
Abstract
Palliative care is noncurative comfort care provided at any stage of terminal illness (National Institute on Aging, 2018). Hospice is a specialty of palliative care: end-of-life care for people with a life expectancy of 6 mo or less at the end stages of a terminal illness (National Institute on Aging, 2018). Approximately 1.49 million Medicare beneficiaries receive hospice annually (National Hospice and Palliative Care Organization, 2019).
As their disease progresses, hospice clients struggle to uphold daily routines and participate in valued occupations (Peoples et al., 2017). Occupational role loss contributes to a loss of self-identity, lack of daily structure, and social isolation (Eriksson et al., 2016). Continued occupational participation helps people with terminal illness adapt to end-of-life transitions. In a qualitative study of 47 people living with cancer, involvement in daily occupations, regardless of declining functional performance, provided a sense of pleasure and competence (Svidén et al., 2010). A phenomenological study of 8 people with life-limiting illness revealed that occupational engagement helped them live with dying by distracting them from their illness, refocusing them on relationships, and revealing value in ordinary tasks (Lala & Kinsella, 2011). Sustained occupational engagement appears essential at the end of life.
However, occupational needs of hospice clients are typically marginalized because of lack of rehabilitative potential rather than refocused toward supported participation (Schleinich et al., 2008). Hospice clients report unmet occupational needs and desire to be more engaged in aspects of their self-care (Schleinich et al., 2008). In a qualitative study of 73 people living with cancer, several participants attempted to self-manage their occupations, but participant-developed compensatory strategies were often counterproductive (Peoples et al., 2017). Hospice providers need to increase attention to clients’ occupational needs.
Occupational therapy practitioners are highly qualified to address the occupational needs of hospice clients. With consideration of personal, environmental, and contextual factors, practitioners facilitate participation through modification of occupations and the environment, compensatory strategies, caregiver training, and bereavement care (Hammill et al., 2014; Mills & Payne, 2015; Pickens, 2011). Specific to this area of care, practitioners have been found to integrate their understanding of the dying process in helping clients maximize occupational skills while supporting them through physical, emotional, and existential loss and preparing them for death (Hammill et al., 2014).
Despite its unique assets, occupational therapy remains underused in hospice care. Lack of research on the efficacy of hospice occupational therapy undermines awareness of occupational needs, integration of occupation-based interventions, and allocation of financial resources for occupational therapy services (Keesing & Rosenwax, 2013). The paucity of supporting evidence may be related to the lack of established outcome measures that distinguish occupational therapy–specific outcomes from outcomes related to the rest of the interdisciplinary team in hospice care (Cooper & Kite, 2015; Eva, 2006; Miller & Cooper, 2011).
With 40% of the U.S. population living with a chronic illness and the older adult population exponentially increasing, people will foreseeably live longer with incurable states and die of more complicated disease processes (National Health Council, 2014; Wan et al., 2016). The demands for innovative and resourceful hospice care will increase. To better serve hospice clients, the occupational therapy profession must validate the efficacy of occupation-based interventions with outcome studies.
A scoping review offers a framework to analyze an emerging area and pinpoint knowledge gaps in a limited literature base by posing a broad research question and investigating published and gray literature, deferring quality analysis of selected studies (Arksey & O’Malley, 2005). The objective of this scoping review was to ascertain how occupational therapy outcomes are captured in the literature and to identify gaps that could lead to improved measures for occupational therapy services in hospice care. Our primary research question was, What are the characteristics of outcome measures in the published literature relevant to hospice occupational therapy services? Our secondary question was, What research designs facilitated measurement of outcomes in the context of hospice care?
Method
Our scoping review followed Arksey and O’Malley’s (2005) guidelines for analyzing and interpreting data. To address our research questions and guide the selection of relevant studies, we conferred with a research librarian on search terms, database selection, and inclusion and exclusion criteria. Our searches used the PubMed, CINAHL, MEDLINE, Scopus, Directory of Open Access Journals, Web of Science, OT Search, and Google Scholar databases. Search terms included hospice, palliative care, occupational therapy, rehabilitation, outcome measure, and assessment. Inclusion criteria were research studies with adults, written in English, published between January 1997 and September 2017, centered on hospice care, and investigated the efficacy of occupational therapy interventions with an outcome measure. Exclusion criteria were systematic reviews, studies with participants not at the end stages of a terminal illness, or intervention program reviews that did not distinguish occupational therapy outcomes from those of other disciplines. The wide date range was deemed necessary because of limited literature in this area of practice.
The first author initiated the literature search and excluded articles on the basis of title, abstract, and duplication. Both authors independently reviewed the full text of remaining articles and then debated until mutually agreeing on final selection. The first author collated data including author, year, study aim, population, methodology, outcome measures, interventions, results, and implications to identify findings of the review.
Results
The first author conducted the search in October 2017, resulting in 844 articles, and then reviewed the titles and abstracts and omitted duplications to narrow the pool to 49 articles. After both authors collaboratively agreed on the inclusion of 8 articles, further review revealed that 1 article was not a completed research study; this article was excluded, resulting in 7 included articles (Kasven-Gonzalez et al., 2010; Lee et al., 2005; Littlechild, 2016; Miller & Hopkinson, 2008; Norris, 1999; Panchmatia & Urch, 2014; Sakaguchi & Okamura, 2015). The first author identified findings based on analysis of the data collation and summary. Figure 1 details the article selection process, and Table 1 (at the end of this article) summarizes data on study participants, methods, and results. To address our research questions, we identified characteristics of the studies’ outcome measures and research designs relevant to occupational therapy hospice care services.
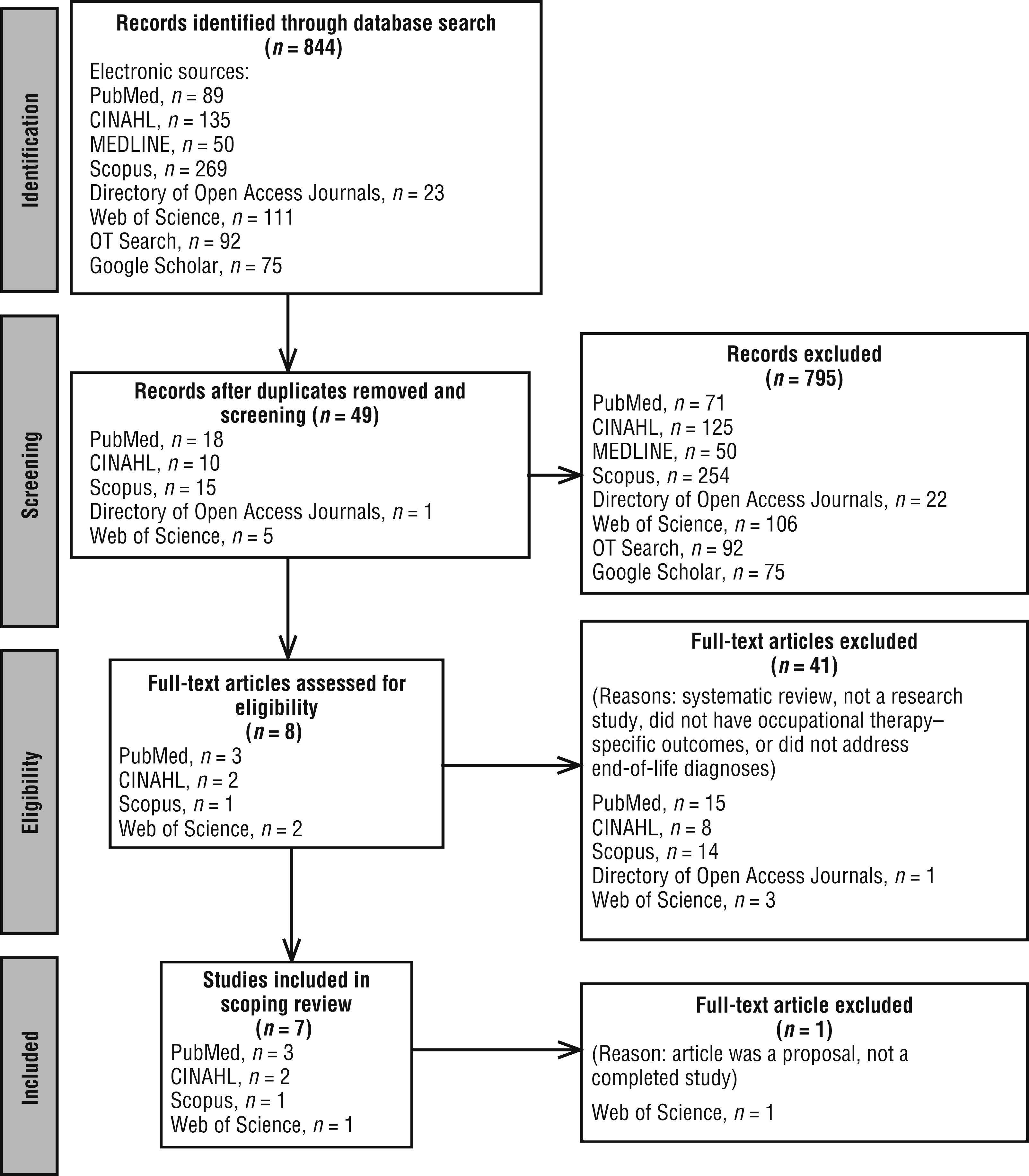
Flow diagram for inclusion and exclusion of peer-reviewed studies in the scoping review.
Evidence Table for Scoping Review on Occupational Therapy in End-of-Life Care
Note. ADLs = activities of daily living; COPM = Canadian Occupational Performance Measure; FACIT–Sp = Functional Assessment of Chronic Illness Therapy–Spiritual scale; GAS = goal attainment scaling; HADS = Hospital Anxiety and Depression Scale; ICF = International Classification of Functioning, Disability and Health; Max A = maximum assist; Min A = minimal assist; Mod A = moderate assist; OT = occupational therapy; PT = physical therapy; SESTC = Self-Efficacy Scale for Terminal Cancer; UB = upper body; VAS = visual analog scale.
Outcome Measures
Outcome measure characteristics in the included studies encompassed similarities and differences. Regarding similarities, two constructs were used in more than one study: (1) occupational performance (Kasven-Gonzalez et al., 2010; Lee et al., 2005; Norris, 1999; Panchmatia & Urch, 2014) and (2) negative symptoms, which included fatigue (Littlechild, 2016) and tension (Miller & Hopkinson, 2008). All outcome measures were ipsative, with “standardized procedures and . . . individualized so that the person compares himself or herself in the same domain across time” (Hinojosa & Kramer, 2014, p. 90). Researchers captured qualitative data with interviews, observations, and nonstandardized questionnaires (Kasven-Gonzalez et al., 2010; Littlechild, 2016; Panchmatia & Urch, 2014; Sakaguchi & Okamura, 2015).
Despite these similarities, outcome measures used varied across studies. No two studies used the same measure, and those used ranged from established measures to study-specific instruments and differed accordingly in psychometric strength. Three studies (Norris, 1999; Panchmatia & Urch, 2014; Sakaguchi & Okamura, 2015) used measures with established reliability and validity, including the Canadian Occupational Performance Measure (COPM; Cusick et al., 2007; Law et al., 2014), goal attainment scaling (Kiresuk & Sherman, 1968; Palisano, 1993; Steenbeek et al., 2010), the Functional Assessment of Chronic Illness Therapy–Spiritual scale (Cella et al., 1993; Noguchi et al., 2004), and the Hospital Anxiety and Depression Scale (Kugaya et al., 1998; Zigmond & Snaith, 1983). The remaining measures lacked established psychometric properties, including the Self-Efficacy Scale for Terminal Cancer (Hirai et al., 2002), study-specific instruments (Littlechild, 2016; Panchmatia & Urch, 2014), nonstandardized levels of assistance with self-care tasks (Kasven-Gonzalez et al., 2010; Lee et al., 2005), and a researcher-revised visual analog scale that substituted tension for pain (Miller & Hopkinson, 2008).
In the review of the outcome measures used, we noted an unexpected finding. Despite participants’ debility, the measures were able to detect positive outcomes with occupational therapy intervention. Five studies measured improved occupational performance and participant satisfaction with the following occupational therapy interventions: preparatory activities and family training (Kasven-Gonzalez et al., 2010); self-feeding (Lee et al., 2005); bathing, cleaning, and socializing (among others; Norris, 1999); transfers, activities of daily living (ADLs), instrumental activities of daily living (IADLs), and community mobility (Panchmatia & Urch, 2014); and life-review collage activities (Sakaguchi & Okamura, 2015). In the two studies addressing management of negative symptoms, occupational therapy interventions enabled participants to more successfully manage fatigue through lifestyle changes (Littlechild, 2016) and tension through relaxation exercises (Miller & Hopkinson, 2008). Although most participants reported satisfaction with occupational therapy outcomes (Kasven-Gonzalez et al., 2010; Panchmatia & Urch, 2014), some participants found overall decline to be distressing in the context of existential loss (Norris, 1999; Panchmatia & Urch, 2014). Because of the progressive nature of terminal illness, some occupational performance outcomes were not sustained throughout the study duration (Kasven-Gonzalez et al., 2010; Lee et al., 2005).
Research Designs
A salient element of end-of-life research is the probable decline of participants. The small samples in six selected studies reflect the difficulty of obtaining a large enough sample for a randomized controlled study (Kasven-Gonzalez et al., 2010; Lee et al., 2005; Littlechild, 2016; Miller & Hopkinson, 2008; Norris, 1999; Panchmatia & Urch, 2014; Sakaguchi & Okamura, 2015). Attrition in one study resulted from 2 participants’ deaths (Norris, 1999). To address participants’ limitations, the researchers used short interventions of two to four sessions (Littlechild, 2016; Miller & Hopkinson, 2008; Sakaguchi & Okamura, 2015). To address small sample sizes, most researchers used a noncontrolled, quasi-experimental, prospective design with pre–post testing, eliminating the need for a separate control group (Lee et al., 2005; Norris, 1999; Panchmatia & Urch, 2014; Sakaguchi & Okamura, 2015). One retrospective design enabled the researchers to gather a large sample without any participant burden (Miller & Hopkinson, 2008), although data collection was dependent on a priori outcome measure selection and reliable methodology. The variety of research designs was limited but addressed participants’ declining functional status over time.
Discussion
In reviewing the results, we identified key concepts and knowledge gaps that underscore the complexity of measuring outcomes with people living with incurable disease. Two key concepts involved ipsative measures and noncontrolled, quasi-experimental, prospective designs to accommodate end-of-life decline. Addressing knowledge gaps regarding an inappropriate focus on occupational performance, lack of established outcome measures, inattention to environmental factors, and limited use of end-of-life occupations can contribute to more effective interventions for and testing of occupational therapy outcomes in hospice care.
Key Concepts
All of the selected studies used ipsative measures. Ipsative measures can accommodate participants’ functional decline by measuring their outcomes against personal levels and self-report rather than norms of a general population (Cooper & Kite, 2015; Eva, 2006; Hinojosa & Kramer, 2014). Norm-referenced measures with preset levels of performance skills may not be sensitive enough to subtle, personal, and meaningful outcomes detected on an ipsative measure (Turner-Stokes, 2009) and would not be appropriate for the variable performance outcomes in an end-of-life context.
Four of the seven studies used a noncontrolled, quasi-experimental research design. Use of noncontrolled, quasi-experimental, prospective research designs is consistent with the literature on strategies to accommodate foreseen participant debility and decline. Recruiting participants who are terminally ill for randomized controlled trials can be difficult because of the severity of illness, the ethical concern of withholding intervention from a vulnerable group, and confounding variables (e.g., polypharmacy for pain control and comorbidities; Duffy, 2011; Yennurajalingam & Bruera, 2011). A noncontrolled, quasi-experimental, prospective research design allows for direct recording of data in the present to measure progress as it occurs over the course of treatment or intervention (Portney & Watkins, 2015), and this design can be used in hospice research when eligibility criteria, participant benefits, statistical analysis, and outcome measures are defined and appropriate; when the setting is controlled; and when burdens are minimized (Yennurajalingam & Bruera, 2011). Although retrospective designs can be cheaper and faster, the advantages of prospective studies are greater control in data collection and decreased memory bias (Portney & Watkins, 2015).
Knowledge Gaps
Inappropriate Focus on Occupational Performance.
Although the findings of some studies reflect positive outcomes in occupational performance with occupational therapy (Kasven-Gonzalez et al., 2010; Lee et al., 2005; Norris, 1999; Panchmatia & Urch, 2014), the outcome measures used failed to accommodate for participants’ eventual decline and to systematically measure end-of-life psychosocial needs. To positively frame the value of life and remaining time to live within the context of functional loss, Eva (2006) recommended focusing on occupational participation rather than on occupational performance. Participation is interaction in a life situation and does not necessarily require occupational performance skills (Koenig, 2014). Participation can involve observing an occupation, engaging in partial or adapted performance, or directing others’ performance (Koenig, 2014). A person who is terminally ill may still experience outcome gains and satisfaction with occupational participation even if functional performance declines. Occupational therapy practitioners and researchers may demonstrate greater functional and psychosocial outcomes and value by measuring changes in occupational participation rather than performance (American Occupational Therapy Association, 2016).
Lack of an Established Outcome Measure.
No widely accepted hospice occupational therapy outcome measure was identified in the seven selected studies. The COPM is often recommended for use in palliative rehabilitation given its client centeredness, assessment of occupations across multiple contexts, and ability to distinguish occupational therapy outcomes from those of other disciplines (Cooper & Kite, 2015; Eva, 2006). However, literature on use of the COPM with hospice populations is scant, and success with the COPM has been limited given participants’ deteriorating performance status (Cooper & Kite, 2015; Norris, 1999). Further study is needed of the validity of the COPM and other noninvasive, occupation-focused assessments in end-of-life care.
Inattention to the Environment.
All outcome measures used in the studies lacked attention to environmental effects on occupational engagement. As a hospice client functionally declines, the physical environment may pose barriers to performing daily routines and valued occupations; physical modifications may promote autonomy and sustained engagement (Cooper & Kite, 2015). In a cultural context or social environment in which dying is viewed as taboo, family and friends may alienate a person living with terminal illness by avoiding end-of-life conversations (Costa & Othero, 2012). Teaching the family communication strategies may help build relationships and support systems for the loved one (Chow, 2018). An environment with inaccessible hospice services may isolate clients and their families, whereas accessible services can enable them to manage negative symptoms, cope, and remain involved in their community (Chow, 2018). The environment thus can be highly influential in supporting a hospice client’s occupational engagement.
Only 1 selected study drew on the social environment to improve the participant’s overall outcomes by involving family in treatment sessions (Kasven-Gonzalez et al., 2010). The remaining 6 studies emphasized participant adaptation to the environment, instructing participants in compensatory strategies, providing rehabilitative interventions to maximize occupational performance (Lee et al., 2005; Littlechild, 2016; Miller & Hopkinson, 2008; Norris, 1999; Panchmatia & Urch, 2014), or using collage making as a communication tool (Sakaguchi & Okamura, 2015). Occupational therapy practitioners have expertise in evaluating and creating supportive occupational environments (American Occupational Therapy Association, 2016), yet this review suggests that the profession fails to capitalize on environmental resources to facilitate end-of-life occupational participation.
Limited Use of End-of-Life Occupations.
Among the selected studies, the range of occupational modalities was narrow. Occupation-based outcome measures primarily focused on self-care occupations (ADLs and IADLs). Four studies measured changes in self-care performance (Kasven-Gonzalez et al., 2010; Lee et al., 2005; Norris, 1999; Panchmatia & Urch, 2014). Articles that did not meet the inclusion criteria for this review recommended ADL assessments as hospice and palliative rehabilitation best practices, referring to the Barthel Index, Katz Index of Independence in Activities of Daily Living, Lawton Instrumental Activities of Daily Living Scale, FIM®, Palliative Performance Scale, and Karnofsky Performance Scale (Javier & Montagnini, 2011), as well as to the Modified Barthel Index and Eastern Cooperative Oncology Group Performance Status scale to screen cancer patients’ needs (Taylor & Currow, 2003).
Research has shown that people living with a terminal illness value being able to engage in daily self-care routines (Eriksson et al., 2016; Peoples et al., 2017); however, qualitative studies have identified that they also value occupations specific to the end of life, such as prioritizing relationships, reworking life to accommodate illness, engaging in legacy building and life review, finding closure, putting affairs in order, and making final arrangements (Hunter, 2008; Jacques & Hasselkus, 2004; Lala & Kinsella, 2011). Of the selected studies that specifically focused on end-of-life occupations, Sakaguchi and Okamura (2015) addressed life review with collage making, and Littlechild (2016) and Miller and Hopkinson (2008) investigated the effectiveness of life management skills to accommodate fatigue and tension, respectively, accentuating the physical and emotional impact of terminal illness.
The dying process not only affects physical functional performance but also shapes occupational needs and psychosocial responses. In the context of end-of-life care, occupational therapy practitioners and researchers seem to have limited the scope of practice to an “ADL–IADL box,” ignoring clients’ other occupational needs that are shaped by dying. Expanding the range of occupational interventions to address specific end-of-life occupations will increase clients’ opportunities for continued engagement throughout the lifespan.
Although the sample of articles meeting inclusion criteria was small, we noted key concepts and knowledge gaps that provide guidance for strategies to support occupational engagement among people living with a terminal disease. Occupational therapy practitioners and researchers may effectively test outcomes using an ipsative assessment and a noncontrolled, quasi-experimental, prospective design to accommodate functional decline. A focus on occupational participation rather than occupational performance will emphasize the value of and connection with life in the context of dying. Development of psychometrically strong outcome measures that assess environmental influences and occupational participation in a range of occupations, including end-of-life occupations, will enable occupational therapy practitioners and researchers to measure the efficacy of occupational therapy in hospice care and to support clients’ meaningful occupational participation during the end stage of life.
Limitations
The emotionally weighted context of dying and clients’ fragile health status at the end of life make clinical practice and research important yet logistically difficult. Even with the broad time frame of our search, the small number of research articles found limited our ability to consider a wider range of participants, settings, study designs, and outcome measures and generalize findings. Additional reviewers may have provided more diverse viewpoints and richer discourse in the review process.
Future Research
To support the unique occupational needs of people living with terminal illness, occupational therapy researchers need to develop and conduct psychometric testing of occupation-based outcome measures that assess occupational participation in a range of end-of-life occupations, the effect of the dying process on physical and psychosocial components, and the influence of environmental supports and that take into consideration clinical utility in daily practice. Generally accepted hospice occupational therapy outcome measures may effectively establish the efficacy of occupational therapy interventions at the end of life across a range of populations, settings, and illness groups. Further investigation is needed on the efficacy of traditional modalities (e.g., ADL retraining, rehabilitative techniques, environmental changes) and nontraditional modalities (e.g., life review, legacy building) in hospice care to support evidence-based practice. Such empirical research will foreseeably validate the efficacy of occupational therapy, justify utilization and funding, and increase access to occupation-based interventions for people who are at the end of life.
Implications for Occupational Therapy Practice
Findings from this scoping review have the following implications for occupational therapy practice:
To expand the influence of occupational therapy in end-of-life care and establish the therapeutic value of occupational participation throughout the lifespan regardless of a client’s level of functional performance, the profession needs to better educate students, practitioners, and researchers, as well as other end-of-life care stakeholders.
To support the occupational needs of people living with terminal illness, occupational therapy practitioners and researchers must broaden their view of end-of-life occupations beyond the “ADL–IADL box” by understanding how dying shapes occupational needs and by exploring clients’ roles and interests across multiple spheres and contexts.
To demonstrate the efficacy of occupational therapy in end-of-life care, practitioners and researchers need occupation-based ipsative outcome measures with psychometric strength and clinical utility that enable them to assess occupational participation, understand how the dying process affects physical and psychosocial components, consider environmental contexts, and explore specific end-of-life occupations.
Conclusion
We sought to characterize the outcome measures and associated research designs adopted in occupational therapy research with people in end-of-life care. In our scoping review of seven selected articles, we found that occupational therapy researchers frequently used prospective designs and occupation-based, ipsative outcome measures. The most common outcome measure construct was occupational performance. We found a range of outcome measures used across the selected studies but no generally accepted outcome measure relevant to hospice occupational therapy services.
In reflecting on our findings and the literature, we conclude that hospice occupational therapy can benefit from the development of outcome measures of occupational participation in end-of-life occupations. In addition to psychometric strength and clinical utility, such measures should provide an understanding of the dying process and the influence of the environment on occupational engagement. Focusing on occupational participation rather than occupational performance will replace the emphasis on functional performance decline with an emphasis on sustained involvement in meaningful roles and interests. As end-of-life care grows in demand and complexity, occupational therapy needs this type of outcome measure to establish the efficacy of occupation-based interventions and to support the unique occupational needs of people living with terminal illness.
Footnotes
Acknowledgment
We acknowledge Amanda Mims, reference librarian at Texas Woman’s University, for her expertise and guidance during the literature search process.
*
Indicates studies that were systematically reviewed for this article.