
Abstract
A child’s experiences are assembled through play, and the essential role of play in children’s lives has long been acknowledged (Isenberg & Quisenberry, 2002; Rigby & Huggins, 2003). Play is a fundamental building block for children’s skill acquisition and involves physical, mental, and emotional aspects (Parham, 2008). Engagement in play activities promotes physical development through active physical participation (e.g., building gross and fine motor skills and coordination; Smith, 2010; Wood & Attfield, 2005). Participation in play can also provide a safe atmosphere in which to develop social skills (e.g., learning role taking and sharing) and can facilitate emotional development (e.g., self-control, management of conflicting feelings, sensitivity to others; Gray, 2011; Rubin et al., 1983). Additionally, cognitive growth, including planning, attention skills, and language development, has been linked to play skills (Isenberg & Quisenberry, 2002; Rigby & Huggins, 2003).
The different functions that play serves have attracted the attention of researchers and professionals from a variety of fields. Although play has been examined from a variety of multidisciplinary perspectives and interests, these researchers have agreed that play is a key facilitator of children’s optimal growth across different life domains (e.g., Isenberg & Quisenberry, 2002). From the perspective of occupational therapy, as a profession concerned with clients’ occupations, play is considered to be children’s primary occupation. A strong positive relationship has been found between participation in occupation, particularly play, and children’s well-being (Hocking, 2009; Moore & Lynch, 2018).
Unfortunately, little attention has been paid to the need for play in children living with life-threatening and life-limiting conditions (LTC/LLC; Amery, 2016; Boucher et al., 2014). The number of children diagnosed with LTC/LLC worldwide is estimated to be more than 21 million (Connor et al., 2017). These children often experience loss or impairment that affects their participation in play, but the role and value of play may be even greater for vulnerable children with LTC/LLC than for healthy children (Amery, 2016; Boucher et al., 2014). In addition, prognoses are variable, and some children with LTC/LLC live into adulthood and thus will require the skills that play can enable them to attain (McNamara-Goodger & Feudtner, 2012; Shaw et al., 2015). Play is integral to the experience of childhood; children benefit from engagement in play (i.e., full experience of their childhood through interaction with peers) and from the outcome of this participation (i.e., development of later-life skills).
Regardless of children’s prognoses or medical conditions, they remain children and have the right to act and live as children, including to engage in play (Boucher et al., 2014; United Nations, 2006). Children with LTC/LLC need encouragement to continue playing as a way of preserving their childhood and facing their illnesses with the least trauma and best quality of life possible. However, little is known about play in this population. The aim of this scoping review was to examine empirical studies investigating play in children with LTC/LLC to explore their play characteristics and factors influencing their participation in play. Additionally, we sought to identify related issues that influence these children’s participation in play. By so doing, we add to the body of literature related to understanding play in children living with LTC/LLC.
Method
Little is known about play as part of the daily life of children with LTC/LLC. Therefore, we conducted a scoping review to map the available literature broadly and comprehensively (Arksey & O’Malley, 2005; Armstrong et al., 2011). The review was conducted and reported in accordance with Aveyard (2014) and Peters et al. (2015).
We followed a strict protocol to promote the reliability of the findings (Aveyard, 2014; Cronin et al., 2008). We identified, critically appraised, and synthesized relevant studies from a range of professional contexts—including health, palliative care, social services, sociology, and design and architecture—to gain a comprehensive understanding of existing research on play in children living with LTC/LLC (Cronin et al., 2008; Davis et al., 2009; Peters et al., 2015; Thomas & Harden, 2008).
Data Sources and Search Strategy
To extract the most relevant empirical literature, we conducted comprehensive searches in multiple electronic databases (AMED, CINAHL, PsycINFO, MEDLINE, Embase, Web of Science, Scopus, ASSIA, and Cochrane Library), a gray literature search, manual searches of relevant journals (i.e., Journal of Social Work in End-of-Life and Palliative Care, International Journal of Palliative Nursing, Palliative Medicine, American Journal of Hospice and Palliative Medicine, End of Life Journal, BMJ Supportive and Palliative Care, Journal of Child Health Care, European Journal of Palliative Care, Health Environments Research and Design Journal, Journal of Healthcare Interior Design, Design Studies, and Architectural Engineering and Design Management), and reference lists of identified articles. The search was limited to documents published between 1990 and mid-October 2017. Although the time range could be considered long, it was selected because of the limited number of available studies.
Only literature published in Arabic or English was searched to limit the possibility of mistranslation from languages in which the authors are not fluent. The main search terms children, play, and LTC/LLC were selected from the overall research topic and used in combination with other key words and subject headings and Boolean operators (AND, OR) and search symbols to ensure that we considered as many relevant studies as possible (Table 1).
Search Terms Used in the Scoping Review
Note. LTC/LLC = life-threatening and life-limiting conditions.
Selection Criteria
To be included in the review, studies had to examine play in children with LTC/LLC, the authors had to clearly describe the results for the sample group, and the articles had to mention LTC/LLC, palliative or end-of-life care, or long-term complex health conditions. The studies also had to include children ages 5 to 11 yr because of the importance of daily play in middle childhood. No restriction was imposed on setting (e.g., home, health care) or country of publication. Although cultural influences on play have been acknowledged, this field is underresearched, so we included studies irrespective of country of origin.
We excluded nonresearch literature such as anecdotal views or opinions because of potential limitations in the authors’ expectations or observations. In addition, we excluded studies examining the effectiveness of play, such as play with therapeutic intent (e.g., sand play, pretend play) or play as a distraction (e.g., in a waiting area or emergency department), and studies focusing on staff members’ or parents’ satisfaction with services or facilities. These exclusion criteria were based on our aim of reviewing the characteristics of children’s play.
Study Selection
Our search yielded numerous results, perhaps because of the broad search terms used. However, it was important to consider all relevant possibilities. To determine the potential relevance of the search results, we initially screened titles and abstracts. We then reviewed the full text of documents that appeared relevant to decide whether they met the inclusion and exclusion criteria.
After removal of duplicates, 3,635 potential studies remained. Screening by title and abstract resulted in 238 articles, which we fully reviewed using the inclusion and exclusion criteria. Studies were excluded primarily because they used nonempirical data, researched the therapeutic effectiveness of play, evaluated the effects of therapeutic camping programs on children’s conditions, or targeted other age groups (e.g., adolescents). This process resulted in 13 relevant articles being included in this review (Figure 1).
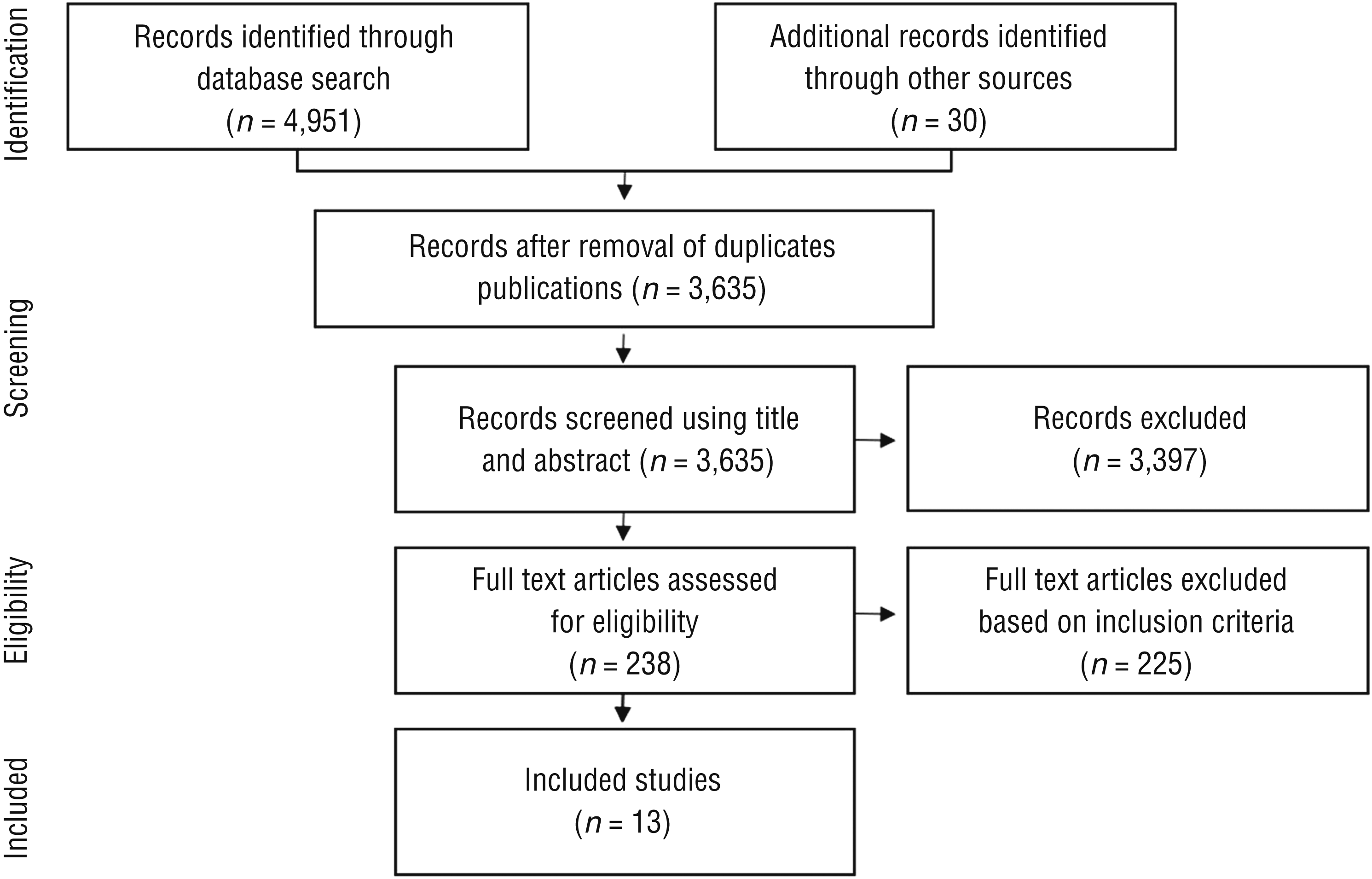
Flow diagram for the inclusion and exclusion process of the scoping review.
Data Extraction and Appraisal
We used the Critical Appraisal Skills Programme (2018) and the Joanna Briggs Institute (2017a, 2017b) Critical Appraisal Tools to assess and appraise quality of the evidence (Thomas & Harden, 2008). This was for the purpose of identifying what the papers found and the strengths of these findings. These guidelines were applied on the basis of study design; included studies had qualitative and mixed methods (qualitative and quantitative) designs. We summarized the 13 articles in a table detailing their key characteristics (see Table 2, at the end of this article).
Evidence Table for the Scoping Review on Play in Children With Life-Threatening and Life-Limiting Conditions
Data Analysis
We used thematic analysis and synthesis to derive the main issues addressed in the empirical literature in relation to play in children with LTC/LLC. We first generated free codes for related areas and then developed descriptive themes to assist us in integrating the studies’ findings through a logical flow in terms of continuity and consistency to arrive at the review findings (Cronin et al., 2008; Thomas & Harden, 2008).
Results
Few studies have explored play in children with LTC/LLC. In fact, only three studies focused on play; for the other studies, examining play was not the main purpose of the research. Lima and Santos (2015) explored children’s perspectives of the influence of play in the care process during hospitalization, and Silva and Cabral (2014) and Graham et al. (2015) investigated the impact of children’s health conditions on dimensions of their play. Six studies that explored children’s experiences receiving care addressed play in their findings to a lesser extent (Aldiss et al., 2009; Ångström-Brännström et al., 2013; Gibson et al., 2010; Kirk & Pritchard, 2012; Mufti et al., 2015; Rabiee et al., 2005). Some aspects of play were addressed in another four studies whose main purpose was to explore the supportive hospital environment (Lambert et al., 2014a, 2014b; van der Riet et al., 2014; Verschoren et al., 2015). We classified the findings into three main themes: continuity of play, influence of health conditions on play, and play opportunities.
Continuity of Play
Several studies found that children with LTC/LLC and their parents hoped that the children would be able to continue their normal everyday lives, including play (Aldiss et al., 2009; Rabiee et al., 2005; Verschoren et al., 2015). Children reported enjoying play (Aldiss et al., 2009; Ångström-Brännström et al., 2013; Graham et al., 2015); play provided a sense of normality and added fun and happiness to their lives (Aldiss et al., 2009; Graham et al., 2015; Lima & Santos, 2015). Children gained comfort at home from play and everyday activities (e.g., playing with Legos, playing video games, coloring, reading) and missed these activities while hospitalized (Ångström-Brännström et al., 2013; Gibson et al., 2010; Lambert et al., 2014b). Having the opportunity to play the games they had at home when hospitalized made their stay more enjoyable (Aldiss et al., 2009; Gibson et al., 2010; Lima & Santos, 2015).
Often, childhood activities are perceived as “normal” or as doing normal childhood things. Although children with LTC/LLC may aspire to such normality, achieving it can be challenging.
Influence of Health Conditions on Play
Lima and Santos (2015) found that children with cancer mainly used electronic devices as entertainment because they could easily play with them in bed; for many children, staying in bed is an impact of LTC/LLC. Gibson et al. (2010) and Silva and Cabral (2014) found that cancer and its treatment restricted children’s active play (e.g., riding a bike) and left them weak and with limited physical ability to participate in play (e.g., because of balance difficulties or attachment to an infusion).
Thus, illness and treatment can place limitations on the play activities of children with LTC/LLC (Aldiss et al., 2009; Graham et al., 2015; Mufti et al., 2015). In addition, children may develop more cautious lifestyles as they follow the relevant medical precautions.
Play Opportunities
The limited data in the literature on play in children with LTC/LLC revealed several aspects of play opportunities that influence their participation in play. These aspects include play equipment, play spaces, and playmates.
Play Equipment.
Although toys are a necessary feature of the pediatric hospital environment, children participating in several studies complained about the limited availability of toys, the need for more age- and gender-appropriate activities (Aldiss et al., 2009; Gibson et al., 2010; Kirk & Pritchard, 2012; Lambert et al., 2014a, 2014b; Lima & Santos, 2015), and the need to maintain and replace play equipment (van der Riet et al., 2014). Children viewed storage of play equipment on high shelves or in locked cabinets negatively (Gibson et al., 2010; Kirk & Pritchard, 2012).
Play Spaces.
For many children, the playroom was one of the most important features of the hospital, in addition to toys (Aldiss et al., 2009; Gibson et al., 2010). Children reported that being in the hospital was unbearable because it restricted their play (e.g., not being able to play with Legos) and took them away from their daily routines (Ångström-Brännström et al., 2013; Lima & Santos, 2015). Although playrooms with a wide range of activities were available in the health care facilities in all of the studies, children reported that these rooms were usually closed after working hours and on weekends (Aldiss et al., 2009; Gibson et al., 2010; Lambert et al., 2014a, 2014b; Lima & Santos, 2015; Verschoren et al., 2015). The use of the play areas was also limited because of inaccessibility or the children’s physical impairments, their need to follow precautions, medical intervention or isolation (Gibson et al., 2010; Lambert et al., 2014a, 2014b; Mufti et al., 2015).
Children expressed a desire for more interesting spaces (e.g., fitness rooms, swimming pools, cinemas; Aldiss et al., 2009; Lambert et al., 2014b; Verschoren et al., 2015). Additionally, children referred to the bathroom as a place where enjoyable play took place; in particular, bathing was reported by some as the most common playtime, and the availability of bath-specific play toys was viewed positively (Graham et al., 2015; Lambert et al., 2014b).
Children emphasized the importance of having shared places to interact with other children. The corridors and waiting areas were mentioned as places where children could engage in pleasant social interaction with others (Verschoren et al., 2015). It has been suggested that playrooms be integrated with the whole hospital or located in the center of the facility (Lambert et al., 2014a, 2014b) and that relational spaces such as gardens be available (Lambert et al., 2014a; van der Riet et al., 2014; Verschoren et al., 2015).
Playmates.
Children enjoyed talking about their friendships (Gibson et al., 2010; Kirk & Pritchard, 2012; Rabiee et al., 2005). Kirk and Pritchard (2012) found that the majority of participants liked school because the presence of more children meant more opportunities for play. This finding is in accord with the observations of van der Riet et al. (2014), who found that a garden at their hospital expanded the children’s experience of social interaction as a context for play. Notably, the presence of siblings allowed children opportunities for play and laughter (Ångström-Brännström et al., 2013).
The social environment of children’s play also includes the cultural norms and support systems in the wider community. Mufti et al. (2015) demonstrated that children were able to recognize the discrimination in their community that resulted from their illness and the influence of this discrimination on losing friends. Being labeled an unwell child in some communities meant that other children avoided making contact, negatively influencing the child’s self-image. The child’s view of self as disabled, particularly because of the limited ability to move during play, led to isolation.
Children’s limited capabilities were found to disrupt their play with grown-ups as well. Children reported enjoying play with parents, nurses, and play specialists (Gibson et al., 2010; Graham et al., 2015), but the time and energy required from those adults to facilitate play placed a burden on them that resulted in limited opportunities.
Discussion
Children with LTC/LLC deserve to receive optimal care filled with opportunities for meaningful experiences and the best quality of life possible throughout their illness and treatment (Boucher et al., 2014). LTC/LLC may limit the ability of children to fully experience their childhood. Health care professionals have a duty to facilitate their access to experiences that are, as much as possible, equitable to those of their peers in their communities (Randall, 2016). The limited research on this topic includes 13 studies that met our eligibility criteria, and our review of these studies identified three key concepts regarding play in children with LTC/LLC: (1) the significance of continuity of participation in usual play and activities, (2) the influence of health conditions challenging children’s play, and (3) social and physical factors shaping children’s play and determining the opportunities available to them.
These studies highlighted the importance of children continuing their everyday lives as “normally” as possible during hospitalization. Play is integral to a sense of normality and provides fun and happiness. Both the children and their caregivers acknowledged the essential role of play. Ito et al. (2015) found that ongoing access to typical activities and relationships contributed to a good death for children with cancer. Practitioners can assist children in maintaining their preexisting roles by providing opportunities for play consistent with their preferences, conditions, and challenges, underlining the need to understand the types of and reasons for play among children with LTC/LLC. Most of the play activities that participants mentioned being unable to take part in while hospitalized may be easily adapted to hospital settings (e.g., playing with Legos, reading). More exploration is needed to discover the factors that hinder children’s participation in their preferred play.
Another factor influencing the continuity of children’s participation in play was the limited availability of play materials and the need for more age- and gender-appropriate toys and activities. However, this finding was not elaborated in the reviewed literature with clear examples and descriptions. Lambert et al. (2014a), for instance, gave vague examples of gender-appropriate play, stating simply that the girls played different games than the boys on computers. The authors added that the available toys were only for younger children. Another study followed children from birth until late adolescence (Rabiee et al., 2005) but did not segregate the perspectives of the different age groups or acknowledge the type of reporter. This lack of clarity draws attention to a gap in our understanding of children’s actual needs.
The play needs of children vary considerably in terms of preferences and developmental needs (Corsaro, 2015). However, play spaces, as perceived by the children in these studies, were not limited to playrooms but were wherever the children could enjoy themselves and have fun. The concept of the built (i.e., physical) environment’s influence, indoors or outdoors, was not considered in any of the reviewed studies, illustrating the need to further investigate the impact of the built environment on play. Some children experienced difficulties using the play areas, but it was not clear whether the areas had been designed so that children with various abilities could enjoy and use them and what factors may have limited the use of these spaces. Many of the studies found that restrictions and limitations on use of the play areas affected social play, providing evidence that the direct influence of the conditions for play indirectly influenced relationships with other children.
Strengths and Limitations of the Scoping Review
Because of the nature of the topic, the reviewed studies were qualitative in design, except for one that used a mixed methods approach. These studies contribute to an understanding of play in children with LTC/LLC and the value of exploring this topic (Daly et al., 2007).
Although we used a systematic approach to collecting articles, this study is not considered a systematic review because of the lack of predefined, precise research questions resulting from the limited research in this area. Thus, limitations include a risk of confirmation bias (Green et al., 2006) and a lack of extensive data synthesis (Armstrong et al., 2011). Moreover, searching only journal articles written in English and Arabic may have resulted in the exclusion of other relevant studies.
Although children are generally underrepresented in research, the majority of the reviewed studies included the children’s perspectives. Studies of children often focus on caregivers’ proxy views of children’s experiences, likely because of ethical issues, ignorance, or a belief that children are less cognitively able to communicate (Scott, 2008). This review included only studies with participants who were children ages 5–11 yr or caregivers representing their children. Several reviewed studies also included adolescents and their parents (Graham et al., 2015; Kirk & Pritchard, 2012), nurses (van der Riet et al., 2014), or relatives (e.g., parents, siblings, grandparents, aunts; Silva & Cabral, 2014), some of whom may not have been able to provide a complete picture of the child’s actual needs or views. Although these participants may have offered a diversity of views, their views were not always clearly segregated in the findings.
Most of the studies were of good or average quality, which suggests reasonable quality overall. Almost all of the studies set a clear aim and used an appropriate design and method to answer the research question, although more details regarding the participants and the methods and modes of analysis would have been beneficial. In addition, their process of reaching findings was not always clear; in particular, reflexivity and other factors in the researchers’ role were not transparent in most of the studies. These shortcomings contributed to the average quality appraisal. Nevertheless, these studies provide important implications that may help inform future practice and research.
The findings that emerged from this review should be considered with caution, especially given that participants in half of the studies were limited to children with cancer. Children experiencing other physical limitations were not well covered by this review; either they were excluded or their inclusion was not made clear in the studies reviewed. These sampling issues underline a crucial gap in research with children with complex conditions. Real difficulties exist in identifying children with LTC/LLC, probably because of the difficulties inherent in their prognoses (Fraser et al., 2012; McNamara-Goodger & Feudtner, 2012). Moreover, because most of the studies did not directly focus on play, they provide only limited evidence regarding the challenges faced by children with LTC/LLC with regard to play and the opportunities available to them. This shortcoming in the literature may reflect a predominance of the medical approach and the future-oriented perspective of adults, in addition to a lack of awareness of the major role of play in both being and becoming. As a consequence, immediate attention is required from occupational therapy practitioners and researchers to find alternative ways to enhance these children’s participation in play as their primary childhood occupation and to enable the best possible quality of life, whether that life is short or extends into adulthood.
Implications for Occupational Therapy Practice
The findings from this scoping review have the following implications for occupational therapy practice:
The nature of LTC/LLC and their effects on children’s abilities and functioning negatively influence participation in the childhood occupation of play.
The continuity of children’s participation in their routines while hospitalized, and particularly of their preferred play modes and items, is important to their well-being.
Cultural, social, and physical environmental factors shape children’s play.
Promoting children’s participation in play can be achieved through recognizing and targeting the strength of environmental influences, facilitating supports, and limiting barriers.
Conclusion
It is a child’s right to play and experience childhood. However, many children with health problems experience play deprivation. The studies we reviewed on play in children with LTC/LLC demonstrated that play is influenced by health conditions and that play opportunities can be enhanced by providing a variety of play tools, accessible areas for play to facilitate social interactions, and age- and gender-appropriate play opportunities. Continuity in play was found to have a positive impact on well-being.
In general, the topic of play in children with LTC/LLC is underrepresented in the literature, and our review provides valuable information on the limitations of existing studies. Good-quality studies are needed that explore children’s everyday routines, including play, particularly in children with nononcological complex conditions. More insight is needed on the play characteristics and spaces used by these children. Awareness of the barriers and enablers children encounter during play can support the design of optimal play environments for children with different capabilities. Support for participation in play by children with LTC/LLC can allow them to achieve a better life experience, to live their childhood as fully as possible, and, if required, to prepare for a good death.
Footnotes
*
Indicates studies that were systematically reviewed for this article.