
Abstract
Student teaching clinics (STCs) are increasingly used among different health professions as a means of providing valuable experiential learning opportunities to students (Holmqvist et al., 2012; Moskowitz et al., 2006; Rogers et al., 2017; Schutte et al., 2015; Simpson & Long, 2007; Wilson, 2014). STCs have been shown to help overcome shortages in fieldwork placement, provide guided practice with faculty supervision, increase interprofessional experiences, provide real-world learning opportunities to support and augment classroom experiences, develop professional reasoning, and even serve as a recruiting and marketing tool for university programs (Holmqvist et al., 2012; Moskowitz et al., 2006; Schutte et al., 2015; Simpson & Long, 2007; Wilson, 2014).
The literature describes teaching clinics in a variety of ways in the literature. In traditional student-run or student-led clinics, students are responsible for providing management and daily operations of the clinic in addition to supervised client services (Simpson & Long, 2007). Other clinic models, often described as teaching clinics or student clinics, provide opportunities for students to deliver services without involvement in the daily operations of the clinic. Although such clinics may vary in the level of students’ involvement in management of clinic operations, their primary mission, to facilitate the development of student clinical skills while delivering services to the community, remains a consistent theme (Stuhlmiller & Tolchard, 2015). We use the term student teaching clinics to refer to such clinics.
Benefits to students participating in STCs are well documented in the health profession literature. They include early exposure to real-world experiences (Bostick et al., 2014); the development of professional reasoning, clinical competence, increased confidence (Kruger et al., 2015; Seif et al., 2014, Stickler et al., 2013), professional growth, and the ability to collaborate with other health professionals (Seif et al., 2014; Stickler et al., 2013); and improved attitudes toward working with underserved populations (Schutte et al., 2015; Sheu et al., 2012; Smith et al., 2012).
Although STCs often focus on student learning outcomes, it is essential that clients of such clinics are provided with ethical, effective, and appropriate care (Buchanan & Witlen, 2006). Although clients of STCs should be aware that the services they are receiving are being delivered by students to benefit student learning, it is important to their continued participation that clients perceive a personal benefit as well (Buchanan & Witlen, 2006). Because STCs typically deliver services to underserved populations, one benefit to clients is that they may experience improved access to services (Lu et al., 2018; Simpson & Long, 2007).
Studies examining client outcomes in STCs tend to focus on the client’s satisfaction with services and service delivery (Ellett et al., 2010; Kent & Keating, 2013; Wilson, 2014) rather than on examining a change in the client’s measureable or perceived functional performance. In studies that have examined client satisfaction with STCs, clients have reported, using Likert-type satisfaction surveys, high levels of satisfaction with factors such as the overall experience; levels of trust, respect, and confidence when interacting with student clinicians; and instructions provided (Ellett et al., 2010; Kent & Keating, 2013; Wilson, 2014). A recent study by Lu and colleagues (2018) expanded the measures of client satisfaction to include issues regarding clinic operation, having medical needs met, and interactions with clinical staff. Using client reports, Lu et al. found that 75% of STC clients perceived that they experienced an improvement in their health since attending an interprofessional STC; appreciated receiving free services, including medication; and felt that their providers were knowledgeable.
Only one study was found that examined changes in client performance when participating in STCs and attempted to measure objective functional outcomes. Lavelle and Tomlin (2001) conducted a retrospective study of people with postacute cerebrovascular accident (CVA) in an occupational therapy STC using modified goal attainment scaling and found that clients made significant progress toward their goals. In addition, they found that clients achieved their goals at statistically equivalent rates regardless of gender, age, side of hemiparesis, or time since onset of CVA. Because no standardized outcome measures were identified in this study, and only one diagnostic group (CVA) was studied, generalizing results is cautioned.
The lack of current literature regarding client outcomes in STCs provides strong evidence for the need to conduct additional research on client outcomes. Therefore, the purpose of the current study was to identify the benefits that occupational therapy STCs provide to client participants and to answer the following research questions:
Is the Canadian Occupational Performance Measure (COPM; Law et al., 2005) effective in measuring client outcomes in an STC?
Do clients receiving treatment in an occupational therapy STC demonstrate significant changes in self-perceived occupational performance and satisfaction?
Method
This study used a retrospective chart review of existing pretest and posttest data. Approval for the study was obtained from the institutional review board at the University of Puget Sound (Tacoma, WA).
The University of Puget Sound has a long history of providing community service in its occupational therapy and physical therapy STCs. The occupational therapy department supports three STCs: a community-based mental health clinic, an adult onsite teaching clinic, and a pediatric onsite teaching clinic. These teaching clinics serve as Level I fieldwork experiences for second-year master’s-level occupational therapy students while providing free services to adults and children from the local community. During their final semester, students deliver supervised services to one adult client and one pediatric client as part of the required coursework.
Clinic clients present across varying ages, diagnoses, and functional levels. The pediatric teaching clinic generally serves clients younger than age 16 yr. The adult teaching clinic serves clients older than 16 but generally serves an older population. Student therapists evaluate, set goals, and design and implement varying interventions, depending on the functional level and needs of the client, while supervised by a licensed occupational therapist.
Participants
We retrospectively analyzed data from the charts of all participants who attended the university occupational therapy adult or pediatric STC during the spring of 2016. Charts consisted of both paper documents and electronic medical records. Inclusion criteria included clients who attended seven or more sessions (allowing for a full evaluation and completion of several intervention sessions) and who completed pretest and posttest assessments for the identified outcome measure. Exclusion criteria included clients who attended six or fewer sessions or clients who had incomplete pre- and posttest COPM data.
A total of 70 clients attended the spring STC; however, 14 charts did not meet the inclusion criteria, resulting in a final sample size of 56. Clients were seen for an average of 18.09 visits (range = 7–22 visits). Reasons for fewer than 22 visits included illness, vacation, no show, client discontinuation of services, and early discharge as a result of progress made.
Instrument
We chose the COPM as a required outcome measure for all clients attending the onsite clinic because of its ability to be used across a range of diagnoses, ages, and functional abilities. Additional evaluation tools were selected on the basis of each client’s individual needs.
The COPM is a client-centered, individualized outcome measure designed to detect changes in clients’ perception of their occupational performance over time (Law et al., 2005). The COPM measures clients’ perception of their current ability to perform occupational tasks and level of satisfaction with that occupational performance. Test–retest reliability of the COPM has been found to be ≥.84, and the concurrent validity and content validity of the COPM for its use as a measure of occupational performance have been generally supported (Carswell et al., 2004; Law et al., 2005).
Carswell et al. (2004) noted that the COPM was responsive to change. A change of 2 or more points on the COPM is considered clinically important (Law et al., 2005) and was chosen as the benchmark for clinical significance in the current study. We used the fourth edition of the COPM for this study because it was accessible to us. For all pediatric clients in this study, the COPM was completed by a parent or guardian as a proxy.
Procedure
Typically, clients attended the STC for 12 wk. Students completed their initial evaluation of clients over three sessions during a 1- to 2-wk period; therefore, counting 2 wk for student breaks, student-led interventions were done over 9 wk.
Students used the COPM to develop the occupational profile and to collaborate with clients to set goals, administering the test as a semistructured interview as outlined in the evaluation manual (Law et al., 2005). All students had received previous instruction on, and practice in, conducting the COPM in two separate courses during the program. Resulting goals varied in content depending on client needs and their students’ and clinical instructors’ focus. All students were strongly encouraged to write occupation-based goals emphasizing approaches outlined in the Occupational Therapy Framework: Domain and Process (3rd ed.; American Occupational Therapy Association, 2014).
Interventions primarily used an establish and restore approach but also incorporated maintain, modify, and prevent approaches designed to target outcomes of increased participation, health, and well-being. For pediatric clients, general areas addressed included basic self-care skills, social interaction skills, fine motor skills, and self-regulation. Goals for adult clients generally addressed basic self-care skills, instrumental activities of daily living, and leisure activities. Figure 1 lists collaborative goals and student-designed interventions that were used for adult and pediatric clients during the clinics to address COPM-identified client needs.
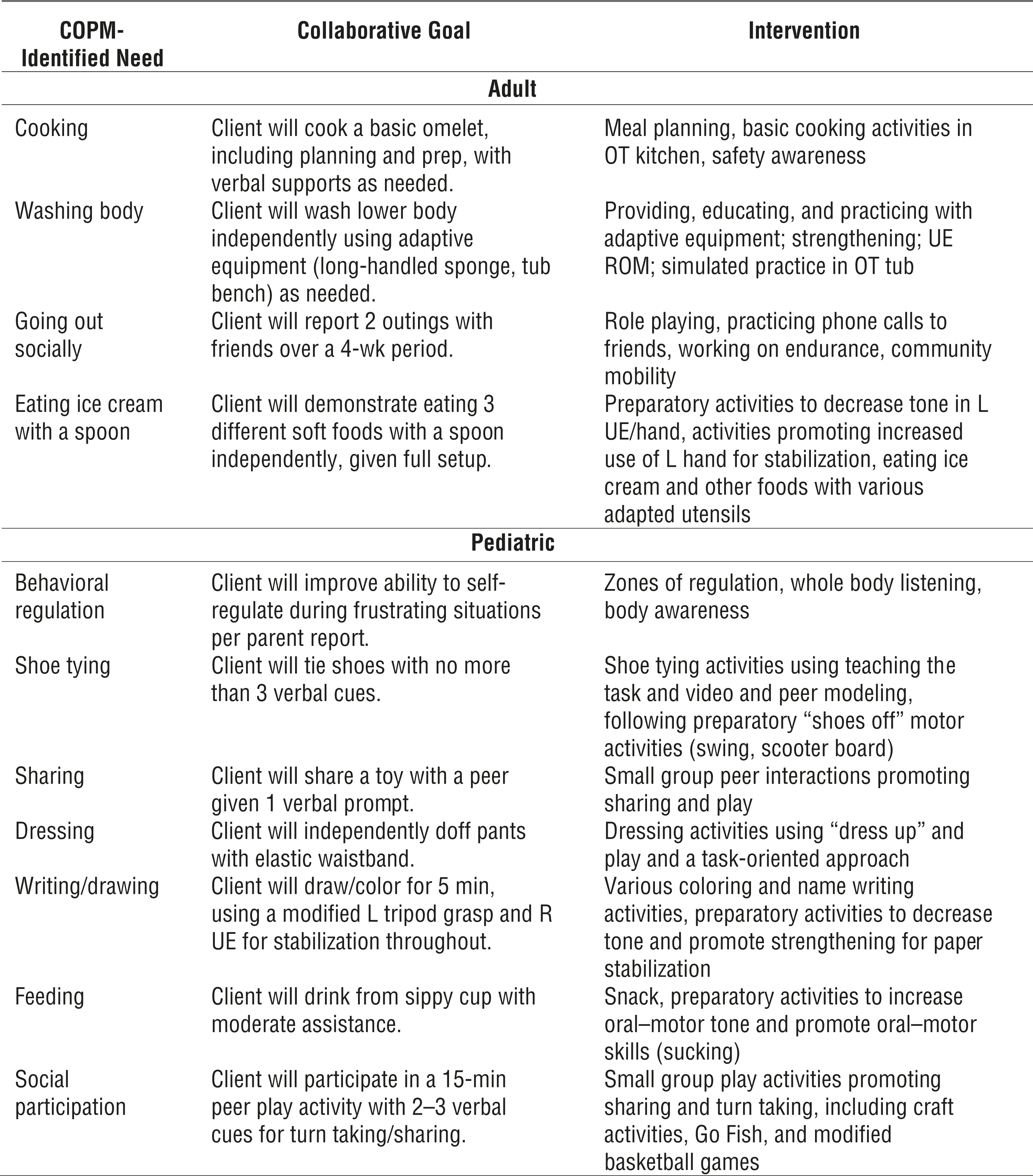
Examples of collaborative goals and student-designed interventions for adult and pediatric clients to address COPM-identified needs.
After the evaluation process, clients attended the STC twice weekly for supervised and mentored student-led interventions. Midway through the interventions, students assessed client progress and modified goals accordingly. During the final weeks of therapy, students provided their clients with home programs so that clients could preserve and advance skills that they had gained or regained during their clinic experience. In addition, students completed discharge evaluations, including a second administration of the COPM to obtain discharge scores in performance and satisfaction and to determine progress toward targeted outcomes.
Data Analysis
Upon clients’ completion of therapy, the first author (Zylstra) reviewed charts and abstracted data. Data were then analyzed by both authors using IBM SPSS Statistics (Version 21; IBM Corp., Armonk, NY), and statistical significance was established as p < .05. Demographic data (i.e., age and diagnosis) were portrayed using means and frequencies for both adult and pediatric client subgroups. Paired t tests were used to examine changes between initial and discharge COPM Performance and Satisfaction scores, for the whole sample and then for subgroups of adult and pediatric clients. Consistent with research cited by Carswell et al. (2004), a change of 2.0 in a COPM score reflects clinically significant change.
Results
Fifty-six client charts met the inclusion criteria. Thirty pediatric charts were included in the data analysis (one with incomplete performance data and one with incomplete satisfaction data), with a mean client age of 6.08 yr (range = 3.3–10.3 yr). Pediatric diagnoses included motor delay (n = 10 participants), cerebral palsy (n = 6), autism (n = 5), cognitive delay/chromosomal differences (n = 3), attention deficit hyperactivity disorder (n = 2), and other (n = 4). Twenty-six adult charts were included, and the mean age was 63.38 yr (range = 29.8–88.6 yr). Diagnoses of adult clients included stroke (n = 19 participants), traumatic brain injury (n = 1), other brain injury (n = 2), upper extremity injury (n = 2), and Parkinson’s disease (n = 2).
Results for both subgroups (adult and pediatric) of paired t tests revealed a mean increase of 1.66 points (standard deviation [SD] = 1.66), t(54) = 7.44, p < .001, n = 55, for COPM Performance scores and a mean increase of 2.27 (SD = 2.01), t(54) = 8.35, p < .001, n = 55, for COPM Satisfaction scores. These results indicate a statistically significant increase in both Performance and Satisfaction scores and a clinically significant increase in Satisfaction scores.
In the adult subgroup, the mean increase in Performance scores was 1.69 (SD = 1.76), t(25) = 4.91, p < .001, and the mean increase in the Satisfaction scores was 2.27 (SD = 2.13), t(25) = 5.45, p < .001. In the pediatric subgroup, the mean increase in Performance scores was 1.64 (SD = 1.59), t(28) = 5.54, p < .001, n = 29, and the mean increase in Satisfaction scores was 2.26 (SD = 1.94), t(28) = 6.26, p < .001, n = 29. These results indicate a statistically significant increase in both Performance and Satisfaction scores for each subgroup and a clinically significant increase in Satisfaction scores for each subgroup.
Discussion
The literature has discussed the benefits of STCs for student learning, but little research regarding the outcomes for clients who participate in these clinics has been identified. In this study, clients who received services from supervised student therapists demonstrated statistically and clinically significant increases in COPM Satisfaction scores and statistically significant increases in Performance scores. These results provide initial support for the effectiveness of student-provided therapy services from the clients’ perspective. These results are also consistent with the outcomes (measured using the COPM) of occupational therapy services delivered by experienced clinicians in six studies reviewed by Carswell et al. (2004) that showed significant changes across diagnosis groups and settings in both Performance and Satisfaction scores on the COPM.
The COPM was readily adopted by both students and clinical instructors. The COPM was an effective means of documenting perceived client progress across a wide range of ages and diagnoses in this setting. In addition, the COPM’s emphasis on client-centered occupational performance may have promoted the use of client-centered, occupation-based goals and interventions throughout the clinic, potentially promoting client satisfaction and paving the way for students to continue these practices as they enter the workforce. The results of this study are consistent with the conclusions of the systematic review by Carswell et al. (2004) that the COPM can be used as an outcome measure for occupational therapy services with a wide variety of clients and can enable client-centered practice and support outcomes research.
These findings, which suggest that clients can make measurable progress with student-provided services, may be important in discussions with insurance providers, such as Medicare and Medicaid, regarding reimbursement of student-provided services. Increased insurance reimbursement for student-provided services may lead to an increase in sites willing to take on fieldwork students. In addition, occupational therapists in outpatient settings may want to consider the use of the COPM as a patient-reported outcome measure. Further research to support these findings is recommended.
Although clients had statistically significant increases in their COPM Performance scores, a variety of reasons may explain why they did not have clinically significant changes in these scores. One explanation may be that Level I fieldwork students do not yet have the skills to support clinically significant changes over a 12-wk intervention period. One suggestion might be to increase the level of hands-on intervention and mentorship provided by the experienced clinical supervisors. In addition, clients were several years postdiagnosis and not in the acute stages of rehabilitation. It is possible that time since condition onset would affect the level of clinically significant change that can be made in an STC setting. However, this concept is not consistent with the findings of at least one study (Lavelle & Tomlin, 2001). Finally, clients attended the clinic on a volunteer basis, and many had attended for multiple years, potentially reducing the perception of performance gains.
Another important consideration is that COPM change scores are calculated by averaging outcomes on multiple goals. Therefore, although a client may not have made clinically significant gains on all goals, they may have made clinically significant gains on one or two goals, resulting in meaningful change in that person’s daily life. In addition to the COPM, other assessment tools were administered to each client presenting to the STC, depending on their individual needs and goals. Examining clinical changes on these assessment measures may strengthen results and allow the documentation of additional changes in client performance not noted by the COPM.
Limitations
Given the unique nature of the STC setting, which provides close supervision by experienced clinicians, these study results may not generalize to other settings where students perform supervised services, such as in traditional Level II fieldwork. In addition, the amount and type of mentorship and direction the various supervisors gave their students in administering the COPM likely varied. Thus, the level of training and the familiarity of the students and their supervisors with the COPM may have affected the results of this study.
The COPM measures perceived gains that may need to be validated using direct measures of performance. In addition, all areas identified as important to the client on the COPM may not have been addressed in therapy. Some of these areas may not have translated to established goals and therefore may not have been addressed during the student-led interventions. This factor may have affected the overall scores and the level of change measured by the COPM.
Traditional limitations and threats to the validity of the data resulting from retrospective studies are also applicable to this study. No control group was available, and some of the changes identified in client performance could have been the result of changes over time or as a result of social interaction between clients and students. The clients attending the STCs were also self-selected because they volunteered to participate in the STCs. Therefore, their overall motivation and commitment levels to their home programs and functional improvement may have been different from those of people attending typical outpatient clinics and may also have affected their perceptions as recorded on the COPM.
Future Research
This study’s findings warrant further evaluation of outcomes for STC clients. Larger sample sizes and use of multiple clinic sites could provide useful data for supporting the effectiveness of student-provided services. In addition to collecting further data on client-reported outcomes, studies need to address functional outcomes using direct measures of performance. This research may be useful in supporting reimbursement for student-provided services and could have an impact on the number of fieldwork sites available by promoting the development of STCs for student learning.
The COPM has demonstrated its usefulness as an outcome measure in this setting, and its use in further studies and clinical settings is recommended. This study’s findings warrant further studies that evaluate the usefulness of the COPM as a measure for occupational therapists to use. In addition, other assessments that can be readily used across client ages and conditions may be beneficial to increase understanding of client outcomes. Finally, gathering additional data on time since diagnosis and amount of previous therapy experience may be helpful in understanding and interpreting client gains.
Implications for Occupational Therapy Practice
This study has the following implications for occupational therapy practice:
The COPM appears to effectively measure client-reported progress across client ages and conditions in an STC setting.
Supervised student-provided therapy services can result in clinically and statistically significant increases in client-reported satisfaction with occupational performance.
Supervised student-provided therapy services can result in statistically significant increases in client perceptions of occupational performance.
Conclusion
This study is currently one of two demonstrating that clients who use the services of an STC perceive statistically significant gains in their occupational performance. The COPM has demonstrated its usefulness as an outcome measure in the study setting; thus, its use in clinical settings and future research is recommended.
Footnotes
Acknowledgments
We thank the University of Puget Sound for supporting our onsite occupational therapy teaching clinic. We especially thank our clients, whose participation in the University of Puget Sound’s onsite teaching clinics makes experiential student learning possible. Finally, we thank the occupational therapy students at the University of Puget Sound for their hard work and commitment to serving the surrounding community and George Tomlin for providing welcome final edits to our article.