
Abstract
Persistent pain is a common experience in childhood (King et al., 2011), and a small proportion of children and adolescents develop persistent pain that substantially interrupts daily functioning, prompting families to access tertiary care for treatment (Konijnenberg et al., 2005). Pain is primarily a protective response, an alarm signal that is experienced in the body (Tabor et al., 2017) and evoked by sensory changes that signify bodily, psychological, or social threat (Eisenberger, 2012; Kozlowska et al., 2008). The expression of pain and distress alerts others to potential threat or to the need for protection and care (Hadjistavropoulos et al., 2011). As such, pain is a biological process that has an ecological context (Bar-Shalita et al., 2015). Evidence has suggested that children and adolescents respond to changes in the internal and external environments through sensory modulation processes (Miller et al., 2007). Sensory modulation is associated with attachment in young children (Whitcomb et al., 2015), school-age children, and adolescents (Purvis et al., 2013). Attachment processes activated by distressing circumstances influence sensory-related behavioral responses (Whitcomb et al., 2015). Together, attachment and sensory modulation processes may influence the experience of persistent pain, affecting functioning. This proposition requires empirical investigation in pediatric populations with persistent pain, with the findings underpinning and informing future clinical investigations.
Children and adolescents interact with the environment through their sensory system and the complex process of sensory modulation (Miller et al., 2007), which encompasses the registration and integration of sensory input from multiple modalities and the interpretation of events according to previous experience, regulation of arousal, and organization of adaptive responses. Children and adolescents register sensory input with varying levels of sensitivity and develop patterns of sensory modulation according to both genetic predispositions and exposure to various life circumstances (Belsky & Pluess, 2009). Children with sensory modulation disorder (SMD; Miller et al., 2007) have been found to perceive painful sensory input as being of higher intensity than those without SMD (Bar-Shalita et al., 2009). Research has demonstrated that healthy children with SMD have lower participation in daily activities than those without SMD (Bar-Shalita et al., 2008; Chien et al., 2016). Adolescents with persistent pain are more likely to have SMD, with associated higher disability and poorer quality of life (QOL; Sinclair et al., 2019).
The protective strategies and responses of children and adolescents with persistent pain in contexts that are perceived to be threatening are influenced by their previous experiences, particularly interactions with their parents (Crittenden & Landini, 2015). These previous interactions have created patterns of attachment. Attachment patterns have two fundamental dimensions: anxiety and avoidance (Bartholomew, 1990). Higher levels of each dimension (i.e., insecure attachment) theoretically predispose children and adolescents to persistent pain and impaired function through (1) cognitive appraisals of threat, (2) autonomic responses that increase hypervigilance and neural sensitivity, (3) pain-signaling behaviors to elicit responses from caregivers, and (4) behavioral withdrawal (Donnelly & Jaaniste, 2016; Kozlowska, 2009). Insecure attachment is correlated with higher pain severity in healthy adolescents (Tremblay & Sullivan, 2010); however, associations between attachment and function among children and adolescents with persistent pain have been inconsistent in the literature (Laird et al., 2015; Ratnamohan & Kozlowska, 2017). Although further work is needed to better understand the associations between insecure attachment and functional disability for children and adolescents with persistent pain, behaviors related to insecure attachment patterns may provide a feasible mediating pathway to functional disability and poorer QOL.
On the basis of this literature, the research questions investigated in this study were as follows:
Are sensory modulation patterns associated with attachment patterns, pain intensity, functional disability, and QOL in a clinical sample of children and adolescents with persistent pain?
Does children’s and adolescents’ insecure attachment mediate the relationship between sensory modulation and pain intensity, function, and QOL?
We hypothesized that
Sensory overresponsiveness or sensory underresponsiveness would be associated with higher insecure (anxious or avoidant) attachment, higher pain intensity, higher functional disability, and lower QOL, and
Children’s and adolescents’ insecure attachment would mediate the relationship between sensory modulation and pain intensity, function, and QOL.
Method
To address the research questions, we used a cross-sectional quantitative design. Ethical approvals were obtained from the Royal Children’s Hospital Ethics Committee (HREC Ref. No. 35119 A) and the University of Queensland (2015001033). Participants were children and adolescents attending a tertiary pain management clinic for assessment (part of this sample has previously been described in a related preliminary study; see Sinclair et al., 2019).
Procedure
From October 2015 to May 2017, all parents, adolescents, and children attending assessment appointments were invited to participate in the study. Families routinely complete standardized questionnaires relating to pain intensity, function, and QOL as part of the assessment procedure. Children (ages 8–12 yr) and adolescents (ages 13–18 yr) complete questionnaires independently. Questionnaires are completed either via a protected online link or in paper form during the appointment. For this study, participants also completed a sensory modulation questionnaire and an attachment questionnaire. Adolescents and parents were provided with information and consent forms before the clinic appointment. To be included in the study, children and adolescents needed to meet the following eligibility criteria: age 8–18 yr, with pain of at least 3 mo duration or a diagnosis of a specific pain disorder, such as complex regional pain syndrome (CRPS), consistent with the referral criteria for the pain clinic, and English speaking, with the capacity to answer the questionnaires independently. Children or adolescents with cognitive or physical developmental delay (who were unable to complete questionnaires independently) were excluded.
Measures
Demographics
Parents provided demographic information (child or adolescent age, gender, duration of persistent pain experienced, country of origin, and address). The family’s socioeconomic status (SES) was ascertained from the family’s residential address (Pink, 2013). The treating medical pain physician diagnosed participants who met formal diagnostic criteria for CRPS; for other participants, the primary pain site was categorized.
Pain Intensity
Children and adolescents rated the intensity of their pain on an 11-point visual analog scale (VAS; Scott et al., 1977) ranging from 0 (no pain) to 10 (worst pain ever). Children and adolescents were asked to retrospectively report their average pain intensity over the past week. The VAS has been validated for children ages 8–18 yr and correlates well with the Faces Pain Scale (Hicks et al., 2001).
Function
Functional disability was measured with the Functional Disability Index (FDI; Walker & Greene, 1991). This self-report measure of activity limitations is composed of 15 items that ask about limitations over the past 2 wk. Each item is scored on a 5-point scale ranging from 0 (no trouble) to 4 (impossible). The FDI has high levels of internal consistency (α = .91 for girls and .87 for boys) and high test–retest reliability (Walker & Greene, 1991).
Quality of Life
Children and adolescents self-reported the extent to which they have problems with physical, emotional, social, and school-related functioning on the Pediatric Quality of Life Inventory (PedsQL; Varni et al., 2001). Items for each domain are rated on a 5-point scale ranging from 0 (never have problems) to 4 (almost always a problem). Scores are reversed and linearly transformed, according to manualized instructions, into a scale ranging from 0 to 100; higher scores indicate higher QOL and functioning. The PedsQL has been validated in children ages 8–18 yr and found to have strong internal consistency (α = .88; Varni et al., 2001).
Attachment Pattern
Children’s and adolescents’ attachment pattern in their relationship with their parents was measured using the Experiences in Close Relationships Scale–Revised (child/adolescent version; ECR–RC; Brenning et al., 2011). The scale is made up of 36 items (18 items measure anxious attachment, and 18 items measure avoidant attachment), each of which is rated on a 7-point scale, ranging from 1 (strongly disagree) to 7 (strongly agree). For convenience, children and adolescents were invited to complete one ECR–RC, answering questions that related to the parent who attended the clinic assessment appointment. This was considered suitable because of the high level of correspondence between results when children and adolescents complete the measure for mothers and fathers separately (Brenning et al., 2011). The ECR–RC has demonstrated a clear, interpretable factor structure; high internal consistency (α = .89–.94); and subscales that correlate with other measures of attachment (Brenning et al., 2011).
Sensory Modulation
Sensory modulation patterns of children and adolescents were measured using the age-appropriate version of the Sensory Profile. The Short Sensory Profile 2 (SSP2; Dunn, 2014) has been validated for children ages 3 yr–14 yr, 11 mo and was completed by the caregiver for children ages 12 yr and younger. The SSP2 contains 34 questions and has adequate internal reliability (α = .79–.86) and moderate correlations with related measures (Dunn, 2014).
The Adolescent/Adult Sensory Profile (AASP; Dunn, 1999) is a self-report measure that is validated for use by adolescents ages 11 yr and older and adults and was completed by adolescents ages 13–18 yr. Internal reliability is adequate (α = .65–.75; Dunn, 1999). The scores for both measures are summarized into four quadrants (sensory sensitivity, sensory avoiding, sensory seeking, and low registration), derived from two dimensions reflecting (1) the thresholds at which people register sensory information in daily life and (2) active or passive behavioral responses.
Continuous scores from the SSP2 and the AASP were standardized for each quadrant to enable their incorporation in the same statistical analyses.
Data Analysis
Statistical analysis was performed using Stata (Version 13.0; StataCorp, College Station, TX). Descriptive statistics (Tabachnick & Fidell, 2013) were used to check for normality of continuous variables before performing statistical analysis. The associations among demographic variables (age, gender, SES, pain site) and the study variables (four continuous sensory variables, two child/adolescent attachment subscales, pain intensity, function, and four QOL variables) were examined using the appropriate method: one-way analyses of variance (ANOVAs), independent t tests, or correlations. Post hoc pairwise comparisons of the means were examined to determine the differences between groups in the ANOVAs. Variables that were significantly associated with function and QOL were controlled for in subsequent analyses.
A series of stepwise hierarchical multiple regressions was performed to ascertain whether sensory modulation or attachment variables independently predicted functional disability or QOL. Separate models were run for each dependent variable: functional disability and physical, emotional, social, and school-related QOL. In the first step, the demographic variables that were significantly associated with functional disability or QOL in the preliminary analyses were entered into the equation. In the second step, the predictor variables (sensory modulation and attachment variables) were added.
We performed a second series of regression analyses to ascertain whether anxious or avoidant attachment (mediator variable) mediated any of the identified relationships between sensory modulation (independent variable) and disability or QOL (dependent variable). Initial calculations considered whether sensory modulation variables significantly predicted functional disability or QOL when covariates were included in the equation (Figure 1a, Path c). If this relationship was significant, we conducted further calculations to ensure the conditions articulated by Baron and Kenny (1986) were met—(1) Variations in the level of the independent variable significantly accounted for variations in the mediator (Figure 1b, Path a), (2) variations in the mediator significantly accounted for variations in the dependent variable (Figure 1b, Path b), and (3) variations in the mediator significantly accounted for variations in the indirect path (Figure 1b, Path c′)—and the independent variables no longer significantly predicted the dependent variables when Paths a and b were controlled for.
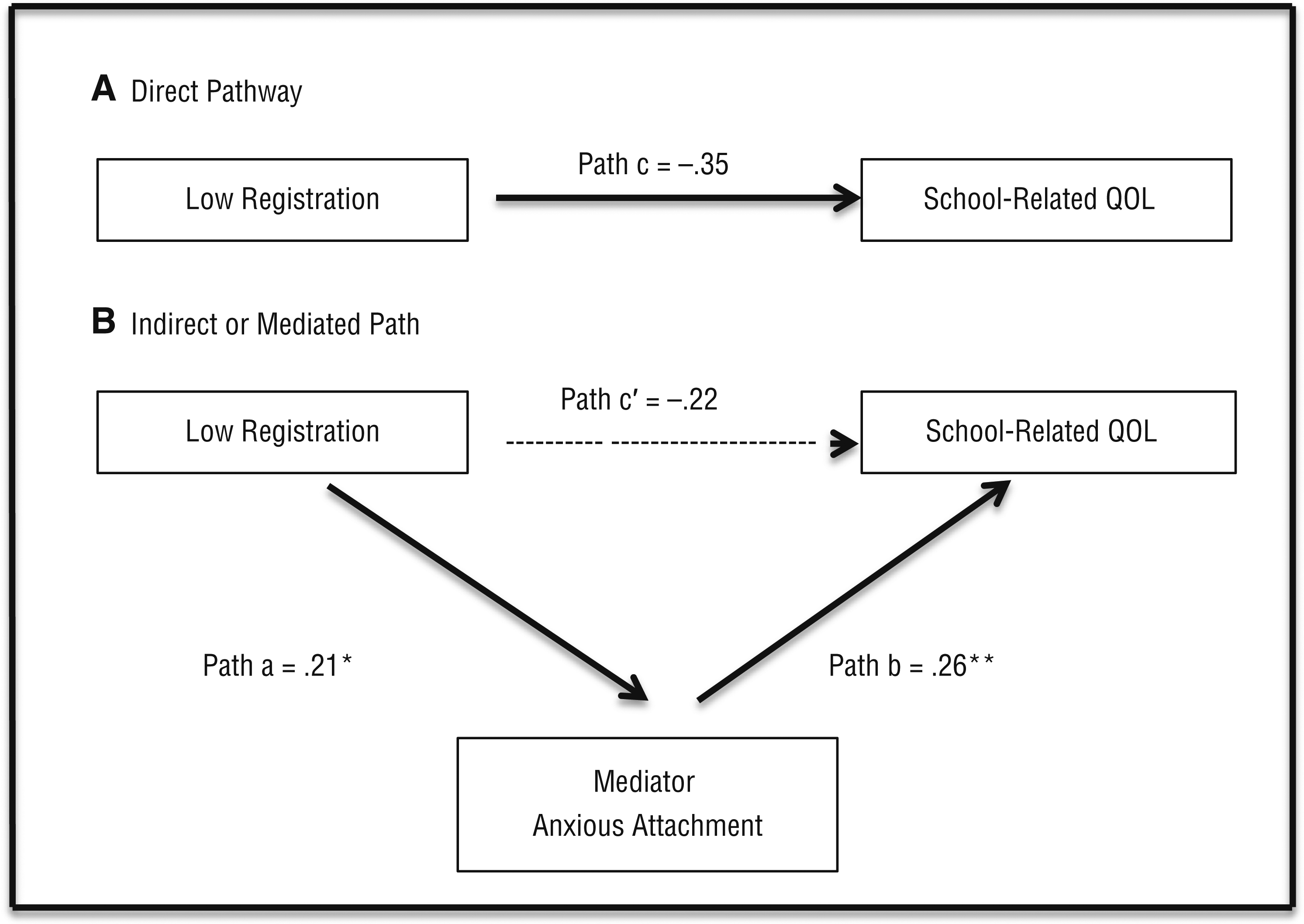
Representation of the (A) direct pathway between low registration and school-related QOL and (B) the indirect pathway between low registration and school-related QOL, mediated by anxious attachment.
If the independent variable significantly predicted the dependent variables but the effect was reduced in comparison with the effect in the direct path, we calculated the percentage of the total effect accounted for by the mediator by dividing the unstandardized β value of Path c′ by the unstandardized β value of Path c, and then subtracting this value from 1 (1 − c′/c), as recommended by Rucker et al. (2011). Values >.80 indicate complete mediation, whereas values <.80 indicate that attachment partially mediates the relationship. The bootstrap method (Preacher & Hayes, 2004) was performed to test the significance of the indirect effect of the mediator. Residual variables were tested for multicollinearity after the regression analyses (Tabachnick & Fidell, 2013).
Results
Participants
From October 2015 to July 2017, 152 children (ages 8–12 yr) and adolescents (ages 13–18 yr) were referred to multidisciplinary team assessment at the Children’s Pain Management Clinic. Of these, 75 adolescents (68 girls, 7 boys) and 39 children (30 girls, 9 boys; N = 114) met study criteria, attended with their parent or grandparent, gave consent to participate, and provided a complete data set. The country of origin for 113 participants was Australia, 3 of whom were Aboriginal or Torres Strait Islanders, and 1 participant was born overseas. Demographic information is presented in Table 1.
Note. CRPS = complex regional pain syndrome; M = mean; SD = standard deviation; SES = socioeconomic status.
Percentages are calculated on the basis of row totals.
For SES, the index summarizes variables (education level and resources) that indicate either relative advantage or disadvantage on a continuum where 10 = higher levels of socioeconomic advantage and 1 = lower levels of socioeconomic advantage.
Independent-samples t tests showed that compared with girls, boys received significantly lower scores on the FDI (boys, mean [M] = 16.81; girls, M = 24.43; t[109] = −2.59, p = .01) and higher scores on the Physical QOL Scale (boys, M = 62.30; girls, M = 41.77, t[109] = 3.56, p < .001). As a result, gender was retained as a covariate in further analyses of these dependent variables. Descriptive data for continuous demographic and study variables are provided in Table 2. Standardized Cronbach’s αs ranged between .71 and .77.
Note. AASP = Adolescent/Adult Sensory Profile; ECR–RC = Experiences in Close Relationships Scale Revised for Children; FDI = Functional Disability Index; PedsQL = Pediatric Quality of Life Scale; QOL = quality of life; SES = socioeconomic status; SSP2 = Short Sensory Profile 2; VAS = visual analog scale.
Means and standard deviations are reported for the unstandardized variables; however, correlations used combined standardized sensory modulation variables (low registration, sensory seeking, sensory sensitivity, and sensory avoiding).
p < .05. **p < .01. ***p < .001.
Correlational Analysis
Age was significantly negatively correlated with school-related QOL and positively correlated with avoidant attachment (see Table 2); thus, age was retained as a covariate in regression analyses with school-related QOL. SES was not significantly correlated with any of the study variables. Pain intensity correlated positively with functional disability and negatively with physical and emotional QOL, but it was not correlated with sensory modulation or the attachment variables. Low registration correlated positively with both anxious and avoidant attachment and negatively with emotional, social, and school-related QOL. Sensory seeking was correlated negatively with anxious attachment. Sensory sensitivity correlated in expected directions with all disability and QOL variables, but sensory avoiding correlated only with emotional, social, and school-related QOL. Neither sensory sensitivity nor sensory avoiding correlated with the attachment variables. Anxious attachment was significantly negatively correlated with social and school-related QOL, and avoidant attachment was negatively correlated with school-related QOL.
Hierarchical Multiple Regression
We performed hierarchical multiple regression analyses to ascertain whether sensory modulation or attachment variables predicted functional disability and QOL. Because sensory seeking was not significantly correlated with functional disability or QOL, we did not include it in the regression analyses.
Functional Disability
Pain intensity and gender were included as covariates in Step 1 of the model. In Step 2, pain intensity (β = .50, t[107] = 6.10, p < .001) and sensory sensitivity (β = .31, t[107] = 2.33, p < .05) remained direct significant predictors for disability; gender was not a significant predictor (β = .06, t[107] = 0.74, p = .46). Sensory sensitivity accounted for 31% of the variance in disability. Tests for multicollinearity indicated low levels of collinearity between the predictor variables.
Physical, Emotional, Social, and School-Related Quality of Life
Hierarchical regression equations revealed that neither the sensory modulation nor the attachment variables, entered in the second step, predicted physical QOL. For emotional QOL, pain intensity (β = −.25, t[102] = −2.69, p < .01) remained the only significant predictor. Sensory modulation and attachment did not significantly predict social QOL when other variables were included in the equations. For school-related QOL, age was a significant predictor of lower QOL. In the second step, low registration (β = −.23, t[102] = −2.03, p < .05) and anxious attachment (β = −.07, t[102] = −1.63, p < .01) also significantly predicted school-related QOL when age and other sensory modulation and attachment variables were included as covariates. The test for multicollinearity indicated low levels of collinearity between the predictor variables; therefore, all predictor variables had a suitably independent effect on school-related QOL.
Mediation Analyses
Hierarchical analyses revealed that sensory modulation variables did not significantly predict physical, emotional, or social QOL; thus, anxious and avoidant attachment could not mediate these relationships. Although sensory sensitivity independently predicted functional disability, variations in sensory sensitivity did not significantly account for variations in anxious (β = .13, t[105] = 1.44, p = .15) or avoidant (β = −.03, t[105] = −0.32, p = .74) attachment (Path a). Thus, anxious and avoidant attachment could not mediate the relationship between sensory sensitivity and functional disability. A series of regression equations tested whether anxious or avoidant attachment mediated school-related QOL, with age included as a covariate. As demonstrated in Figure 1, anxious attachment was found to mediate the relationship between low registration and school-related QOL. The percentage of the total effect accounted for by the mediator was calculated to be 11%, indicating that low registration had both direct and indirect effects on school-related QOL and that anxious attachment was a partial mediator in this relationship.
Discussion
In this study, we investigated the question of whether sensory modulation patterns were associated with attachment patterns, pain intensity, functional disability, and QOL in a clinical sample of children and adolescents with persistent pain. We also considered whether child and adolescent insecure attachment mediated the relationship between sensory modulation and pain intensity, function, and QOL.
Sensory modulation patterns were associated with anxious attachment, avoidant attachment, or both for children and adolescents with persistent pain; these results partially supported the first hypothesis. First, higher sensory seeking correlated with lower anxious attachment (or more secure attachment). This finding suggests that children and adolescents with persistent pain and higher sensory seeking have a history of emotionally attuned parental support in threatening environments. Second, higher low registration was associated with higher anxious and avoidant attachment. Purvis et al. (2013) found a similar correlation between sensory deficits and insecure attachment for children and adolescents attending camp who had a history of trauma. Ratnamohan and Kozlowska (2017) found that a high proportion of children and adolescents with persistent pain had both insecure attachment and a history of exposure to adverse life circumstances. Higher low registration among children and adolescents with persistent pain may be related to previous developmental trauma, which predisposes such children and adolescents to insecure attachment (Crittenden, 2008).
In contrast to expectations in the first hypothesis, no significant correlations were revealed between either sensory sensitivity or sensory avoiding (i.e., lower sensory threshold patterns) and anxious or avoidant attachment among children and adolescents with persistent pain. Given theoretical expectations and previous findings that higher sensory sensitivity has been associated with anxious attachment and sensory avoiding has been associated with avoidant attachment in healthy adult samples (Jerome & Liss, 2005; Levit-Binnun et al., 2014), the current findings are somewhat surprising. Notably, in a study by Meredith et al. (2016), the association between sensory sensitivity and anxious attachment was not retained when controlling for stress. Although we did not measure stress in the current study, we would expect children and adolescents experiencing persistent pain to also be experiencing high levels of distress (Schaaf et al., 2003), which may have influenced the results. It is also possible that results may differ for children relative to adults. More research is required with both populations to better understand this relationship.
Neither attachment patterns nor sensory modulation patterns were associated with pain intensity, in contrast to our first hypothesis and theoretical expectations. Our results are consistent with Ratnamohan and Kozlowska (2017), who found that insecure attachment was not associated with pain intensity in a clinical sample of children and adolescents with persistent pain, but they contrast with those of laboratory studies of healthy children and adults, among whom sensory overresponsiveness has been associated with higher pain intensity and duration (Bar-Shalita et al., 2009, 2012, 2014). Bar-Shalita et al. (2015) demonstrated that there was no significant statistical difference between adults with sensory overresponsiveness and those without SMD in relation to pain sensitivity, although pain sensitivity was positively correlated with sensory overresponsiveness in the context of multisensory processing related to daily life. For children and adolescents with persistent pain, avoidance behaviors associated with SMD may limit exposure to multisensory input and thereby limit the experience of aversive emotional responses to sensation and, thus, pain.
We identified complex relationships among sensory modulation, attachment, functional disability, and QOL. Once attachment variables were statistically controlled, sensory sensitivity remained a significant predictor only of functional disability. Attachment did not mediate this relationship. This suggests that, for some children and adolescents with persistent pain, sensory sensitivity that is independent of attachment processes is related to disability. Low registration and anxious attachment both independently predicted school-related QOL when other sensory modulation and attachment variables were statistically controlled. Although other studies have considered the associations between these constructs separately (Chien et al., 2016; Laird et al., 2015), this study is the first to demonstrate the independent effect of sensory modulation and attachment on QOL.
We found that anxious attachment partially mediated the relationship between low registration and school-related QOL, which supports our second hypothesis. That is, for children and adolescents with persistent pain, low registration had a direct effect on school-related QOL, and for those with anxious attachment the effect was enhanced. Low registration has been found to be associated with anxiety in typically developing boys and in boys with SMD (Bart et al., 2017). Anxiety experienced by children and adolescents with lower sensory awareness may trigger hyperactivating behavioral responses related to higher anxious attachment (Crittenden, 2008; Mikulincer et al., 2003). The primary aim of attachment-related activating responses, which include pain signaling, is to elicit protection from caregivers when sensory information is perceived to be threatening (Kozlowska, 2009). The mediating effect of anxious attachment on the association between low registration and school-related QOL suggests that in challenging, pain-provoking circumstances, children with low registration may engage in strategies consistent with anxious attachment behaviors, such as displaying pain and prioritizing closeness to parents, to manage distress. Maintaining safety by remaining close to parents rather than engaging in school-related tasks may potentially inhibit school-related QOL.
Limitations and Future Research Recommendations
Several limitations should be considered. First, measurement bias may exist. Self-report measures may have been open to bias related to memory, mood, and, for the child, the presence of parents when completing the questionnaire, all of which may have influenced our results. Moreover, parents completed the SSP2 for children ages 12 yr and younger. Because sensory perception is a subjective experience, the outcomes may have been biased by the parents’ observation; children may have provided different information relating to their own experience of sensory modulation if they had been able to complete a self-report measure.
Second, the sample size restricted use of more complex statistical models (such as structural modeling equations) that take into account complex interactions between multiple variables. Third, from an ecological perspective, affordances in the environment have an impact on sensory modulation and attachment processes and create facilitators and barriers to function, which needs to be considered in future studies. Fourth, the number of years that children and adolescents had experienced persistent pain may have influenced their QOL; this information should be collected as a continuous variable for testing in future studies. Fifth, although the ratio of girls and boys in the current study reflects that found among young people with persistent pain, evidence has shown that the frequency of persistent pain increases with age for girls (King et al., 2011), and the gender imbalance in this study may limit generalization of the findings to boys.
Implications for Occupational Therapy Practice
The results of this study revealed associations between sensory modulation and attachment patterns (relational patterns of interaction), functional disability, and QOL that may warrant consideration when addressing the functional capacity of children or adolescents with persistent pain.
Previous exposure to trauma and patterns of insecure attachment need to be considered for children and adolescents with persistent pain and higher low registration.
Addressing sensory sensitivity may improve participation in daily activities for children and adolescents with persistent pain.
For children and adolescents with low registration, findings reinforce the need to consider attachment-based therapies to support school-related QOL.
Conclusion and Future Recommendations
This study is, to our knowledge, the first to investigate relationships among sensory modulation, attachment, pain, QOL, and functioning in a clinical sample of children and adolescents with persistent pain. Participants with low registration were found to have both higher anxious and higher avoidant attachment, whereas those with higher sensory seeking had lower anxious (or more secure) attachment. Sensory modulation and attachment were not associated with pain intensity; however, higher sensory sensitivity predicted functional disability. Low registration and anxious attachment predicted lower school-related QOL, with anxious attachment mediating the relationship between low registration and poorer school-related QOL. Results support the need for further research and consideration of the interactions between sensory modulation and attachment when addressing functional abilities and QOL in treatment.
Footnotes
Acknowledgment
This research was partially funded by an Australian Post-Graduate Award from the University of Queensland. It was conducted at the Royal Children’s Hospital, Melbourne, Victoria, Australia, in conjunction with the University of Queensland, Brisbane, Queensland, Australia.