
Abstract
Duchenne muscular dystrophy (DMD) is an X-linked congenital disease affecting 4.8 in 100,000 men and boys (Mah et al., 2014). Spinal muscular atrophy (SMA) is a genetically heterogeneous group of inherited disorders that most often involve impairment in the survival motor neuron 1 gene and varies in incidence from 1 in 6,000 to 1 in 25,000 (Viollet & Melki, 2013). Both DMD and SMA cause progressive muscle degeneration and weakness over time, contributing to impairments in cardiorespiratory function, ambulation and mobility, and activities of daily living (ADLs; Chen et al., 2012; Johnson et al., 1992). Feeding and oral hygiene are important components of ADLs and have received limited clinical attention in this population.
Over the past 30 yr, large gains have been made to improve the length and quality of life of people with DMD and SMA, and it is now common for people to live well into their 30s (Ishikawa et al., 2011; Ricotti et al., 2015). As people with DMD and SMA live longer, novel areas of dysfunction and disability have become apparent. Over the past 20 yr, a growing body of evidence has examined the impact these diseases have on oral function as it pertains to nutrition and feeding skills. People with DMD and SMA develop progressive weakness of the muscles involved in swallowing, chewing, and speaking (Archer et al., 2013; Botteron et al., 2009; Chen et al., 2012). This weakness impairs mastication, leading to increased fatigue with meals (Chen et al., 2012; Pane et al., 2006; van Bruggen et al., 2014). Weakness in the masticatory system is one of the primary causes of progressive loss of active temporomandibular range of motion (ROM) in these populations (van Bruggen, van den Engel-Hoek, Steenks, Bronkhorst, et al., 2015). Loss of active ROM and pharyngeal weakness also increase the risk of dysphagia for people with DMD and SMA because of their impact on pharyngeal mechanics (Aloysius et al., 2008; van den Engel-Hoek et al., 2009, 2013). Dysphagia leads to increased choking risks and compromised nutritional status, which requires diet modification and supplemental nutrition strategies (i.e., placement of a gastrostomy or nasogastric tube).
Progressive bulbar weakness also leads to changes in oral and cranial morphology experienced by people with DMD and SMA (Straathof et al., 2014; van den Engel-Hoek et al., 2016; Wadman et al., 2014). Among those with DMD, morphologic changes can occur as early as ages 7–10 yr (Morel-Verdebout et al., 2007). Such morphologic changes result in significant temporomandibular joint contractures with resultant reductions in both active ROM (AROM) and passive ROM (PROM; Johnson et al., 1992; McDonald, 1998; Skalsky & McDonald, 2012). Limited oral function resulting from deficits in AROM and PROM has a negative impact on both feeding and oral hygiene for people with DMD and SMA (Symons et al., 2002). In some cases, these ADLs can be compromised to such an extent that the person may require dentistry interventions under general anesthesia, but such interventions can pose life-threatening risks to people with DMD as a result of malignant hyperthermia, metabolic acidosis, and cardiopulmonary complications (Balasubramaniam et al., 2008; Mielnik-Błaszczak & Malgorzata, 2007).
Several studies have examined interventions to improve oral function in people with DMD and SMA (Ahlborg et al., 2012; Cha et al., 2010; Kawazoe et al., 1982; Nozaki et al., 2010; van Bruggen, van den Engel-Hoek, Steenks, van der Bilt, et al., 2015). These studies have primarily assessed therapeutic exercise, stretching, massage, thermal modalities, head position, and home exercise routines to affect bite force, mastication efficiency, and temporomandibular joint pain. Several of these studies examined active oral opening with variable reports of change. None of these studies examined passive oral opening or any other PROM parameters for the temporomandibular joint. Passive mandibular ROM, however, is critically important in people with DMD and SMA because it is directly linked to functional use of the mouth for respiration, feeding, swallowing safety, oral hygiene, and communication, much in the same way that passive ankle dorsiflexion is vital to ambulatory longevity in these people (Scott et al., 1981).
The TheraBite® (Figure 1; ATOS Medical, Malmö, Sweden) is a ROM device that is inserted in the mouth to provide a passive stretch to the temporomandibular joint. It has been used primarily to treat acute mandibular hypomobility in people after radiation therapy for head and neck cancer and has been shown to significantly improve oral opening, oral hygiene, and quality of life for these people (Pauli et al., 2016). The TheraBite has also been effective in the treatment of myogenic temporomandibular disorders (Kraaijenga et al., 2014). At this time, only one article has examined the use of the TheraBite with people with DMD and SMA (Ahlborg et al., 2012). This study showed consistent loss of AROM in people with DMD and consistent, although highly variable, gains in AROM in people with SMA; however, it did not assess PROM and its impact on ADLs.
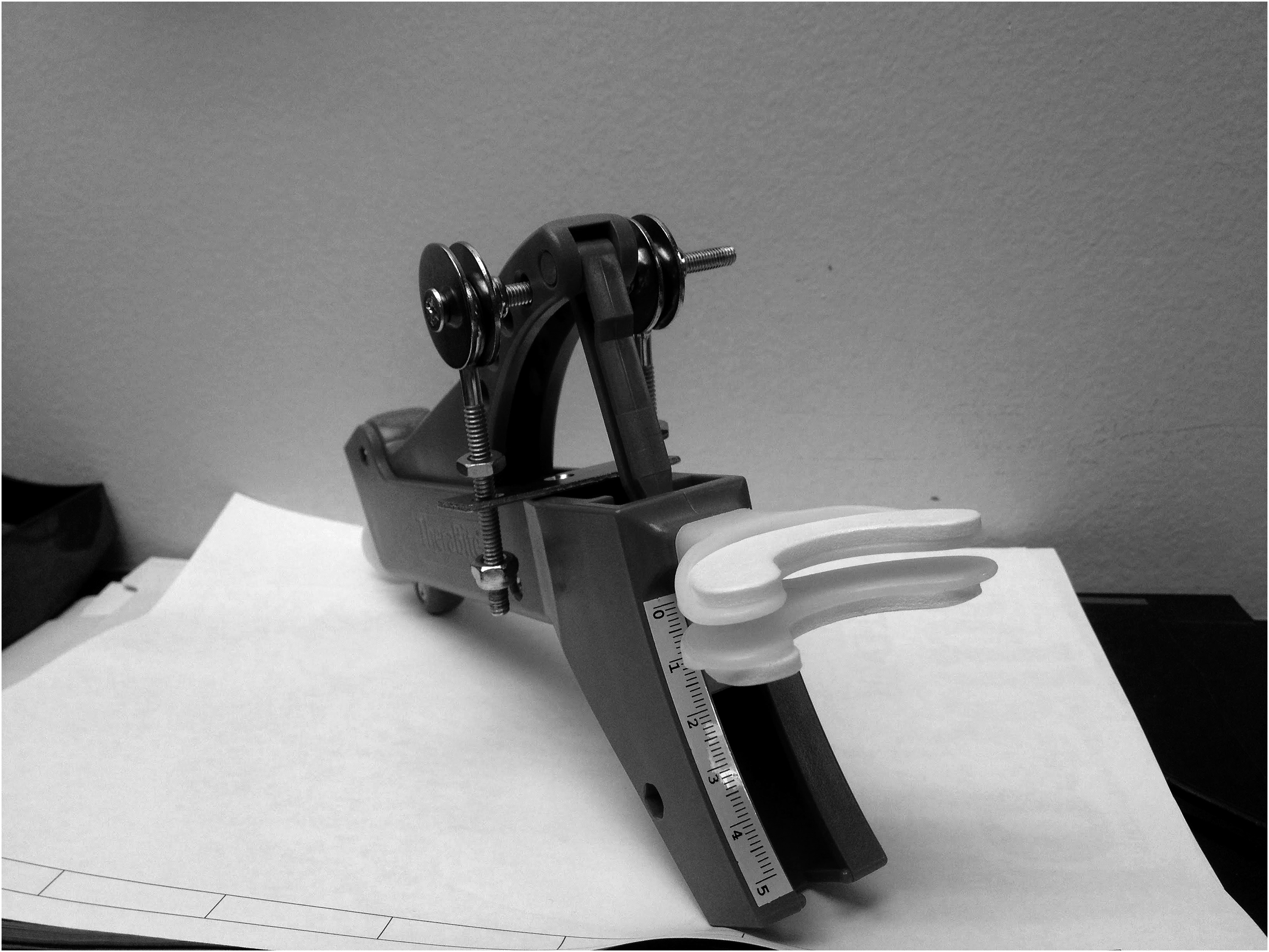
TheraBite with block mechanism in place.
Given the literature supporting improvement in temporomandibular ROM with use of the TheraBite for people with head and neck cancer and the precedent of application to the populations with DMD and SMA, we used this device in the treatment of 2 adult clients with DMD and 1 adult client with SMA (Type 2). Our primary aim was to determine whether the TheraBite would improve AROM or PROM of the temporomandibular joint. Our secondary aim was to explore whether the TheraBite would have a positive impact on ADLs or caregiver support, given that most adults with DMD or SMA require significant assistance with ADLs.
Cases
Participant 1
Participant 1 was a 32-yr-old man with a confirmed diagnosis of DMD. He required constant bilevel positive airway pressure (BIPAP) for adequate ventilation, and his Brooke Upper Extremity Scale (Brooke et al., 1981) score was 6, with hand function limited to power mobility and computer access via use of fiber-optic switches. He and his parents reported concerns with fatigue during meals, long meal durations (>30 min), and reduction in the variety of foods he could safely masticate because of fear of choking. He presented with macroglossia and reduced active oral opening that affected feeding, communication, and oral hygiene. His active oral opening at the onset of therapy was 19 mm when measured with the TheraBite disposable oral ROM scale, which is significantly less than the mean of 52.7 mm for typical men of this age group (Mezitis et al., 1989).
Intervention
Participant 1 began a course of occupational therapy with a consistent home program over the course of 30 mo. Therapy did not require any authorization by the Institutional Review Board or Medical Ethics Committee of the Children’s Hospital of Philadelphia per hospital policy because the TheraBite is commonly used in occupational and physical therapy for people with temporomandibular hypomobility caused by the effects of radiation therapy and has been proven to be safe and effective in this population (Pauli et al., 2016).
Direct therapy occurred for a period of 5 mo, initially with weekly sessions that were decreased to biweekly as the participant and caregivers demonstrated familiarity and comfort with use of the device. At this point, the home program was fully in place, and annual follow-ups were scheduled. The caregivers, consisting of nursing staff and parents, were asked to stretch the participant’s temporomandibular joint with the TheraBite for 10 sets of 30-s stretches and to repeat this 4 times per day. This protocol deviated from the manufacturer’s recommendations for adults with mandibular hypomobility after radiation therapy, which is 7 sets of 7-s stretches, repeated 7 times per day. The protocol used here is substantially longer and was specifically designed this way to combat the presence of long-standing joint contracture. The caregivers had to remove the BIPAP for each exercise trial, then reapply it for adequate respiration.
After the initial 5 mo of therapy, the participant reported variability in the degree of stretch and discomfort provided by different caregivers. Therefore, an external blocking mechanism was constructed similar to that shown in Figure 1 to ensure consistent stretching forces among caregivers. The external block, made of metal, was necessary because caregivers were able to inadvertently bend the built-in plastic blocking mechanism on the TheraBite during stretching trials. From this point onward, the TheraBite was blocked at a specific distance in relation to the adhesive ruler along the base of the device. It was at this point that we began to measure PROM. The caregivers were given autonomy to advance the external block to increase the oral opening as the participant’s tolerance permitted over time.
When the block was first added to the participant’s home program, he reported a consistent stretch from all involved in the exercise routine, which created a level of discomfort on a 10-point numeric scale of 7/10 at the belly of the masseters bilaterally. He had previously never complained of discomfort because up to that point, the stretches he had received were less aggressive and varied among caregivers. His discomfort fell to <2/10 within 2 days and never went higher than 2/10 for the duration of the program, which continued for 2 yr.
Results
As shown in Table 1, the active maximal interincisal opening decreased slightly after therapy, but passive opening increased by 6 mm (from 15 mm to 21 mm), a 40% improvement. At the end of the therapeutic course, Participant 1 subjectively reported reduced fatigue with meals and less anxiety with feeding. His father reported greater ease in completing the participant’s oral hygiene.
Active and Passive Maximal Interincisal Opening for All Participants
Note. DMD = Duchenne muscular dystrophy; SMA = spinal muscular atrophy.
Active maximal interincisal opening measured using the disposable TheraBite range of motion scale.
Measured against left central incisor.
Passive maximal interincisal opening measured using the adhesive scale on the TheraBite during stretching exercises.
Participant 2
Participant 2 was a 38-yr-old man with a confirmed diagnosis of DMD. He required a tracheostomy for external ventilation assistance and demonstrated upper extremity function similar to that of Participant 1 (Brooke Upper Extremity Scale score = 6). He and his parents reported the same concerns as did Participant 1. His active maximal interincisal opening was 16 mm when measured with the TheraBite disposable oral ROM scale, which is significantly less than the mean of 52.7 mm for typical men of this age group (Mezitis et al., 1989).
Intervention
Participant 2 was seen 4 times over the course of 20 mo during his multidisciplinary neuromuscular clinic occupational therapy consultations. Weekly therapy was not provided because of transportation limitations. The caregiver-directed home program consisted of stretches using the TheraBite for 8 repetitions of 30-s stretches 3 times per day. A custom blocking mechanism was fabricated from wood with a lacquer to prevent warping; the previously described metal blocking mechanism was uncomfortable because it pinched the participant’s mandibular lip (Figure 2). As the participant’s tolerance to stretch improved, his father shaved the block with a grinder in 1- to 2-mm increments to increase the temporomandibular ROM. The participant did not report pain or discomfort throughout the entire 20-mo period.
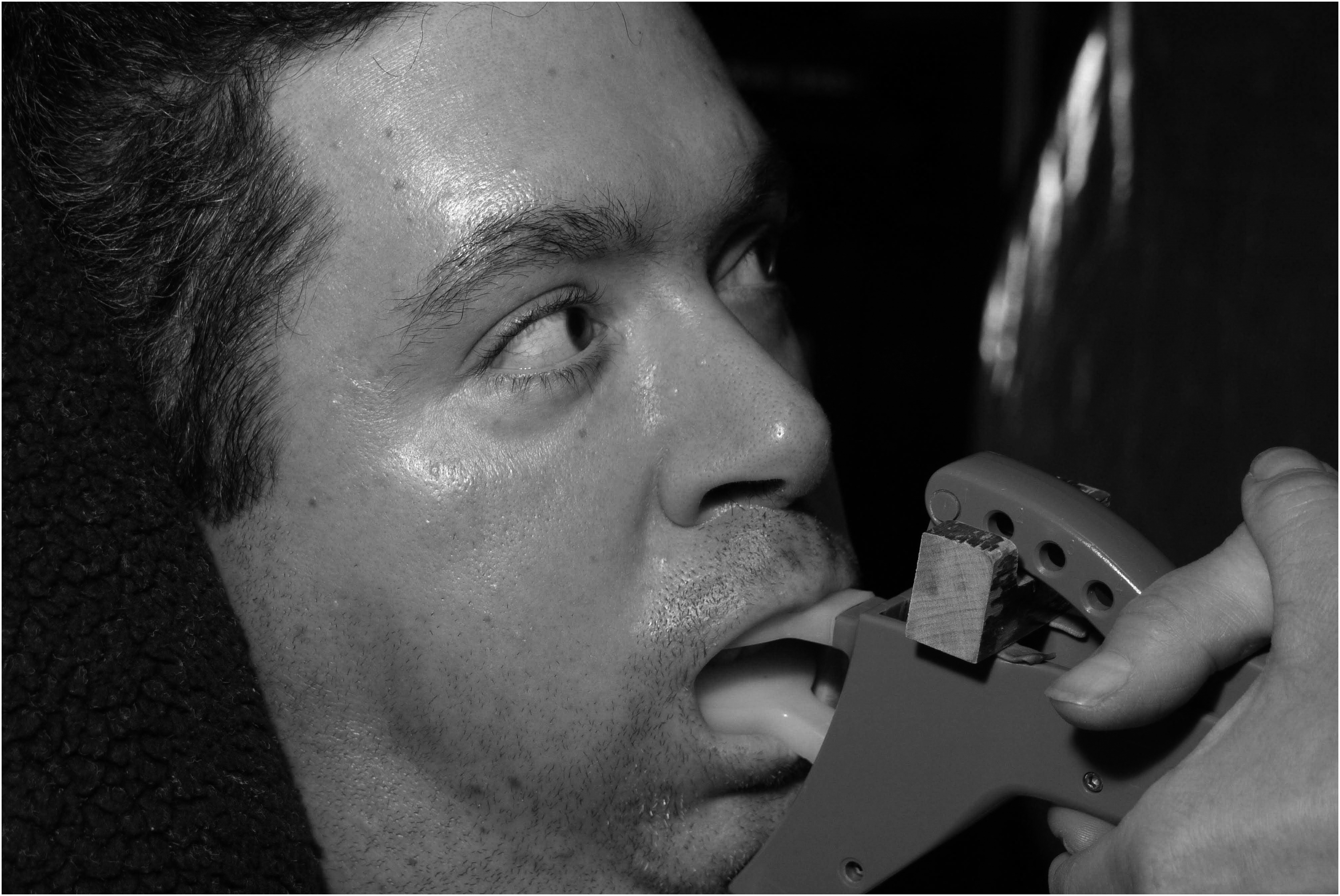
Participant 2: TheraBite open with homemade block in place.
Results
As shown in Table 1, Participant 2’s active maximal interincisal opening remained unchanged after therapy, but passive opening increased by 8.5 mm (from 13 mm to 21.5 mm), a 65% improvement. He subjectively reported reduced fatigue during feeding tasks, improved mastication performance with soft solid food, and reduced meal duration. His father reported greater ease of completion of the participant’s oral hygiene.
Participant 3
Participant 3 was a 32-yr-old woman with SMA Type 2 who required BIPAP ventilation at night and use of sip intermittent positive pressure ventilation during the day. Her upper extremity function was limited to power mobility via use of a joystick with minimal right arm movements. Decreased mandibular opening impaired her ability to eat meals off a spoon or without excessive spillage. She also reported difficulty with bolus management. Her active maximal interincisal opening at the onset of therapy was 15 mm when measured with the TheraBite disposable oral ROM scale, which is significantly less than the mean of 49.52 mm for women (Mezitis et al., 1989). Fatigue also played a major role in her oral hygiene and feeding function. She decreased active opening to 11 mm after two attempts during her initial examination.
Intervention
Participant 3 was followed for a total of 7 mo, with the frequency starting at every 2 wk, then decreasing to every 2 mo as she and nursing staff became comfortable with the home exercise program. Her therapy regimen consisted of 5 repetitions of 10-s stretches completed every hour. An external blocking system was again used to maximize consistency among caregivers (Figure 3). In this case, a stack of tongue depressors served as the inflexible block. The participant did not report pain or discomfort.

Participant 3: TheraBite with blocking system in place.
Results
As shown in Table 1, the participant’s active maximal interincisal opening improved from 15 mm to 20 mm after therapy, a 33% gain. Passive opening improved from 15 mm to 22 mm, a 47% gain. No improvement in fatigue was reported, but both the participant and her caregivers reported improvements with oral hygiene and mastication efficiency with soft-solid foods.
Discussion
Progressive loss of oral opening among people with DMD and SMA has been documented in the literature, and it is recommended that clients with DMD and SMA be screened for this loss, given the importance of adequate oral opening in feeding, communication, and oral hygiene (van Bruggen et al., 2011, 2014; van Bruggen, van den Engel-Hoek, Steenks, Bronkhorst, et al., 2015). Previous studies reported no significant change in active oral opening for people with DMD using the TheraBite (Ahlborg et al., 2012; Nozaki et al., 2010; van Bruggen, van den Engel-Hoek, Steenks, van der Bilt, et al., 2015), which is in agreement with the experience of the 2 participants with DMD. TheraBite use in the SMA population has revealed inconsistent gains in temporomandibular AROM (Ahlborg et al., 2012), but our results show improvement for our participant with SMA. Our study demonstrates, for the first time, that TheraBite treatment can improve temporomandibular PROM among people with DMD and SMA, and it can have a positive impact on ADLs.
In comparison with Ahlborg et al.’s (2012) findings, our patients with DMD had a lesser reduction in AROM: Of the 6 patients with DMD in Ahlborg et al.’s report, 5 lost ROM, and 4 lost as much as 2–4 mm over the course of 21 mo of treatment. Although our participants with DMD did not gain AROM either, only 1 of our 2 participants with DMD lost AROM over 24 mo of treatment, and his loss was minimal at 1 mm. Moreover, our results validate Ahlborg et al.’s findings that the TheraBite can improve active maximal interincisal opening in people with SMA, even if the gains they observed were inconsistent (ranging from 13% to 29% among their 3 participants). Ahlborg et al.’s study, however, differs from ours because they did not use a blocking mechanism to ensure consistent stretching forces among the caregivers providing the therapy. In addition, our participant with SMA participated in therapy for roughly one-third the amount of time as the people with SMA in the Ahlborg et al. study. Our results thus suggest that use of the external blocking mechanism and a more aggressive stretching routine may lead to higher gains in AROM with less therapeutic intervention.
The loss of AROM and PROM has been hypothesized to be the result of weakness and fibrosis in the submental and suprahyoid muscles, respectively (Archer et al., 2013; van den Engel-Hoek et al., 2012). This weakness in people with DMD is not expected to improve with TheraBite therapy, which is likely the reason for the discrepancy we observed between AROM and PROM improvements in our participants. Our results suggest that improved PROM after TheraBite use may reduce long-term temporomandibular tightness, given that regular stretching regimens started early in the life of people with DMD can decrease the progression of contracture (Scott et al., 1981). Note that mandibular hypomobility in people with DMD is the result of soft-tissue contracture, not bony ankylosis, which would be uncorrectable without surgical intervention (Skalsky & McDonald, 2012).
Our results also suggest that use of the TheraBite with people with DMD and SMA is safe and well tolerated. During the course of therapy, none of the participants reported significant discomfort (>2/10). The only exception occurred during the first therapy session, in which Participant 1 used the external blocking mechanism, but his discomfort resolved spontaneously within 2 days. This result indicates that the forces used to provide the stretch were similar to those used by therapists when prescribing common stretching routines for other areas of the body, such as ankles, elbows, and shoulders (Prabhu et al., 2013).
Limitations
This study had a few limitations. First, it was a retrospective study. Because of environmental and medical factors, it was not possible to determine the true frequency with which therapy was delivered in the home setting; however, the participants and caregivers reported adherence to the protocol. Second, the 3 participants do not represent the full age span of the population with DMD or SMA because they were all late stage with longstanding temporomandibular joint contractures. Finally, we were able to capture reported improvements in fatigue, feeding efficiency, oral hygiene, and caregiver burden only through subjective report.
Implications for Occupational Therapy Practice
The results of this study have the following implications for occupational therapy practice:
Occupational therapists and occupational therapy assistants have unique skills to treat temporomandibular joint dysfunction and its sequelae in this population.
Temporomandibular joint dysfunction must be addressed in this population to improve quality of life and reduce premature morbidity.
Ongoing temporomandibular joint assessment during the lifespan of people with DMD and SMA is a best-practice recommendation and will allow for improved identification of impairment.
Intraoral interventions with the TheraBite may improve ADL function in these clients.
Conclusion
Improving temporomandibular PROM may serve to prolong feeding efficiency and safety for people with DMD and SMA, which is essential to elongation of the lifespan (Botteron et al., 2009). In this study, the TheraBite was used as a way to significantly improve PROM for our participants. This study suggests the importance of using a blocking mechanism to improve outcomes and the relevance of customizing the blocking method to the morphological facial differences, the varying equipment used for external ventilation, and personal and family routines.
Additional research is needed to understand the natural history of temporomandibular ROM problems in people with DMD and SMA and how to measure functional outcomes associated with any gains in ROM or fatigue. It will also be important to determine whether introducing TheraBite usage earlier in disease progression will prolong oral function and its effect on ADLs. The optimal TheraBite usage schedule and the persistence of the changes seen here are also topics for future research, as are the characteristics of a follow-up program that are needed to maintain the gains.
Footnotes
Acknowledgments
All research was conducted at The Children’s Hospital of Philadelphia.