
Abstract
Older adults are at risk of developing disability during and after cancer treatment (Deimling et al., 2007). Disability is the degree to which a person feels limited in and reduces the frequency of activity engagement because of a health condition (Jette et al., 2002). Disability is related to lower quality of life (Pergolotti et al., 2017) and can influence adherence to cancer treatment and even survival (Wildes et al., 2013).
Impairment-driven cancer rehabilitation (Silver et al., 2013) attempts to remediate the impairments that are hypothesized to contribute to disability (e.g., weakness, fatigue). However, few studies have measured whether this bottom-up approach (Trombly, 1993) of impairment reduction fully translates into reduced disability in cancer survivors. Adjusting activities and environments may also be required for optimal functioning (Nagi, 1991).
A top-down approach (Trombly, 1993) in which activity engagement is used to directly target disability is conceptually appealing in oncology. Cancer survivors often have little energy for or access to rehabilitation (Stubblefield, 2017) and, therefore, may be interested in an intervention that directly addresses the activities that they want and need to do. Such an approach lends itself to an in-home intervention where activities can be practiced in their natural environments.
Researchers who have studied in-home interventions have described the importance of feasibility testing to prepare for full-scale clinical trials (Pilegaard et al., 2018). The primary aim of this study was to explore the feasibility of both an in-home intervention for older adult cancer survivors and the study procedures that would be needed in subsequent efficacy testing. The exploratory aim was to determine whether there was a signal of efficacy within the data suggesting that the intervention increases activity engagement, decreases disability, and increases quality of life.
Method
Design
This Phase 1 pilot study used a single-blind (data collector) randomized controlled trial (RCT) design. Participants were randomized to receive either the 6-wk intervention or usual care. Study procedures were approved by the Committee for the Protection of Human Subjects at Dartmouth College (Hanover, NH).
Participants
Eligibility Criteria.
The inclusion criteria were (1) age ≥65 yr, (2) experiencing disability (i.e., a score of ≥3 on the Vulnerable Elders Survey [Saliba et al., 2001] or an answer of “yes” to the question “Do health problems interfere with your ability to carry out your social or day-to-day activities?” [Deimling et al., 2007]), and (3) either (a) diagnosed with any solid or hematological cancer and undergoing treatment of curative intent or having completed therapy within 6 mo with an absence of disease recurrence or (b) diagnosed with metastatic breast cancer or chronic hematologic malignancies with a life expectancy of ≥2 yr. Patients were excluded in the presence of (1) moderate or worse cognitive impairment as indicated by a score of ≤3 on the Callahan six-item cognitive screening tool (Callahan et al., 2002) or (2) medical record documentation of severe mental illness (i.e., schizophrenia, bipolar disorder), active suicidal ideation, or active substance use disorder.
Sample Size.
Consistent with the intent of a pilot study (Kraemer et al., 2006), the primary aim was to evaluate the feasibility of the intervention and the study procedures. There are no definitive guidelines for determining the sample size of a pilot study. A review article of 79 pilot or feasibility studies reported a median number of 30 participants per study arm (Billingham et al., 2013). In line with those conventions, we planned to enroll 60 participants.
Recruitment.
A research assistant (RA) reviewed the clinicians’ schedules for patients who were eligible regarding age and diagnosis. The clinicians introduced the RA, who explained the study and completed the disability and cognitive screening, proceeding with informed consent procedures for eligible and interested patients.
Randomization
Participants were randomized to the intervention versus usual care using a computer-generated scheme (1:1 randomization, blocked within strata with block lengths of 2 and 4 varied randomly). Randomization was stratified according to site (Norris Cotton Cancer Center versus Veterans Affairs Medical Center) and disease stage (nonmetastatic versus metastatic disease). Group assignment was conveyed to participants by the interventionist. Participants were instructed to not mention the group assignment to the project RA.
Intervention
Health Through Activity Intervention.
The Health Through Activity (HTA) intervention has been described elsewhere (Lyons, Newman, Adachi-Mejia, et al., 2018; Lyons, Newman, Kaufman, et al., 2018). Briefly, it borrows principles from a behavioral therapy that uses activity scheduling to help people increase their engagement in activities that contribute to life satisfaction (Lejuez et al., 2011). If needed, the weekly activity scheduling structure was augmented by education (on topics of activity adaptation, exercise, energy management, and sleep), environmental adaptation (e.g., rearranging furniture), provision of adaptive equipment (e.g., magnifier), and practice with the interventionist (Table 1).
Activity Scheduling Steps Used in Each Health Through Activity Intervention Session
Note. — = not applicable.
Usual Care.
Participants assigned to usual care were encouraged (during the randomization notification telephone call) to engage in any activities that they believed would increase their health and well-being. Usual-care participants were offered the opportunity to engage in the HTA program upon completion of the study.
Data Collection
Feasibility.
The RA and the interventionists documented adherence to study and intervention procedures. The RA tracked the number of patients identified, approached, screened, enrolled, and withdrawn. The interventionists recorded number, length, date, and location of sessions as well as adverse events. After the second assessment, the RA recorded her “guess” regarding treatment condition to assess the degree to which the single blind was maintained.
Potential Efficacy.
The RA orally administered the outcome assessments by telephone and entered the data in real time into a custom-designed database. Outcome assessments were administered upon enrollment and at 8 and 16 wk after enrollment.
Disability.
The Late-Life Function and Disability Instrument (LLFDI; Haley et al., 2002; Jette et al., 2002) was developed for use in community-dwelling older adults. The 16-item Disability subscale measures the frequency with which major life activities are performed and the degree of limitation experienced when doing each activity. Higher scores indicate less disability.
Quality of Life.
The Functional Assessment of Cancer Therapy–General (FACT–G; Cella et al., 1993) provides a total score as well as four subscale scores for quality of life: Physical, Social/Family, Emotional, and Functional Well-Being. Evidence supports the psychometrics of the FACT–G with older adults with cancer (Overcash et al., 2001). Higher scores indicate better quality of life.
Activity Level and Satisfaction.
The Activity Card Sort (ACS; Baum & Edwards, 2008) was developed to measure the instrumental, leisure, and social activity levels of older adults. A modified version for use with cancer survivors (ACSm; Lyons et al., 2010) was used in this study. The following response choices and values were used to create ratio scores: I do not do and do not want to do (0 points in both the denominator and numerator); I do this now and am satisfied (1 point in both the denominator and numerator); I do this now but am not satisfied (e.g., it’s hard, boring, scary, infrequent) (1 point in the denominator and 0.5 points in the numerator); and I do not do this regularly, but I want to do this (1 point in the denominator and 0 points in the numerator). Higher ratio scores indicate greater satisfaction with activity level.
Behavioral Activation.
The Behavioral Activation for Depression Scale (BADS; Kanter et al., 2007) measures self-reported avoidance behavior and activated behavior. The BADS Activation subscale contains seven items that directly reflect the goals of the HTA program (e.g., “I am content with the amount and types of things I did,” “I engaged in a wide and diverse array of activities,” “I was an active person and accomplished the goals I set out to do”). Higher scores indicate greater activation.
Data Analysis
Recruitment, retention, and intervention data were summarized with descriptive statistics. Baseline characteristics and scores were summarized with descriptive statistics, and the two groups were compared with Fisher’s exact test to explore the degree to which the randomization process worked to effectively create balanced groups. The Clopper–Pearson (1934) exact method was used to assess the degree to which the RA remained blinded to group assignment using her guess for group assignment at the 8-wk assessment.
To explore potential efficacy, we conducted linear mixed models to identify changes over time. In addition to using group (HTA vs. usual care) as a factor, we used stage (metastatic vs. nonmetastatic disease) as a factor because people with metastatic disease could experience worsening disability over time whereas people with curative disease could naturally experience reductions in disability as they recover from treatment. Linear mixed models were calculated using a compound symmetry covariance structure examining fixed effects of group, stage, Group × Stage, time, Group × Time, Stage × Time, and Group × Stage × Time.
In a post hoc analysis, we wanted to see whether we could detect change in items that were specifically addressed by participants in the HTA group. Two of the 16 LLFDI items (“taking part in a regular fitness program” and “taking care of the inside of your home”) were addressed by most participants in the HTA group and accounted for the majority of goals set. For example, 88% of the HTA group set at least one goal for engaging in aerobic exercise and 46% set at least one goal regarding home management. Exercise and home management activities were the target of 84% of the weekly goals set during HTA sessions. Therefore, we created a new variable using only those two items from the LLFDI and reran the linear mixed-modeling process on the new variable.
Results
Participants
Recruitment and retention data are presented in Figure 1. Forty-four percent of patients approached reported no disability, and 30% declined to either enroll or be formally screened for the study. Most who declined reported no interest in rehabilitation because they were doing “as well as could be expected.” One person declined because of disinterest in an in-home intervention. Sixty-one participants enrolled in the RCT. Two participants were subsequently found to be ineligible and were removed from the study. Fifty-nine participants were randomized.
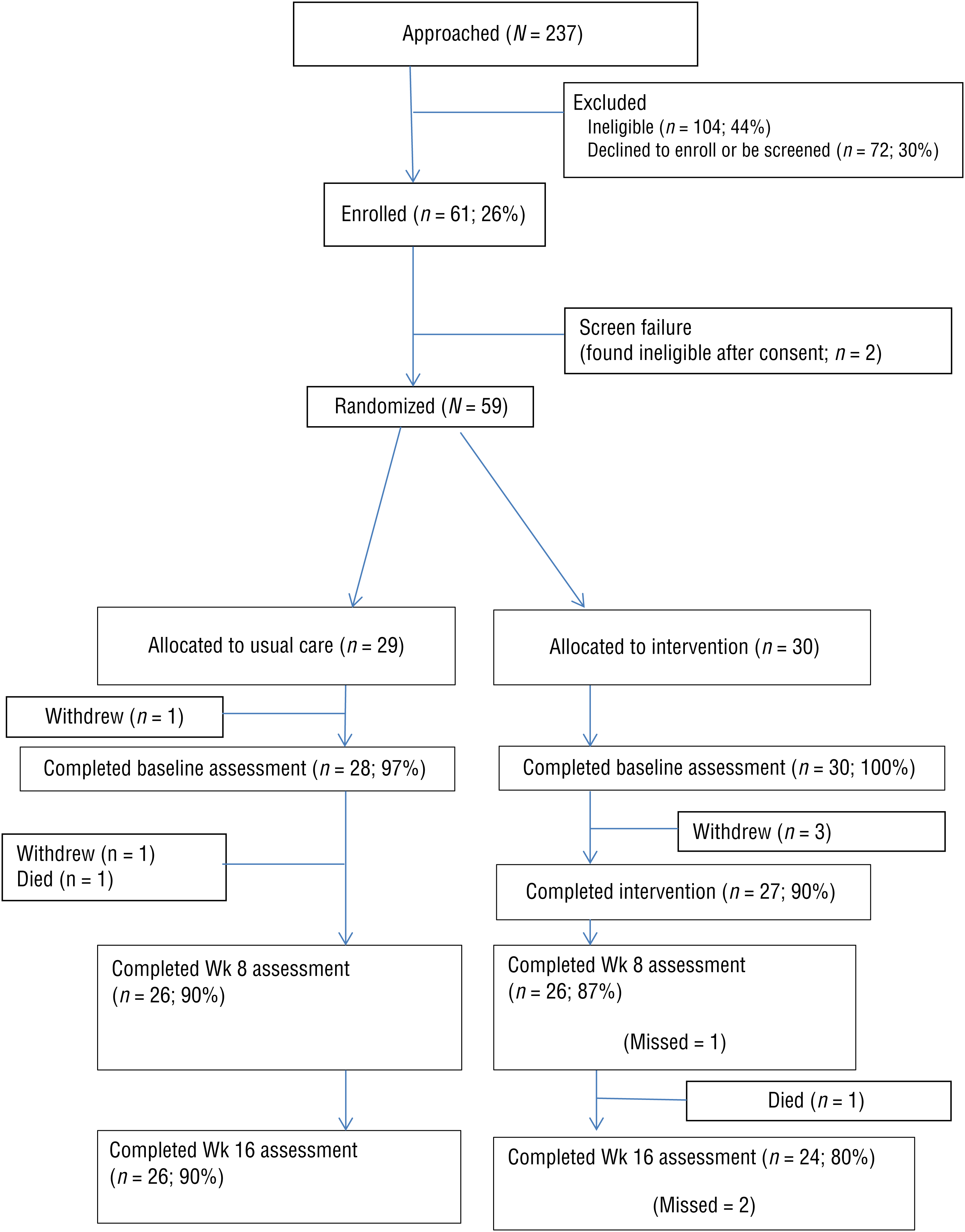
CONSORT (Consolidated Standards of Reporting Trials) flow diagram for study participants.
Participant characteristics are presented in Table 2. The sample was predominantly female (64%), married (54%), and highly educated (75% had some college experience). The sample’s racial and ethnic composition was primarily White (97%) and non-Hispanic (100%). The most common diagnoses were hematological cancers (56%) and breast cancer (31%). Thirty had metastatic disease (51%), and 29 had nonmetastatic disease (49%). There were no significant differences in baseline scores or characteristics between groups.
Phase 2 Participant Characteristics (N = 59)
Note. GED = General Education Development; — = not applicable.
Fisher’s exact test.
Feasibility
Randomized Controlled Trial Study Procedures.
After recruitment, all participants accepted randomization. Upon completion of the study, 3 participants in the usual-care group chose to meet with the interventionist to review the HTA program materials (1 wanted to pursue a goal and use the intervention to attain a piece of equipment; the others expressed interest in and appreciation of the workbook materials but did not wish to pursue structured activity scheduling). Six participants broke the blind when conversing with the RA. There was a trend suggesting that the RA guessed the group assignment with slightly more accuracy than would be expected by chance alone (64% accuracy, 95% confidence interval [48%, 78%], two-sided p = .07). The RA reported that she had a sense of when the interventionist was doing home visits based on time away from the office, and that information influenced her guesses.
Two participants withdrew from the usual-care group and 3 participants withdrew from the intervention group for an overall withdrawal rate of 8%. Two participants reported feeling too ill to participate (1 from the HTA group, 1 from usual care), 2 reported lack of interest in or need for the intervention (HTA group), and 1 thought the assessments were too long (usual care). Ninety percent of usual-care participants completed all study outcome assessments, and 80% of intervention participants completed all study outcome assessments.
Intervention Procedures.
Ninety percent of participants randomized to the intervention group completed the intervention’s six sessions. Of the 27 program completers, 15 (56%) completed the program within 7 wk of being randomized, 9 (33%) more completed the program within 8 wk of being randomized, and 3 (11%) took more than 8 wk to complete the program. Reasons for postponing a session included illness (from cancer treatment or another reason), inclement weather (with a preference to reschedule as opposed to talk via telephone), vacation (of interventionist or participant), and death in the family. On average, the sessions were 56 min long (standard deviation [SD] = 22 min, range = 5–135 min). The first session was only slightly longer (mean [M] = 64 min, SD = 13) than the subsequent five sessions (M = 55 min, SD = 23). As planned, most sessions occurred in the participants’ homes (n = 147, 89%), with fewer occurring by phone (n = 13, 8%), as a result of inclement weather or patient or therapist illness, or at the cancer center (n = 5, 3%).
Two adverse events occurred during the study. One man chose to practice floor-to-stand transfers in preparation for returning to kayaking. He first transferred safely in front of the interventionist and between sessions successfully completed the transfer on many days, but on 1 day, he experienced back pain after performing the transfer. He did not practice the transfer for 2 days, and the pain resolved on the third day. One woman fell while walking with a friend. She had taken a walk with the interventionist and did not display any challenges in balance or gait. When walking with her friend, she reported feeling a “burst of energy” and an inability to stop herself from rapidly moving and falling forward. A subsequent medical workup did not reveal any cancer progression or explanation for the fall. She did not sustain permanent injury from the fall but did chip a tooth, which was subsequently repaired. She walked with the interventionist during subsequent sessions and reported that her children urged her to not stop walking.
Potential Efficacy
The estimated marginal means from the linear mixed models are presented in Table 3. Regarding the primary outcome of interest, there was a main effect of time on the frequency component of the LLFDI Disability subscale, F(2, 94) = 3.7, p = .03, with both groups reporting small increases over the study. Although there were no significant main effects or interactions, the limitation component of the LLFDI Disability subscale stayed essentially flat in the usual-care group, with small improvements seen in the HTA group.
Linear Mixed Models to Explore Changes in Outcomes Over Time
Note. ACSm = Activity Card Sort modified; BADS = Behavioral Activation for Depression Scale; FACT–G = Functional Assessment of Cancer Therapy–General; HTA = Health Through Activity Intervention; LLFDI = Late-Life Function and Disability Instrument; SE = standard error; UC = usual care. LLFDI 2 includes only the exercise and the home management items from the Late-Life Function and Disability Instrument.
When the exercise and home management items from the LLFDI Disability subscale frequency component were examined in the post hoc analysis, there was a main effect of time, F(2, 93) = 3.4, p = .04; a Group × Time interaction, F(2, 93) = 3.5, p = .03; and a trend toward Group × Stage × Time interaction, F(2, 93) = 2.7, p = .07. Upon inspection, HTA participants (both with and without metastatic disease) showed increased frequency in exercise and home management activities. Participants without metastatic disease in the usual-care group showed no change on these items, and those with metastatic disease reduced frequency over time. There was a main effect of time for the two-item limitation variable, F(2, 95) = 3.1, p = .05. The usual-care group showed small improvements, whereas the HTA group reported larger improvements during the intervention period, although the interaction between group and time was not significant, F(2, 95) = 2.2, p = .11.
Regarding quality of life, there was a main effect of time, with both groups reporting steady improvement, F(2, 93) = 5.8, p = .004. The usual-care group reported an increase of 4 points over the course of the study, and the HTA group reported a change of 6.4 points on the FACT–G over the course of the study, indicating a clinically meaningful improvement only in the HTA group (Cella et al., 2002). There was a main effect of stage that approached significance, F(1, 51) = 3.9, p = .053, with participants with metastatic disease reporting slightly higher FACT–G scores than those without metastatic disease.
Regarding satisfaction with activity level, the ACSm scores for the HTA group rose steadily. At baseline, participants were satisfied with their engagement in 67% of their usual activities. After intervention, satisfaction increased to 70%, and 8 wk later, satisfaction increased to 76%. The satisfaction among participants in the usual-care group was more variable, with 72% at baseline, 76% at the second assessment, and then dropping to 73% 8 wk later. However, there were no significant main effects or interactions within the linear mixed models.
Regarding behavioral activation, there was a main effect of time for activation, F(2, 95) = 9.4, p < .0001, indicating improvement in both groups over time. There was also a significant interaction among group, stage, and time, F(2, 95) = 3.3, p = .04. The two curative groups showed similar increases in activation during the first 8 wk of the study, whereas the metastatic groups showed a different pattern. The participants with metastatic disease in the usual-care group showed a slight dip in activation during the first 8 wk of the study, whereas the participants with metastatic disease in the HTA program showed an increase in activation.
Discussion
The primary aim of this study was to assess the feasibility of the HTA and the study procedures that would be needed in a larger scale trial of efficacy. Once enrolled in the RCT, participants had a high retention rate, with a withdrawal rate of 8%. However, identifying and screening potential participants was labor intensive because 44% of patients approached reported no disability and 30% declined to either enroll or be formally screened for the study. These recruitment rates mirror those reported by Cheville, Rhudy, et al. (2017), who found that only one-third of patients with advanced cancer were receptive to rehabilitation services.
Intervention participants were highly receptive to the in-home program, with 89% of the sessions occurring within the home as designed. The intervention procedures appear acceptable and feasible, with 89% of the participants completing the intervention within the first 8 wk of the study. Two participants experienced an adverse event while engaging in an activity on their own between sessions. Both participants had practiced the activity with the interventionist before attempting it, and neither had experienced discomfort or exhibited unsafe behavior. The in-home intervention was designed to minimize risk by having the opportunity to practice with a therapist. Acknowledging both the risks and the benefits of exercise, both participants reported that continued participation in the activities was important to them, and they subsequently engaged in the activities without incident.
There is a signal suggesting the potential efficacy of the HTA program. The HTA group displayed steady improvement in both the frequency and limitation components of the LLFDI Disability subscale, but the gains were small in magnitude. This result is not completely surprising because the dose of the intervention was low compared with other efficacious interventions that follow older adults for months (e.g., Bakitas et al., 2009; Clark et al., 1997). Regarding the items that most participants chose to address within the intervention, the Group × Time interaction indicates that the HTA group had significantly higher frequency of engagement in exercise and home management activities. This result mirrors the results of a content analysis of HTA sessions that found significant improvement in activity engagement and confidence in the ability to perform personally chosen valued activities (Lyons, Newman, Kaufman, et al., 2018).
Taken together, the results suggest that the HTA program helped participants increase engagement in personally chosen activities, although it did not translate into substantial decreases in disability. However, the continued improvement beyond the end of the HTA program suggests that participants continued to build activity level and it might take more time for those effects to be seen. There is evidence to suggest that reductions in participation restrictions or disability take up to 6 mo to be seen (Hammel, 2016).
The data suggest that the HTA program may be most helpful for people with metastatic disease. Participants with metastatic disease who participated in the HTA program showed increases in activation and in exercise and home management frequency, whereas people with metastatic disease assigned to usual care showed declines in both sets of scores over time. This finding suggests that the HTA program may be useful in helping people with metastatic disease adopt active lifestyles and behaviors that could slow the functional decline that is predicted with advanced cancer. New research is articulating the promise of palliative rehabilitation (Cheville, Morrow, et al., 2017; Nottelmann et al., 2017), and these results encourage future exploration.
Going forward, two adjustments may be warranted. It is possible that individualized outcome assessments (Donnelly & Carswell, 2002) may be more appropriate (and sensitive) for a patient-directed intervention such as the HTA, in which participants can choose where to focus their energies. In addition, the potency of the intervention may need to be enhanced by lengthening the intervention or supplementing it with other modalities such as virtual or social support.
The following limitations of the study should be considered when interpreting the results. First, the study was powered for feasibility testing, not for the analyses of potential efficacy. The provisional efficacy analyses also include a post hoc analysis that was not prespecified when designing the study. Second, the study sample was not blind to group assignment and was mostly composed of highly educated, White women.
Implications for Occupational Therapy Practice
This study has the following implications for occupational therapy practice:
The HTA intervention is client directed, nonprescriptive, and occupation based, reflecting core tenets of occupational therapy.
This study offers evidence of the feasibility and potential efficacy of directly addressing activity engagement in cancer rehabilitation, which appears to be most helpful for people with metastatic disease, as opposed to focusing exclusively on impairment reduction.
Practitioners interested in using this intervention before definitive efficacy testing is completed should monitor goal attainment to ensure that the intervention is supporting participants’ needs.
Conclusion
The study results suggest that a home-based occupational therapy intervention for older adults is feasible to implement and acceptable to participants. There were encouraging indications that the HTA program helped participants increase their activity level, specifically in exercise and home management activities, and particularly for those with metastatic cancer, although improvements were less evident for reductions in disability. Further research is warranted, particularly within the subpopulation of people living with metastatic cancer.