacting occupational pattern in human life” (p. 737).
Both the second and third editions of the Occupational Therapy Practice Framework: Domain and Process (American Occupational Therapy Association [AOTA], 2008, 2014) included rest and sleep as an occupation. The third edition defined rest and sleep as the “activities related to obtaining restorative rest and sleep to support healthy, active engagement in other occupations” (AOTA, 2014, p. S20). A chapter on sleep and rest was included in Willard and Spackman’s Occupational Therapy (12th ed.; Solet, 2014), but only one comprehensive text on sleep and sleep problems has been published for occupational therapy practitioners (Green & Brown, 2015).
In a scoping review, Leland et al. (2014) examined sleep interventions that could be considered within the domain of occupational therapy practice for older adults. They found that effective occupational therapy treatment methods for older adults involve the encouragement of evening routines that render favorable sleep behaviors, the enhancement of a sleep-conducive environment, and the adaptation of daily routines. Later, Leland et al. (2016) studied the association between the discontinuation of napping, an occupation-based intervention, and enhanced sleep in older adults. They found that those who received an occupation-based intervention had an overall net gain in nighttime sleep, demonstrating that the elimination of daytime napping and engagement in daytime activity improve nighttime sleep.
A recent feasibility study on restoring effective sleep tranquility through occupational therapist–conducted cognitive–behavioral therapy for military veterans with insomnia found that this approach may reduce veterans’ sleep difficulties and improve their participation (Eakman et al., 2017). The authors also cited the need for a future controlled trial. Foitzik and Brown (2017) found an important relationship between sleep occupations and sensory processing abilities in children. Because sleep is an occupational need, occupational therapy practitioners should implement routine assessment and treatment of sleep to improve their clients’ quality of life. In addition, occupational therapy practitioners should call for future research that prioritizes sleep (Tester & Foss, 2017).
Despite occupational therapy practice’s rich history in the assessment and treatment of people with CTS from a functional standpoint and its expansion of the study of sleep, no research has connected occupational therapy with sleep quality’s role in hand function, CTS severity level, and CTS pain level in people with CTS. Accordingly, this study used a cross-sectional design to investigate the relationship of sleep quality and hand function in clients with CTS. We hypothesized that sleep quality is positively associated with hand function above and beyond the association of pain and CTS severity with hand function in clients with CTS.
Method
Participants
Participants included 53 treatment-seeking adults who were diagnosed with CTS using electromyography (EMG). Inclusion criteria included being age 18 yr or older and the ability to understand and respond in English. There were 17 male participants and 36 female participants, ranging in age from 30 to 86 yr (mean [M] = 58.42, standard deviation [SD] = 14.74). Although there were fewer participants with mild CTS (n = 12; 22.6%) than moderate (n = 20; 37.7%) or severe (n = 21; 39.6%) CTS, this difference was not significant, χ2(2) = 2.755, p = .252.
Participants were recruited between August and November 2015 through convenience sampling. Institutional review board approval was attained through a major university. Participants included adults who were physician referred for EMG testing at an orthopedic practice in the southwestern United States. Informed consent from each participant was obtained before participation.
Measures
The Manual Ability Measure–20 (MAM–20; Chen, 2011), an occupational therapy assessment, was used to assess hand function. It consists of 20 items rated on a scale of 1–4, indicating clients’ difficulty completing everyday hand tasks, and has been found to be responsive to changes in hand function for clients receiving occupational therapy.
The Pittsburgh Sleep Quality Index (PSQI; Buysse et al., 1989) is a 19-item measure in which participants retrospectively report their sleep quantity and quality for the past month. Participants score their sleep in seven areas: sleep latency, subjective quality of sleep, habitual sleep efficiency, sleep duration, sleep disturbance, use of sleeping medication, and daytime dysfunction. The PSQI’s test–retest reliability and validity are high (Backhaus et al., 2002). Participants were asked to indicate their hand pain level using a visual analog scale (VAS) ranging from 0 (no pain) to 10 (worst pain).
A nerve conduction test and EMG were used to detect CTS and CTS severity. The nerve conduction test quantifies the speed at which impulses move along the median nerve, with delayed conduction velocity reflecting poor nerve function. EMG evaluates denervation (nerve blockage) in the muscle innervated by the median nerve (Weiss, 2013). In mild CTS, the sensory latency 14 cm across the wrist is greater than 3.7 ms; in moderate CTS, the sensory latency 14 cm across the wrist is greater than 3.7 ms, and the motor latency 8 cm across the wrist is greater than 4.2 ms; and in severe CTS, the sensory response, motor response, or both are absent, or denervation is present on EMG (Weiss, 2013).
Data Collection
The data collection procedure included the following seven steps:
EMG testing on patients was conducted by a physician.
Potential participants were identified by EMG findings as having a positive CTS diagnosis.
The physician verbally asked the potential participants for permission to include them in the study.
After they gave verbal permission, potential participants were given a written cover letter explaining the reason for the study and an informed consent form.
Participants completed the informed consent form (which communicated that they could withdraw from the study at any time).
Participants completed the MAM–20, PSQI, and VAS (to ensure confidentiality, no participant names were used).
Data were collected and stored in a secure and locked file to protect confidentiality.
Data Analysis
Descriptive statistics for all continuous variables included means, standard deviations, and ranges. Descriptive statistics for categorical variables included frequencies, percentages, and χ2 tests. Independent-samples t tests were used to assess gender differences on sleep and CTS measures. Pearson correlations were used to assess the association between measures. Hierarchical multiple regression was used to test the association between measures after controlling for the influence of other variables. IBM SPSS Statistics (Version 23; IBM Corp., Armonk, NY) was used for data analysis.
Results
The mean Rasch-derived manual ability was 62.76 (SD = 12.11). The mean pain level as assessed by VAS was 5.96 (SD = 2.1). When present, EMG sensory latencies were a mean of 4.33 ms (SD = 0.69) and EMG motor latencies were a mean of 5.88 ms (SD = 1.69). The mean PSQI score of 10.15 (SD = 4.53) was above the cutoff score of 5 for detecting disturbed sleep. Participants reported an average of just under 6 hr of sleep per night in the past month (M = 5.94, SD = 1.53).
Male participants had higher CTS severity (M = 2.50, SD = 0.63) than female participants (M = 2.03, SD = 0.80), t(51) = 2.10, p = .041. Male and female participants did not significantly differ regarding sleep disturbance, manual ability, pain, EMG sensory latency, or EMG motor latency.
Sleep quality as assessed by the PSQI was significantly negatively correlated with manual ability; therefore, greater scores on the PSQI were associated with lower manual ability, r(53) = −.47, p = .001. Sleep disturbance as assessed by the PSQI was significantly positively correlated with pain; therefore, higher scores on the PSQI were associated with greater pain, r(53) = .364, p = .007.
There was a medium, though nonsignificant, correlation between sensory EMG latency and pain, r(33) = .306, p = .073. Neither EMG sensory latency nor EMG motor latency was significantly correlated with sleep disturbance, manual ability, or pain (all ps > .300).
Both sleep disturbance and sleep quantity were negatively correlated with manual ability; therefore, more disturbed sleep and shorter sleep duration were associated with lower manual ability (rs = −.354 and −.276, ps = .009 and .045, respectively). Both sleep disturbance and sleep quantity were positively correlated with pain; therefore, more disturbed sleep and shorter sleep duration were associated with greater pain (rs = .378 and .278, ps = .005 and .044, respectively). Neither sleep disturbance nor sleep duration was associated with CTS severity or EMG sensory or motor latency (p > .10).
In a multiple regression analysis, sleep disturbance was significantly associated with manual ability after controlling for sleep duration. After controlling for sleep disturbance, however, sleep duration was not significantly associated with manual ability (Table 1).
Multiple Regression Analyses of the Association Between Sleep Disturbance and Duration and Manual Ability
Note. Overall model: F(2, 50) = 4.66, p = .014, R 2 = .396. — = not applicable.
Sleep disturbance was significantly associated with pain after controlling for sleep duration. After controlling for sleep disturbance, however, sleep duration was not significantly associated with pain (Table 2).
Multiple Regression Analyses of the Association Between Sleep Disturbance and Duration and Pain
Note. Overall model: F(2, 50) = 5.232, p = .009, R 2 = .416. — = not applicable.
Sleep quality was significantly associated with manual ability after controlling for CTS severity and pain. Scores on the PSQI accounted for a unique 12.7% of the variance in manual ability. Table 3 provides regression statistics and parameter estimates. Figure 1 shows the association between greater sleep disturbance, as measured by the PSQI, and worse manual ability, as measured by the MAM–20.
Multiple Regression Analysis of the Association Between Sleep Quality and Manual Ability After Controlling for Carpal Tunnel Syndrome Severity and Pain
Note. Overall model: F(3, 49) = 5.387, p = .003, R 2 = .498. — = not applicable; PSQI = Pittsburgh Sleep Quality Index.
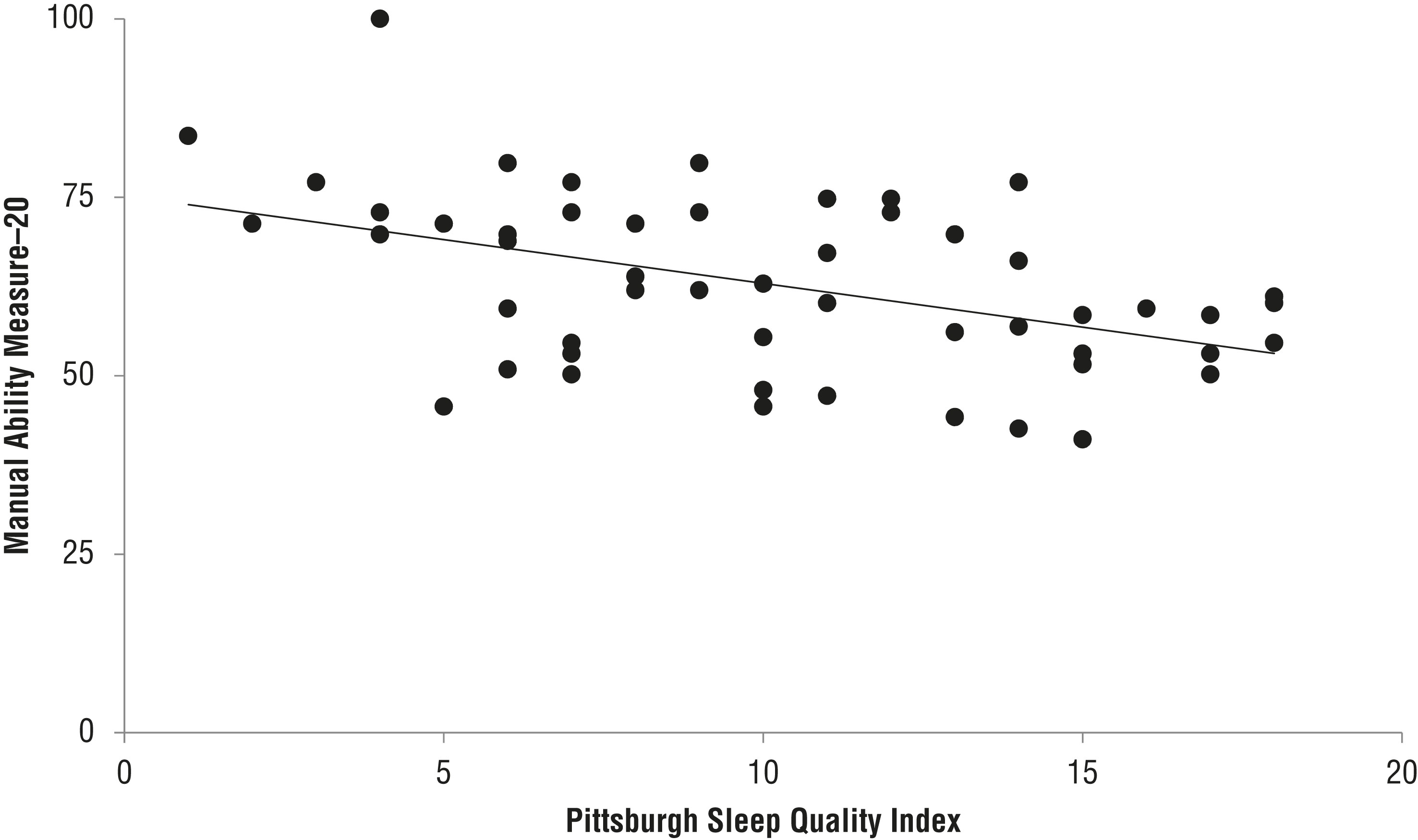
Association between sleep disturbance (Pittsburgh Sleep Quality Index) and manual ability (Manual Ability Measure–20).
Discussion
In this study, we found that greater sleep disturbance was associated with lower hand function in a group of treatment-seeking clients with CTS. This association remained even after controlling for both pain and CTS severity. Study participants also reported higher pain levels when sleep disturbance was higher. Although sleep disturbance and shorter sleep duration were both associated with lower hand function and higher pain, this relationship was stronger for sleep disturbance than for duration. A vicious cycle may exist in which CTS-related symptoms, including pain, may worsen sleep quality, or it may be that each worsens the other.
Occupational therapy practitioners should consider that careful assessment and differential diagnosis are necessary to inform interventions to improve sleep. Sleep disturbance, in general and as measured by the PSQI, can have several different causes, including insomnia, obstructive sleep apnea, and circadian rhythm disorders. Sleep disturbance is also often comorbid with pain (Morin et al., 1998).
Insomnia is no longer considered to be secondary to other disorders, such as pain, which is reflected in recent changes to diagnostic nosologies, including the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; American Psychiatric Association, 2013). Instead, research has shown that insomnia has an independent course that merits focused treatment (Harvey, 2001; Stepanski & Rybarczyk, 2006). Therefore, clients who present with sleep disturbance should be referred for evaluation and treatment of sleep disorders. Clients with CTS and disturbed sleep would also benefit from occupational therapy interventions such as assistance in adjusting sleeping position to decrease compression of the median nerve. In addition, an occupational profile can be used to determine whether sleep disturbance influences other areas of occupation.
Limitations
The use of convenience sampling at one point is a limitation of this study. However, external validity is good because all participants were treatment seeking and diagnoses were confirmed by EMG.
Future Research
Future research should include prospective or objective measures of sleep or both, including sleep diaries, actigraphy, or polysomnography, as well as objective measures of hand strength with a hand dynamometer. Another way to further this study would be to look at prospective data through sleep diaries. In addition, in this study, male participants had higher CTS severity than female participants, and Mondelli et al. (2005) reported that distal motor latency of the median nerve was more delayed in men than women in a nonsurgical sample. Future research could include investigating why this phenomenon exists.
Implications for Occupational Therapy Practice
The findings of this study have the following implications for occupational therapy practice:
Because a significant correlation existed between sleep quality and hand function in study participants after controlling for both pain and CTS severity, occupational therapy practitioners should consider baseline evaluation of sleep quality in clients with CTS, the multiple possible causes of sleep disturbance, and referral for further assessment and treatment when indicated.
Because participants with CTS were more likely to have a higher pain level when sleep disturbance was higher, practitioners should consider incorporating treatment approaches for clients with CTS that go beyond typical hand-specific rehabilitation, such as proper bed positioning, sleep preparation routines, and proactive pain control.
Designing effective CTS interventions should include sleep promotion instruction because even brief educational instruction can improve sleep outcomes (Wong et al., 2014).
Conclusion
In a sample of treatment-seeking patients with CTS, sleep quality was associated with hand function even when controlling for pain level and CTS severity level. This finding suggests that sleep may have a unique role in explaining the hand function of clients with CTS.
Findings from this study support public health and workplace initiatives that include the promotion of sleep quality for people with CTS. Occupational science was informed by this study through its investigation of the occupation of sleep, which revealed its strong link to hand function and pain in participants with CTS. Finally, occupational therapy practice was informed by the findings of this study: Because of the strong link between sleep and hand function, practitioners should ensure that CTS care includes evaluation of sleep and treatment of sleep problems.