
Abstract
Visual impairments are common after traumatic brain injury (TBI). Studies estimate that as many as 90% of people with TBI experience injury-related vision impairments (Ciuffreda et al., 2007), of which 56%–80% are oculomotor (Ciuffreda et al., 2007; Schlageter et al., 1993). The oculomotor system has representation in all brain lobes, making eye movements easily impaired as a result of TBI (Baker & Epstein, 1991; Helvie, 2011; Leigh & Zee, 2006). Eye movements include pursuits, saccades, vestibular ocular reflex, convergence, and fixations (Leigh & Zee, 2006). Oculomotor impairments can negatively affect activities of daily living such as reading, computing, and community participation (Ciuffreda et al., 2007; Kapoor & Ciuffreda, 2002; Warren, 1993a).
Evaluation and treatment of oculomotor impairments are key to improving functional vision in TBI rehabilitation (Warren, 1993a, 1993b). Both remedial protocols and compensatory interventions can be used (Powell & Torgerson, 2011; Warren 1993a, 1993b). Little evidence exists to assist clinicians with a reliable remedial protocol for impaired oculomotor skills in this population. Published literature on vision rehabilitation after TBI primarily provides Level II and III evidence, is typically older than 5 yr, and frequently involves people with mild TBI or stroke (Berger et al., 2016; Kapoor & Ciuffreda, 2002; Riggs et al., 2007).
The two protocols used in this study reflect a remedial approach to oculomotor treatment (Powell & Torgerson, 2011; Warren, 1993b). The Six Eye Exercises (SEE) protocol is informed by exercises in the literature that emphasize direct eye movement practice (Ciuffreda & Ludlam, 2009; Kapoor & Ciuffreda, 2002). Each eye movement described by Leigh and Zee (2006) is included. The SEE protocol reflects a bottom-up approach to oculomotor treatment (Powell & Torgerson, 2011) and has been used by clinicians in the study facility with anecdotal success. The standard-of-care (SOC) control protocol emphasizes activity-based eye movement practice frequently used by occupational therapy practitioners (Powell & Torgerson, 2011; Raymond et al., 1996; Warren, 1993a, 1993b; Zoltan, 2007). Activities and occupations that integrate eye movements, such as scanning and reading, are included. The SOC protocol reflects a top-down approach to oculomotor treatment (Powell & Torgerson, 2011).
Formally comparing these two protocols could help determine whether a top-down or bottom-up approach to remedial oculomotor treatment is most effective in TBI rehabilitation. This pilot study was designed to examine the process, resources, management, and scientific validity (Thabane et al., 2010) for conducting an appropriately powered randomized controlled trial (RCT) of a direct exercise protocol for oculomotor rehabilitation after TBI.
Method
Research Design
A two-group RCT design was used. The study was approved by the HCA Healthcare HealthONE (Denver, CO) institutional review board.
Instruments
The primary outcome measure, the Craig Hospital Eye Examination Rating Scale (CHEERS), measures the severity of oculomotor impairments. It is an eye movement rating scale that examines smooth pursuit, saccades, vestibular ocular reflex, vergence, and fixation and nystagmus. Interrater reliability was reported as strong, and test–retest reliability was reported as moderate (Politzer et al., 2017). A higher CHEERS score means greater impairment.
Several secondary outcome measures were used to determine the functional impact of oculomotor impairments:
For saccadic speed and accuracy, the King–Devick Test (K–DT; Lieberman et al., 1983), a rapid number naming test that measures saccades, was used. K–DT test–retest reliability and sensitivity to changes in reading fluency and comprehension are reported as strong (Dodick et al., 2017; Heick et al., 2016). Slower speed and more errors mean greater impairment.
For scanning speed and accuracy, the Delis–Kaplan Executive Function System (D–KEFS; Delis et al., 2001) Trail Making Test: Condition 1 Visual Scanning, a number cancellation test, was used. Test–retest reliability is .56. Slower speed and more errors mean greater scanning impairment.
For reading speed and accuracy, the Nelson–Denny Reading Test (NDRT; Brown et al., 1993): Subtest 1, a reading screening instrument that measures reading rate, was used. Test–retest reliability for the NDRT reading rate is modest (Rudner, 1991). A modified version of Subtest 1 was used. Participants read the passage aloud versus silently for 1 min to enable evaluators to monitor reading errors. Fewer words read and more errors mean greater impairment.
For subjective symptoms, the Vision Symptom Scale (VSS), an 11-symptom self-report Likert scale (from 0 to 4) developed for this study to monitor subjective symptom frequency and severity, was used. It was administered immediately after the NDRT to characterize reading-induced symptoms. Psychometric properties were not established because of time frames for trial completion. A higher score means more severe symptoms.
Participants
Consecutive admissions to the inpatient TBI program at a single Colorado-based rehabilitation hospital were screened for eligibility by their primary occupational therapist within 72 hr of admission. All patients with TBI who were ages 18–65 yr were screened for eligibility. Patients were eligible if they had any impairment of visual fixation, pursuits, saccades, vestibular ocular reflex, or convergence. People with oculomotor impairment were excluded from enrollment if they had a projected inpatient stay of less than 6 wk, could not see stimuli during oculomotor screening, could not use at least one arm, could not follow a standard three-step instruction, could not sustain attention for a 30-min treatment session, or were participating in another clinical trial. After giving consent, eligible participants were enrolled in the experimental SEE group or the control SOC group by a masked statistician according to a randomization schedule. Participants were masked to group assignment.
Procedures
All participants underwent a baseline vision evaluation by a rehabilitation optometrist who was masked to group assignment. The optometrist performed the CHEERS, an acuity check, and an eye health examination on site. Compensatory lenses for acuity and double vision were prescribed as indicated. An investigator was present at all initial evaluations with the optometrist. Within 1–24 hr of the vision evaluation, participants completed a baseline functional evaluation in a quiet room with one of two occupational therapists who were uniformly trained on administering the secondary outcome measures and who were masked to group assignment. Recommended compensatory lenses from the vision evaluation were not used during baseline functional testing, because the lenses had not been made in time. Lenses worn before injury were used if available. Meetings were held with the evaluators at monthly intervals to maintain consistency with evaluation performance.
During the treatment phase, all SEE group and SOC group participants received their regular therapies, including vision interventions that fell within SOC occupational therapy as directed by their primary occupational therapist. Participants received 30 min of additional 1:1 vision treatment, according to their group assignment, 5 days per week for 4 wk. One of four nonevaluator occupational therapists, who were uniformly trained in one of the specific protocols, performed the treatment. The treating occupational therapists were masked to the protocol being used in the other treatment group. Monthly meetings were held to review protocols. Participants used recommended compensatory lenses, once obtained, for acuity and double vision during treatment sessions.
The SEE protocol included six exercises: eye stretches, tracking, gaze stabilization, spatial localization, saccades, and vergence. Eye stretches and four of the remaining five exercises were performed in each treatment session. The SOC protocol included activities that integrate oculomotor skills under four categories: visual–motor, scanning, visual cognition, and reading. At least one activity from each category and 5 min of reading were performed in each treatment session. After completing their respective 4-wk protocols, each participant was retested on all primary and secondary outcome measures according to the pretesting procedure. Participants in both groups used their corrective lenses for acuity and double vision during posttreatment testing. Participants had to complete 16 of 20 allotted therapy sessions for data to be maintained for analysis. Participants were paid $25 for each completed pre- and posttesting session.
Data Analysis
Data were analyzed descriptively as frequencies, percentages, means and standard deviations, and 95% confidence intervals.
Results
Participants
Over a 1-yr period, 138 people in acute rehabilitation with acquired brain injury were screened for eligibility. Twenty-six met all eligibility criteria (Figure 1); 6 of them declined participation. Sixteen participants (80%) completed the minimum number of treatment sessions. Four participants withdrew from the study early as a result of fatigue (3 from the SOC group and 1 from the SEE group). No other negative effects were reported in either treatment group. Two participants completed only partial posttreatment evaluations because they were discharged early from the hospital, and they were dropped from analysis. Therefore, 14 participants (70%) were retained for analysis (6 in the SOC group and 8 in the SEE group). No significant differences between the two groups were detected for age, gender, education, mechanism of injury, length of posttraumatic amnesia, or days postadmission. Demographic and clinical characteristics of the two groups are presented in Table 1.
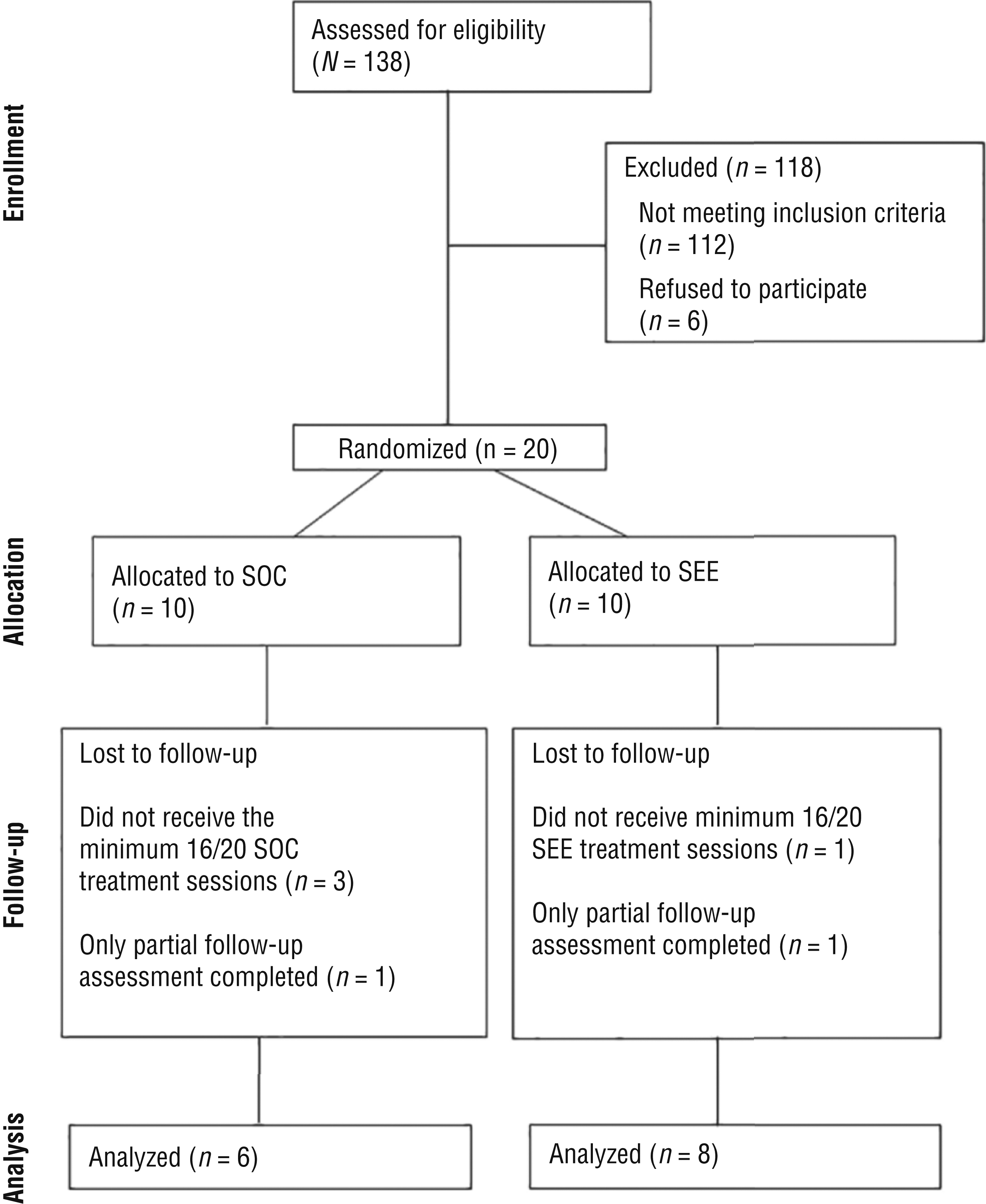
Consolidated Standards of Reporting Trials (CONSORT) flow diagram for study participants.
Participant Demographics
Note. M = mean; MVA = motor vehicle accident; SD = standard deviation; SEE = Six Eye Exercises; SOC = standard of care.
Possible sco
Possible score range, 5–35.
Primary Outcome
At baseline, the SOC group CHEERS total indicated that this group was more impaired than the SEE group (Table 2). Impairment was most frequently noted on the Smooth Pursuit subscale of CHEERS (100%). Both groups improved on CHEERS, with the SOC group exhibiting greater average change (Table 3). On the Smooth Pursuit subscale, more in the SEE group (38%) reached an unimpaired score than in the SOC group (17%).
Primary and Secondary Outcome Measure Scores
Note. CHEERS = Craig Hospital Eye Examination Rating Scale; D–KEFS = Delis–Kaplan Executive Function System; K–DT = King–Devick Test; M = mean; NDRT = Nelson–Denny Reading Test; SD = standard deviation; SEE = Six Eye Exercises; SOC = standard of care; VOR = vestibular ocular reflex; VSS = Vision Symptom Scale.
Mean Score Change From Baseline to Posttreatment
Note. CHEERS = Craig Hospital Eye Examination Rating Scale; CI = confidence interval; D–KEFS = Delis–Kaplan Executive Function System; K–DT = King-Devick Test; M = mean; NDRT = Nelson–Denny Reading Test; SD = standard deviation; SEE = Six Eye Exercises; SOC = standard of care; VSS = Vision Symptom Scale.
n = 5.
Secondary Outcomes
At baseline, 100% of the participants reported visual symptoms on the VSS. The SEE group reported a greater average number and severity of symptoms than the SOC group (Table 2). Posttreatment, the number and severity of symptoms improved in both groups, with the SEE group exhibiting a greater reduction in average number of symptoms (Table 3). Posttreatment, 38% of the SEE group was asymptomatic compared with 17% of the SOC group.
Reading rate on the NDRT was similar for both groups at baseline (Table 2). Both groups improved at posttreatment, with the SEE group exhibiting a greater average improvement in reading speed (Table 3). The SEE group was slightly slower on the D–KEFS Visual Scanning test at baseline and exhibited greater average improvement posttreatment (Table 3). The SEE group was also slightly slower on the K–DT at baseline and exhibited slightly greater average improvement posttreatment (Table 3).
Discussion
Participants in both groups improved in functional status over the course of treatment, indicating that oculomotor intervention could be helpful and is not harmful in TBI rehabilitation (Berger et al., 2016; Ciuffreda & Ludlam, 2009; Kapoor & Ciuffreda, 2002; Powell & Torgerson, 2011; Raymond et al., 1996; Riggs et al., 2007; Schlageter et al., 1993; Warren, 1993a, 1993b). Even though participants in the SEE group had more symptoms at baseline than those in the SOC group, a larger percentage of the SEE participants reported improvement and resolution of their disruptive visual symptoms during reading without extra reading practice. Further study could reveal clinical usefulness of bottom-up direct practice using the SEE protocol along with more traditional top-down activity-based practice in occupational therapy treatment of vision impairments in people with TBI (Powell & Torgerson, 2011). Process, retention, resources, procedures, and outcome measures as described by Thabane et al. (2010) were suggestive of an appropriately powered RCT.
Limitations and Future Research
The imbalance of impairment severity in the treatment groups was the primary limitation of this study. For small pilot studies, allocation by minimization to more closely match the groups on severity of injury and impairments is suggested. Another limitation involved the use of lenses for acuity and double vision. Two participants in each group needed special lenses to compensate for double vision. The lenses were not used during pretesting because they had not yet been obtained, but they were used during posttesting because the participants had used them throughout the duration of their treatment. It is difficult to determine whether these participants improved from the treatment, the lenses, or both. A plan for quickly dispensing lenses for pretesting is recommended.
The diffuse nature of TBIs and the natural healing that occurs during acute rehabilitation make it difficult to attribute improvements to treatment alone. In an appropriately powered study, we suggest using statistical analyses to determine more closely what factors can be attributed to improvements outside of treatment. More sensitive oculomotor testing for a primary outcome measure could improve objective measurement; a computerized pursuit test, for example, could reduce errors.
In the future, a third treatment group that receives 15 min of SEE treatment and 15 min of SOC treatment is recommended. This combination treatment would allow evaluation of the efficacy of using both direct bottom-up and activity-based top-down practices. A fourth group that does not receive extra treatment could be considered. Applying this methodology to an outpatient population after a period of natural healing has happened may also strengthen validity. Finally, this study design could also be used with people with concussion and mild TBI to determine efficacy of oculomotor interventions in populations with these conditions.
Implications for Occupational Therapy Practice
The results of this study have the following implications for occupational therapy practice:
Oculomotor dysfunction seems to improve during inpatient rehabilitation with targeted treatment; best practice for remedial treatment of oculomotor impairments post-TBI has not yet been established.
An RCT of this nature could positively contribute to the body of evidence for vision intervention in TBI rehabilitation.
Providing oculomotor-based treatment in TBI rehabilitation has only minimal negative effects and could be helpful for improving functional vision.
Conclusion
The results of this pilot study suggest that an appropriately powered RCT would be useful in examining the efficacy of oculomotor intervention in TBI rehabilitation, with some changes. The SEE protocol may be useful as a preparatory activity in activity-based vision treatment or as a stand-alone intervention to comprehensively treat oculomotor impairments in TBI rehabilitation.
Footnotes
Acknowledgments
We thank the Colorado Neurological Institute (CNI) for its generous grant to make this pilot study financially possible. In addition to financial support, CNI also shared its statistician, Larry Snell, who provided us clear direction, expert statistical abilities, and enthusiastic participation in this project. The authors have no individual conflicts of interest to disclose.