
Abstract
Technology has been integrated into occupational therapy practice at an increasingly quick pace (Smith, 2017). Occupational therapy educators are therefore challenged to include the design and sophisticated application of technology solutions in occupational therapy curricula for students to prepare to treat clients with disabilities. When novel, off-the-shelf technological devices are first introduced to the market, they are often costly, but they usually become more accessible to consumers over time. One such technology is 3D printing, which has evolved rapidly and is becoming more accessible and commonplace (Bogue, 2013; Prato & Britton, 2015).
Applications of 3D printing in the health care industry include customized medical devices, such as hearing aids, orthodontic braces, and hip joints (Eltorai et al., 2015; Ventola, 2014; Wang et al., 2017). 3D printing has expanded to even broader medical applications, including tissue and organ fabrication, implants and prosthetics, and pharmaceutics (Ventola, 2014). Within the prosthetic field, 3D printing has the potential to be cost effective while offering individualization; however, the evidence on durability and functionality is lacking (ten Kate et al., 2017). Within the field of occupational therapy, the integration of 3D printing is gaining practical application for client use (Ganesan et al., 2016). For example, 3D-printed adaptive devices have emerged in practice settings such as schools (Buehler et al., 2014). However, limited research has been published on the feasibility or acceptance of the 3D printing process or of 3D-printed assistive devices in occupational therapy practice.
The use of technology to make adaptations to the environment that support participation and well-being is a standard of occupational therapy education, with the expectation that entry-level occupational therapy practitioners are competent in their ability to design and apply assistive technology devices (Accreditation Council for Occupational Therapy Education [ACOTE®], 2018). Assistive technology devices include products that are both specially designed and generally available to support the participation of people in their occupations (Steel & Layton, 2016).
3D printing is one of many ways to design customized devices to enhance client participation (Morgan & Schank, 2018), potentially offering lower cost and more durable alternatives than other methods (Ganesan et al., 2016). In addition, the rapid sharing of resources and knowledge in virtual “makerspaces” allows for faster device creation and sharing more quickly than ever before (Morgan & Schank, 2018). Given the makerspace trend both within and outside of occupational therapy, as well as Smith’s (2017) call to integrate technology within practice settings and to prepare occupational therapy students and entry-level practitioners to collect data outcomes when integrating “maker” technologies, further investigation into optimal integration of this technology in occupational therapy education is warranted.
Many recent university students, typically millennials or Gen Z, see technology not as tools but as devices necessary for daily life (Phillips & Trainor, 2014). In addition, millennials’ preferences for learning include experiential and interactive approaches (Phillips & Trainor, 2014). Researchers surveyed 116 entry-level Australian occupational therapy students and reported that the students preferred kinesthetic and multimodal instructional designs for learning, particularly learning through practice (Brown et al., 2008). Engaging in experiential learning activities that incorporate technology use in occupational therapy will prepare students to use this skill set in practice. In addition, occupational therapy students’ level of comfort with computer software and hardware will be instrumental in their use of technology in the future to address clients’ needs. The student preference for an experiential classroom has prompted a shift in instructional design from lectures to more engaging, experiential-based learning activities to meet the instructional standards as mandated by ACOTE (2018).
With any technology introduced to society, automatic adoption cannot be expected. Researchers have suggested that in rehabilitation practice, the perception of how technology can help in therapists’ work is the most important factor in determining their acceptance and use of technologies (Liu et al., 2015). In the theoretical foundations of the Technology Acceptance Model (TAM; Davis, 1989), perceived usefulness of devices is the determinant of future behavior to use the device in practice. Given that lack of training and negative attitudes about technology are reported barriers to its integration in practice (Copley & Ziviani, 2006), it is crucial that occupational therapy educators introduce novel technologies in educational settings to support future use of technology in practice.
Although the largest barrier to use 3D printing in practice may be a lack of occupational therapy–specific information (Martin et al., 2016), exposure to the technology through learning opportunities is necessary for future intention to use, according to the TAM. Reports on the integration of 3D printing within occupational therapy education are lacking, justifying data collection regarding changes in student acceptance of technology over time. The objective of this exploratory research study was to examine the following question: Does the integration of a 3D printing assignment within a required occupational therapy course increase the perceived acceptance of 3D printing technology by the students on the basis of usefulness, ease of use, attitudes, and intention to use the technology?
Method
Research Design
This was a one-group pretest–posttest study. The University of the Sciences in Philadelphia institutional review board approved this study.
Participants
Participants were recruited from the Spring 2018 assistive technology course, which enrolled one cohort of entry-level master of occupational therapy and doctor of occupational therapy students in their second year of the professional program. Of the 59 students invited to participate in the study, 58 completed the study.
Procedure
All students enrolled in the course were assigned a 3D printing mentor and were required to complete a 3D printing assignment in groups of three (except one group of two). Mentors were the course instructor, a fourth-year entry-level occupational therapy doctoral student, and an adjunct instructor. The students were required to use clinical reasoning skills to design and produce a 3D-printed device to assist a fictional client in increasing participation in daily occupations. The requirements of the assignment included describing the client’s contexts, environments, and client factors as the details of a fictional case study; showing that the 3D print increased client participation in daily occupations (specifying an outcomes measurement); and completing a reflection by comparing the device with a similar off-the-shelf or customized product.
During Wk 3 of the course, the instructor introduced 3D printing with two videos (approximately 2 min each), with examples of broad applications to areas not related to occupational therapy practice. The instructor then announced the opportunity to participate in an online study, which involved a questionnaire administered pre- and posttest. After signing an electronic informed consent, the students were asked four demographic questions (Table 1).
Participant Demographics (N = 58)
Note. DrOT = doctor of occupational therapy; M = mean; MOT = master of occupational therapy; SD = standard deviation.
The study questionnaire was based on the TAM, which is extensively used to predict user acceptance of technologies (Figure 1), and consisted of 13 questions scored on a Likert scale ranging from 1 (totally disagree) to 7 (totally agree; Davis, 1989; Venkatesh & Davis, 2000). The TAM integrates concepts of perceived acceptance categories, including perceived usefulness and perceived ease of use of the technology. According to the framework, these two determinants are postulates of user attitude toward the technology and intention to use the device, which influence the user’s behavior for continual use (i.e., usage behavior). Questions 1–4 correspond to the TAM’s perceived usefulness category, 5–9 to perceived ease of use, 10 and 11 to attitude toward the technology, and 12 and 13 to intention to use the device (Table 2). TAM questions are intended to be modified from the original to reflect the technology being studied. This study’s questionnaire, with modified questions, was administered online in Wk 3 (pretest) and Wk 15 (posttest).
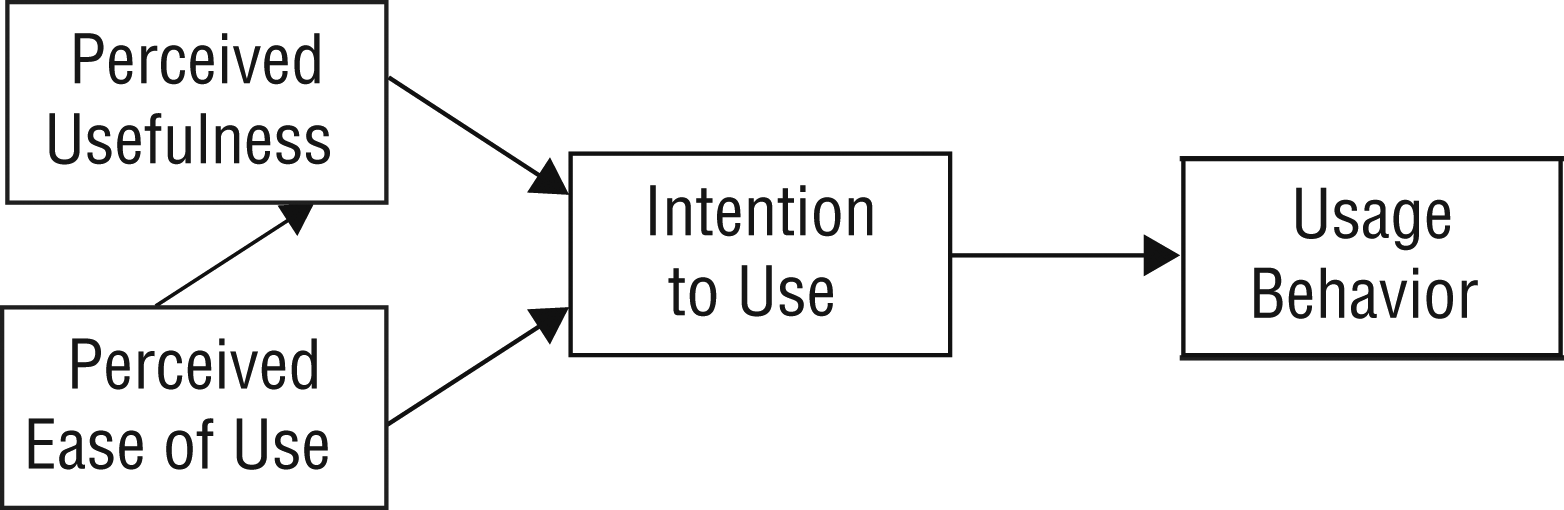
Technology Acceptance Model (Venkatesh & Davis, 2000).
TAM Pretest and Posttest Questionnaire Scores (N = 58)
Note. M = mean; SD = standard deviation; TAM = Technology Acceptance Model.
Scale: 1 = totally disagree, 2 = disagree, 3 = somewhat disagree, 4 = neutral, 5 = somewhat agree, 6 = agree, 7 = totally agree.
Questionnaire was altered from pretest to posttest to reflect change in verb tense.
Students were instructed to download software and register with Tinkercad (https://tinkercad.com) and Thingiverse (https://thingiverse.com) design-sharing sites. Students received a brief tutorial on how to operate Tinkercad online software to design their own devices. During Weeks 4–14, students were expected to come prepared to their assigned mentored session with a design already completed in Tinkercad or downloaded from Thingiverse for modification recommendations. Students were then mentored on how to operate the 3D printers. Some students received further mentoring if their printed design failed and needed to be further modified. Four 3D printers were available for use throughout the semester. Because 3D printers emit particles (Yi et al., 2016), as a safety precaution, they were stored in a well-ventilated room separate from student and faculty common areas and classrooms.
Data Analysis
From pre- to posttest, we scored students’ responses to the questionnaire to score the TAM’s four categories (Table 3). We used paired t tests to analyze 58 students’ pre- and posttest questionnaire responses with IBM SPSS Statistics software (Version 24.0; IBM Corp., Armonk, NY). Significance level was set at .05. We used Cohen’s d to calculate effect sizes of the TAM categories. Results were interpreted as 0.10, small effect; 0.30, medium effect; and 0.50, large effect (Cohen, 1988).
TAM Category Scores from Pretest- to Posttest (N = 58)
Note. M = mean; SD = standard deviation; TAM = Technology Acceptance Model.
Results
Of the 59 students who received the invitation to participate in the study, 58 completed the questionnaire pre- and posttest (98.3% response rate), and their responses were used to score the TAM categories (see Table 3). All TAM categories increased significantly (p < .05). From pre- to posttest over 12 wk, significant differences were obtained for perceived usefulness, t(57) = −3.431, p = .001, d = 0.451; perceived ease of use, t(57) = −8.583, p < .001, d = 1.136; attitude toward using, t(57) = −2.545, p = .014, d = 0.334; and intention to use, t(57) = −5.024, p < .001, d = 0.660. Individual questions were analyzed for significant changes (see Table 2), and significant differences were found for all except Questions 2 and 11.
Discussion
Study findings provide evidence that an assignment that applies 3D printing in an occupational therapy educational program may improve students’ technology acceptance. We found the largest effect size in the category of perceived ease of use (d = 1.136), which was surprising because although four working 3D printers were used, mechanical issues were ever-present. These issues included clogging of the nozzle, difficulties with changing plastic filament, difficulties with loading software and storing files between PC and Mac computers, and general printer maintenance. Perhaps the initial perception of new technology use is overwhelming to envision, as evidenced by the majority of student responses ranging from neutral to disagree on the pretest questionnaire. This large magnitude of difference seems to confirm that students appreciate the full process of 3D printing, including the struggles; therefore, they may learn to be better prepared to trouble shoot difficulties during future use.
The attitude toward using category had the smallest effect size but was still of medium effect (d = 0.334). Responses to this category’s questions (10 and 11) on the pretest questionnaire were initially fairly favorable regarding 3D printing use in occupational therapy, resulting in a ceiling effect when the majority of posttest responses were agree. However, the initial favorable ratings may be explained by previous exposure to 3D printing applications through social media outlets, which may increase awareness of and curiosity about 3D printing technology. The perceived usefulness category also increased, with statistically significant differences and a medium effect size (d = 0.451).
According to the TAM, all of the first three categories need to be favorable before the intention to use category will be influenced. Our results reflected the theoretical framework of the TAM, with the majority of students intending to use 3D printing in the future and to recommend its use to other occupational therapists. It may be interpreted that for this sample, with a large effect size (d = 0.660), the intention to use 3D printing technology improved significantly after the 3D printing assignment.
Study Limitations and Future Research
As anticipated, difficulties and malfunctions of the 3D printers occurred. Therefore, throughout the semester, we scheduled only three groups to use the four printers on a weekly basis, in case a printer was out of order. However, in many weeks, two or more printers were malfunctioning at any given time. In addition, the cost of 3D printers may limit access to 3D printing and future adoption of the technology in clinics. Because of safety concerns regarding particle emissions, the feasibility of using 3D printing machinery in health care facilities should be carefully considered.
This research design has some limitations, the first being a lack of a control group. Therefore, future research could be improved with a quasi-experimental design that uses the same pretest and posttest questionnaire but includes a control group that does not have a 3D printing assignment. Second, mixed methodology may be helpful to explain the questions that did not statistically change in positive perception, mainly Question 2 (“I think that using 3D printers would improve the effectiveness of how occupational therapists deliver services to clients”). Although we can only speculate, a possible resistance to technology integration may exist because practitioners may fear losing hands-on skills and creativity in providing unique assistive aid options for clients. Qualitative data collection may help examine the perceptions of students and practitioners to effectively deliver occupational therapy services to clients, using both novel and familiar technologies.
Last, this research did not include clients’ perception, as recommended in previous literature. For example, Lenker et al. (2013) suggested including assistive technology user perspectives in outcomes. This research also did not address whether the 3D-printed device improved client functioning in desired occupations. Client perceptions may also enhance students’ critical thinking skills to address client-centered practice. Therefore, we recommend that future research includes client perspectives and functional outcomes measurements.
Insufficient evidence exists to support assistive technology device interventions; even frequently used devices lack evidence for use (Anttila et al., 2012). This lack of evidence is further problematic because ACOTE (2018) has mandated the inclusion of assistive technology device design and training in entry-level education. Even so, although 3D printing competence is not specifically mandated to be included in educational curricula, 3D printing is one of many methods to design assistive devices. Therefore, we recommend that future research include matching potential clients to student groups to design a 3D print to address a real-life problem.
We recommend a longitudinal study to examine whether students’ perceptions are sustained and technology is used after graduation. According to the TAM (Venkatesh & Davis, 2000), over time, people will continually rely on a match between their job goals and technology use as a basis for their ongoing usefulness perceptions. We cannot expect that, as students, our participants fully understand the complexities of the job demands of occupational therapy, especially without the demonstrability of the effect of technology on client functioning outside of the authentic clinical or community practice setting.
Current 3D printing applications in the medical field involve strict oversight by the U.S. Food and Drug Administration to ensure safety of 3D-printed products for human use (Morrison et al., 2015). Unlike pharmaceutical, organ, and tissue-related 3D printing, assistive technology applications in occupational therapy do not require strict governance of 3D printing methods or materials. On the contrary, 3D-printed assistive devices for occupational therapy must meet minimal requirements, including skin sensitivity safety precautions. However, to our knowledge, safety recommendations regarding exposure to 3D-printed plastic material are not reported in the literature. Although current research provides reports on 3D-printed products as an intervention, future research should include studying the long-term effects of thermoplastics or other forms of 3D printing materials on skin, with consideration of skin sensitivities and involved, complex client conditions.
Implications for Occupational Therapy Education
This research has the following implications for occupational therapy education:
Through a 12-wk experiential learning assignment and with the integration of mentoring, technology acceptance of 3D printing may improve for students enrolled in entry-level occupational therapy programs.
When integrating “maker” technologies into educational programs, the most experiential and interactive approaches to learning should be considered.
Conclusion
Changes in perceptions of 3D printing revealed that students’ attitudes and intention to use may shift if experiential learning modules are implemented in an educational setting. For the future, we recommend an examination of clients’ perceptions of 3D-printed assistive devices compared with their perceptions of off-the-shelf devices. We hope in disseminating this information, other occupational therapy educational programs will be aware of how to integrate 3D printing assignments in their curriculum and what changes in student perceptions to anticipate.
Footnotes
Acknowledgments
Thank you to Deborah Zayon, adjunct instructor, for providing 3D printing training, support, and mentoring for this project. Thank you to the Marvin Samson Foundation for supporting the purchase of the 3D printers.