
Abstract
Osteoarthritis (OA) is one of the most common skeletal muscle diseases (Bijlsma et al., 2011). It is characterized by the presence of pain in the joints, followed by functional limitations (Fernandes et al., 2010) that frequently occur in the hands. According to some studies, hand OA is associated with OA in other joints, such as the hips or knees (Dziedzic et al., 2013; Gabay & Gabay, 2013; Maheu & Berenbaum, 2009; Zhang et al., 2009). Moreover, OA occurs more frequently among women, and the prevalence of hand OA increases with age (Neogi & Zhang, 2013; Zhang et al., 2009).
Hand OA is treated through a combination of nonpharmacological and pharmacological treatments, and treatment is adapted according to the client’s wishes and expectations, pain level, and functional restrictions (Zhang et al., 2007). Analgesics and nonsteroidal anti-inflammatories for the alleviation of symptoms, orthoses for the carpometacarpal (CMC) joint, client education, and hand exercises have proved to be effective in treating hand OA (Kjeken et al., 2011; Kloppenburg et al., 2015; Zhang et al., 2007).
Rehabilitation texts have discussed the use of orthoses to control pain and joint inflammation of the proximal interphalangeal (PIP) or distal interphalangeal (DIP) joints (Egan & Brousseau, 2007; Fess et al., 2004). A literature review revealed two studies describing the use of orthoses for OA in the DIP joint; one was a trial without a control group and another was a trial with no randomization to condition (Ikeda et al., 2010; Watt et al., 2014). Customized orthoses that are fabricated on demand for OA of the interphalangeal (IP) joint have not been very well studied, and little scientific evidence exists for the use of orthoses in the treatment of OA in the CMC joint (Egan & Brousseau, 2007). To address this gap, we conducted a randomized controlled trial (RCT) of treatment with orthoses for pain in the PIP and DIP joints of the hand with symptomatic OA.
Method
Study Design and Participants
We conducted an RCT with a masked assessor and an intention-to-treat analysis. Seventy-seven adult participants with hand OA were recruited from the outpatient clinic of the rheumatology department. Inclusion criteria were women ages 40 yr and older with a diagnosis of hand OA according to American College of Rheumatology criteria (Altman et al., 1990) with symptoms in the second or third finger, or both, of the dominant hand (these fingers were the most symptomatic), with pain rated between 3 and 8 cm on a 10-cm numerical rating scale (NRS), who had been undergoing stable pharmacological treatment for the preceding 3 wk. Exclusion criteria were secondary hand OA, neurological and skeletal muscle disease that could compromise the upper limb, and cognitive deficit that could obstruct the comprehension of assessment instruments.
Participants who met the inclusion criteria were scheduled for interviews and evaluations. Before study enrollment, all participants gave written informed consent to participate in accordance with the Declaration of Helsinki (World Medical Association, 1999). The study was carried out in the outpatient clinic of the Universidade Federal de São Paulo. The study was approved by the institutional ethics committee, and the article was prepared according to the Consolidated Standards of Reporting Trials (CONSORT) statement (Moher et al., 2010).
Computer-based randomization was used to allocate the clients into two groups: the intervention group (IG) and the control group (CG). Group allocation was initially concealed in an opaque, sealed envelope, which was opened by each consecutive client to reveal her group assignment at the time of study recruitment.
Procedure
A custom finger gutter thermoplastic orthosis was fabricated by a senior hand therapist (Paula Gabriel Silva) by molding the volar side of the finger and aligning the DIP and PIP joints with neutral positioning. Considering the finger’s anatomy and the limit of the metacarpophalangeal articulation, adjustments were made to the splint’s dorsal side (Figure 1) for each client’s intervention joint at the baseline visit and following assessments. Clients were shown how to fit the orthosis and were asked to wear it every night for 6 mo. They were also asked not to alter their pain relief medication and other hand therapies during the study, if possible, and any changes were documented at each visit. The clients in the CG did not use an orthosis during the study period. No placebo was included because there is no accepted placebo or sham for the use of orthoses.
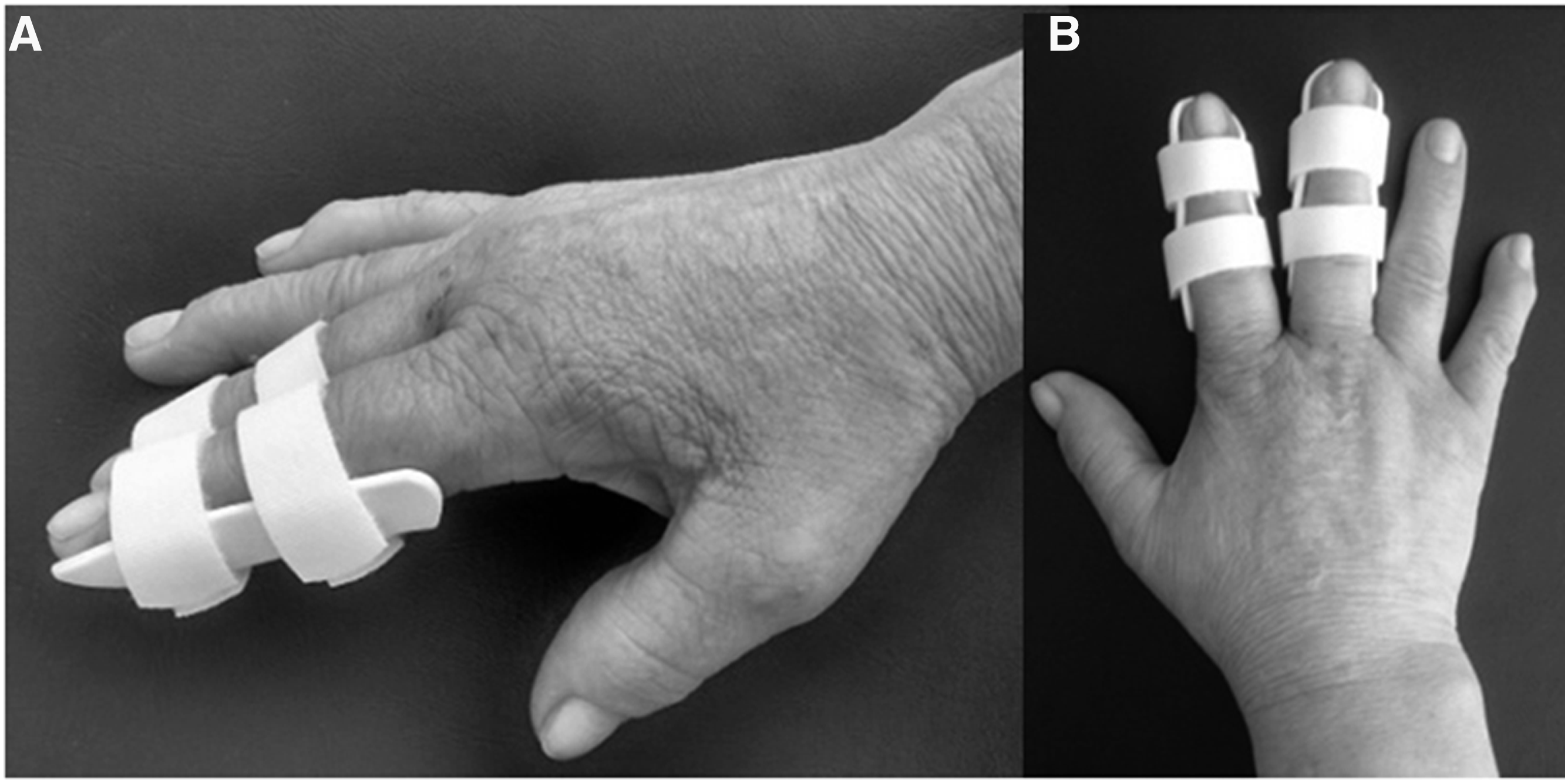
Custom finger gutter thermoplastic orthosis for the second and third fingers: (A) side view; (B) dorsal view.
All participants (in both the IG and the CG) participated in an educational program on hand OA that was held in the days after the evaluations. This client education involved three 40-min sessions that included a lecture by the trial researcher (Silva) that provided information about the disease, its symptoms, medical treatments, joint protection, and energy conservation.
Outcome Measures
Primary and secondary outcome measures were recorded at baseline (T0) and 45 (T45), 90 (T90), and 180 (T180) days after inclusion in the study by another senior hand therapist (Fabiana de Carvalho Silva), who was masked to participants’ group allocation and custom gutter orthosis.
Primary Outcome Measure
Pain was measured on the 11-point NRS (Ferraz et al., 1990), which ranged from 0 cm (no pain) to 10 cm (unbearable pain) and was recorded for the second and third fingers of the dominant hand when resting and during activity (IP joints in flexing and extending functional movement, respectively) in the past 24 hr.
Secondary Outcome Measures
The Australian/Canadian Osteoarthritis Hand Index (AUSCAN) was used to evaluate the client’s knowledge about pain (Bellamy et al., 2002). The AUSCAN consists of 15 questions divided among three categories: pain, stiffness, and physical function. Scores range from 0 to 60; the higher the score is, the worse the function.
The Cochin Hand Functional Scale (Chiari et al., 2011; Poiraudeau et al., 1987, 2001) was used to evaluate the client’s level of functional incapacity. It consists of 18 questions divided among five categories related to common daily activities that involve perceived function: activity in the kitchen, dressing, hygiene, activity at work, and other. Scores range from 0 to 90; the higher the score is, the worse the function.
The Moberg Pick Up Test (MPUT), modified by Dellon, is a manual performance test of object recognition through the pinch function; it is composed of 10 metallic objects. Clients need to pick up, hold, and manipulate the objects to recognize them. The test was performed with eyes open and then blindfolded, and the time taken to recognize the objects was recorded (Loss et al., 2012; Stamm et al., 2003, 2007).
Grip strength was assessed by means of a Jamar grip dynamometer (JLW Instruments, Chicago, IL). The dynamometer was calibrated, and pinch strength was evaluated through tip-to-tip, tripod, and lateral pinches using the dynamometer’s pinch gauge. Three measurements were recorded using a standardized method, and the average was reported (Caporrino et al., 1998; de Araújo et al., 2002).
Radiological classification for hand OA was performed according to the criteria proposed by Kellgren and Lawrence (1957), and the presence of erosion was assessed according to the scoring method of Verbruggen and Veys (1996). The patient informed the evaluator about any use of medication.
Statistical Analyses
To determine sample size, we performed a power calculation using repeated-measures analysis of variance (ANOVA) for two groups and four measurement times. This calculation yielded a target sample size of 22 participants needed to detect a difference of 2 cm on the NRS for average pain, with 90% power to detect a statistically significant difference at the 5% level. Considering a possible loss of 20% of participants, we determined that each group should consist of 26 clients.
Statistical analyses were performed using IBM SPSS Statistics for Windows (Version 19; IBM Corp., Armonk, NY). Descriptive statistics are presented in Table 1 as means and standard deviations. The persistent initial variables for both groups were compared using Student’s t test for variables with normal distribution and the Mann–Whitney U test for variables with nonnormal distribution. The categorical variables were evaluated with the χ2 test. To evaluate the response to the intervention, we used repeated-measures ANOVAs to evaluate the variables that persisted in the between-groups and within-group analyses over time. Pearson correlations were used to correlate the pain variables with the other variables. We selected those variables with significant correlations and performed a multivariate regression to predict improvement in pain while at rest and during activity. An intention-to-treat analysis was carried out. If a client could not attend an evaluation (T45, T90, T180), data from the previous evaluation were used. The level of significance was set at p < .05.
Demographic and Clinical Characteristics at Baseline
Note. AUSCAN = Australian/Canadian Osteoarthritis Hand Index; Cochin = Cochin Hand Functional Scale; kgf = kilogram-force; M = mean; MPUT = Moberg Pick Up Test; NRS = numerical rating scale in centimeters; SD = standard deviation.
p < .05.
Results
Of 77 potential participants, 52 were eligible for the study and were randomized to the IG (n = 26) or the CG (n = 26; Appendix A). The participants had similar results at baseline (Table 1), except for grip strength, tip-to-tip pinch, and lateral pinch strength, for which the IG had lower average values. One IG participant did not show up at T180 for personal reasons, but data for all participants were analyzed.
We evaluated each participant’s most symptomatic finger during activity. Both the IG and the CG showed similar proportions of more symptomatic second and third fingers (p = .760). Pain in the second finger (n = 37; 71.2%) was more prevalent than pain in the third finger (n = 15; 28.8%); 30.1% displayed erosive OA, but this greater joint involvement did not influence pain variation at rest (p = .836) and during activity (p = .371).
Regarding pain, the IG reported lower NRS scores for pain at rest and during activity (p = .006 and p ≤ .001, respectively; Table 2). The within-group analysis showed a significant reduction in pain during activity in the CG between T0 and T90 (p = .010), but this reduction was not maintained throughout the evaluation period. In the IG, mean NRS score for pain was reduced by 2.1 cm at rest and by 4.3 cm during activity, and in the CG, the reductions were 0.1 cm and 0.7 cm, respectively.
Between-Groups Comparison of Mean NRS, Medication, Grip and Pinch Strength, AUSCAN, COCHIN, and MPUT Scores Over Time
Note. ANOVA = analysis of variance for repeated measures; AUSCAN = Australian/Canadian Osteoarthritis Hand Index; Cochin = Cochin Hand Functional Scale; kgf = kilogram-force; MPUT = Moberg Pick Up Test; NA = not applicable; NRS = numerical rating scale in centimeters; T0 = baseline; T45 = 45-day evaluation; T90 = 90-day evaluation; T180 = 180-day evaluation.
Intragroup.
p < .05.
The results for both groups were similar over time; we found no statistically significant within-group and between-groups differences for medication, pinch strength (tip-to-tip, tripod, and lateral), AUSCAN stiffness, and Cochin kitchen activities and office activities (see Table 2). Some variables showed statistically significant differences in the intragroup evaluation but did not change over time: grip strength, Cochin hygiene, and MPUT performed with the dominant hand with eyes open and with eyes closed (see Table 2). The results for the IG differed from those of the CG over time, with lower within-group and between-groups averages for AUSCAN pain, physical function, and total score and Cochin dressing, other, and total score (Table 2).
Reduction in pain during activity showed a moderate and negative correlation with Cochin scores for kitchen activities (r = −.522, p = .006) and other ( = −.547, p = .004) and a weak and negative correlation with total score (r = −.388, p = .050). Variables that predicted a reduction in pain at rest were Cochin scores for work activities (r = .410, p = .038) and the absence of Bouchard’s node on the third finger (p = .022). The absence of Bouchard’s node on the third finger (p = .014) was predictive of a reduction in pain during finger activity.
We observed a statistically significant reduction in orthosis use between T45 and T180. The average at T45 was 7 hr, 52 min; at T180, it was 6 hr, 41 min. Twelve clients needed adjustments to their orthoses (3 at T45, 7 at T90, and 2 at T180); these adjustments were performed on the day of the evaluation without the need for a return visit. Table 3 shows the effect sizes and 95% confidence intervals for all parameters that were significantly different between the groups over time (as determined through ANOVA).
Effect Sizes and 95% Confidence Intervals for Parameters That Were Significantly Different Between Groups With ANOVA
Note. Cohen’s d interpretation: small, 0.20; medium, 0.50; and large, 0.80. ANOVA = analysis of variance; AUSCAN = Australian/Canadian Osteoarthritis Hand Index; CI = confidence interval; NRS = numerical rating scale in centimeters.
Discussion
This study is the first to address the treatment of symptomatic hand OA in the PIP and DIP joints with nighttime orthoses. Studies such as those of Ikeda et al. (2010) and Watt et al. (2014) have previously examined the effect of orthoses for DIP joints affected by OA. Pain is necessary for the diagnosis of hand OA, and some studies have reported that a 2- or 3-cm variation on the NRS is required to show a clinically significant difference in pain (Zhang et al., 2009).
In our study, the reduction in pain from T0 to T180 was greater in the IG than in the CG. This result corroborates the research of Ikeda et al. (2010) and Watt et al. (2014). In the Ikeda et al. study, pain was reduced by 39 mm over 4–10 mo; in the Watt et al. study, a difference of 1.5 cm in 3 mo and 2 cm in 6 mo was observed for the fingers with orthoses. The results of these studies suggest that the short-term use of a nighttime orthosis can reduce pain in hand OA.
In our RCT and in the studies by Ikeda et al. (2010) and Watt et al. (2014), the average initial pain rating indicated moderate pain; however, it is known that level of pain is sometimes not linked to the duration of disease or progression. We noticed a variation among the three studies: In our study, the highest average disease duration was 7.14 yr; in Ikeda et al., it was 2 mo–2 yr; and in Watt et al., it was 6.3 yr. Longer disease duration does not necessarily imply greater pain; the participants in these three studies characterized their pain as having the same intensity.
Our evaluation indicated that in both groups, the second finger was the most symptomatic (71.2%), then the third finger (28.8%). This finding corroborates data from other studies showing a higher degree of pain in the second finger of the hand with OA (Altman et al., 1990). In the analysis of secondary outcomes, we found a between-groups difference in favor of the IG regarding the AUSCAN and Cochin assessments, with a reduction in total score. These differences occurred over the long term (T180). The results for grip and pinch strength and the MPUT were similar between the groups over time, and the reduction in pain did not differ among these measures. Reduction in pain showed a negative and low correlation with the total score and moderate correlation with the score for kitchen and other activities. Low scores on Cochin office activity and the absence of Bouchard’s node in the third finger predicted good response to orthosis treatment.
Our findings corroborate the results of Zhang et al. (2002). Their study compared people with symptoms of hand OA with people showing no symptoms and observed that those with the disease presented with a reduction of 10% of maximum grip strength and had difficulties with writing and handling small objects. They suggested that symptomatic hand OA obstructs manual function, especially fine motor control. The use of an orthosis may contribute to the reduction in pain and lead to an improvement in the performance of hand activities, which we observed in the Cochin score for the IG.
The finding that the presence of Bouchard’s node predicted a poorer result for pain reduction with orthosis use is clinically relevant; we believe that early intervention is needed to control PIP joint inflammation and alleviate clients’ symptoms. The immobilization provided by the orthosis could have decreased mechanical stress, possibly reducing the inflammatory process. The custom orthoses allowed for alignment and stabilization of the IP joint, and we believe custom orthoses should be recommended for clients with hand OA and endorse their use at night to avoid interference in daily activities. During this RCT, we lost no clients as a result of harmful or collateral effects such as allergy to the material, dissatisfaction with the orthoses, or worsening of the clinical condition; moreover, all clients adhered to the treatment.
The participants kept a diary to record the duration of orthosis use, which they adjusted daily according to their symptoms. We detected a statistically significant reduction in the number of days of orthosis use between T45 and T180, which led us to conclude that a reduction in pain allowed clients to reduce the duration of orthosis use. Regarding adherence to orthosis use, we asked clients whether they would continue to use the orthosis after the study ended. All clients responded positively, and they all requested orthoses for other symptomatic fingers. The clients reported that although they still felt pain, they also felt some comfort; the affected joints were rested while using the orthosis, which alleviated pain in those joints.
A strength of this study is the greater homogeneity between groups as a result of the inclusion of only women (OA is more prevalent among women; Neogi & Zhang, 2013; Zhang et al., 2009), because it removes the difference in strength between men and women (Caporrino et al., 1998; de Araújo et al., 2002), which could cause bias. The treatment of the second or third finger, or both, in this trial also ensured greater homogeneity between groups. We chose to evaluate these fingers according to the prevailing literature for hand OA (Altman et al., 1990; Bagis et al., 2003).
This research has some limitations. The analysis cannot be generalized to male clients, the contralateral hand, and fingers that were not evaluated. Replication of this study should address these points. The best time to recommend orthoses and establish a comparison between joint involvement and hand function is an area for future studies regarding orthoses to treat hand OA.
Implications for Occupational Therapy Practice
This research has the following implications for occupational therapy practice:
Nighttime orthoses are effective in reducing pain and improving hand function in patients with symptomatic OA in the interphalangeal joint.
Patients had good adherence to treatment with night orthoses.
The use of nighttime orthoses is based on scientific evidence.
Conclusion
This RCT demonstrated the efficacy of nighttime orthoses for the reduction of pain in women with hand OA, especially in the IP joints of the second and third fingers of the dominant hand. The orthoses did not alter muscle strength or manual performance but did improve hand function. Fine motor coordination showed a negative correlation with a low to moderate reduction in pain. Factors that predicted an improvement in pain with the use of nighttime orthoses were the absence of Bouchard’s node in the third finger and no difficulty in performing the fine pinch for writing. The use of nighttime orthoses for OA in clients’ IP joints proved to be safe and resulted in a significant reduction in pain and improvement in manual activities. Therefore, we recommend the use of these aids in nonpharmacological treatment of OA.