
Abstract
After a person has a cervical-level spinal cord injury (SCI), recovery of arm and hand function is a top priority during rehabilitation (Simpson et al., 2012). To address this goal, occupational therapy practitioners commonly apply electrical stimulation (ES) to facilitate performance of upper extremity (UE) activities (Popovic et al., 2011).
Six neuromuscular applications of ES are commonly used. Neuromuscular electrical stimulation (NMES) is used to elicit a muscle contraction. When NMES is coupled with a specific, planned functional task (e.g., cycling), it is referred to as functional electrical stimulation (FES). The use of a wearable NMES device is called a neuroprosthetic. Biofeedback-triggered NMES enhances muscle contractions by triggering a stimulation when electromyographic activity exceeds a clinician-defined threshold, triggering stimulation. Transcutaneous electrical nerve stimulation (TENS) is a form of ES targeting pain management (Kapadia & Popovic, 2011; Lynch & Popovic, 2008; Maffiuletti, 2010). ES coupled with high-repetition, task-oriented FES is called activity-based restorative therapy (ABRT), which seeks to promote recovery of neural function (Sadowsky & McDonald, 2009). For each of these ES applications, occupational therapy practitioners choose parameter settings (e.g., waveform shape, frequency, intensity, pulse duration, pad placement and size) on the basis of client factors and activity.
To date, ES literature associated with central nervous system lesions has largely focused on applications for the stroke population (Marquez-Chin et al., 2017). For the SCI population, NMES can improve muscle mass, reduce risk of skin breakdown, and address bone density loss (Dudley-Javoroski & Shields, 2008; Gordon & Mao, 1994; Kapadia & Popovic, 2011; Maffiuletti, 2010; Marquez-Chin et al., 2017). High-repetition, task-oriented training supported by FES (i.e., ABRT) may effectively promote independence with activities of daily living and contribute to neuroplastic changes (Kapadia & Popovic, 2011; Sadowsky & McDonald, 2009). Popovic et al. (2006) found clinical improvements in hand function after 12 wk of ES therapy, albeit not statistically significant. Martin et al. (2012) reported statistically significant improvements in overall UE performance, function, and speed after 2 wk of NMES application.
Occupational therapy practitioners do not receive systematic education and training on ES interventions. Occupational therapy programs have limited requirements for delivery of ES content in preprofessional curricula (Accreditation Council for Occupational Therapy Education, 2012). State occupational therapy practice acts vary in their incorporation of ES as an occupational therapy treatment modality. Moreover, published studies do not provide explicit guidance for implementation of ES with clients who have SCI. The Paralyzed Veterans of America Consortium for Spinal Cord Medicine (2005) developed guidelines for upper limb rehabilitation, which mention FES without specific implementation guidance. Nussbaum et al. (2017) recommended use of NMES for treatment of muscle impairment, but they did not detail its clinical application. Fehlings et al. (2017) ranked ES as “low evidence” on the basis of the strength of study designs in the ES literature. Despite this conclusion, they suggested that NMES should be used clinically because potential benefits outweigh drawbacks; however, no specific guidelines for ES implementation were included. Therefore, it appears that no clinical practice document explicitly guides occupational therapy practitioners about appropriate, goal-related implementation of ES for this population.
The absence of uniform practice guidelines suggests the potential for low treatment fidelity in clinical deployment of this modality. In this study, we surveyed clinicians about their use of ES with clients who have a cervical-level SCI. The goal was to ascertain how ES is being used in occupational therapy practice, specifically, its clinical rationale; expected benefits to performance skills and occupations; parameter settings; and research evidence being used as a basis for treatment protocols.
Method
Design
A web-based survey was used to obtain a one-time, cross-sectional snapshot from a geographically dispersed sample of occupational therapy practitioners. The online format was chosen to maximize participation and to afford consistent data capture. The study procedures were approved by the institutional review board at Northwestern University.
Participants
Using public data, we contacted managers at rehabilitation facilities accredited by the Commission on Accreditation of Rehabilitation Facilities (CARF) and members of the SCI Model System Network (http://www.msktc.org/sci/model-system-centers). The managers and members were requested to forward the survey link to occupational therapy staff who met the following inclusion criteria: (1) current licensure as an occupational therapist or occupational therapy assistant, (2) recent experience (previous 6 mo) treating people with SCI, and (3) state eligibility to administer ES as an occupational therapy treatment modality. Information on whether participants were occupational therapists or occupational therapy assistants was not collected.
Instrument
The goal was to create a survey that would be amenable to online delivery and yield adequate depth of information without becoming onerous for respondents. The research team drafted a preliminary set of item stems and response options that were subsequently revised on the basis of two focus groups, one with clinical experts in SCI and one with three managerial colleagues who gave editorial feedback on clarity and formatting. Whenever possible, closed-ended questions were used to increase reliability of responses and to reduce respondent burden. The final version of the survey consisted of 37 items: 10 items about ES parameter settings (e.g., amplitude, pulse width, frequency, duty cycle, waveform, ramp time); 2 items regarding their chosen ES protocol; 18 items about ES treatment rationale, clinical decision making, and goals; and 7 items for which respondents rated level of confidence with their clinical decision making associated with ES.
Procedure
Prospective participants received an electronic invitation to complete the survey, which was forwarded from their clinical manager. The invitation included a link to consent information and survey items. All responses and submissions remained anonymous and contained no identifiable information. Participants did not receive an honorarium, but a subset of participants were randomly selected to receive a gift card and tablet computer. The survey was available on SurveyMonkey® (SurveyMonkey, San Mateo, CA) from April 1, 2014, to September 1, 2014.
Data Analysis
The responses were checked for potential data entry errors (e.g., numeric outliers resulting from miskey) and missing data. We descriptively summarized data using IBM SPSS Statistics (Version 24; IBM Corp., Armonk, NY). Free text responses were thematically grouped and checked for consistency by two members of the research team.
Results
Investigators contacted 112 sites, representing 103 CARF centers and 14 model system units (5 sites qualified as both). A total of 73 respondents provided consent; 72 were eligible to administer ES according to their state practice act, and 57 ultimately completed the survey. The survey interface did not require a response for every question; therefore, not all items were answered by all 57 participants. Table 1 summarizes respondent demographics. All regions of the United States were represented. All respondents had used ES in a treatment session with a client who had SCI within the previous 6 mo. The following types of ES equipment were most commonly available at respondents’ clinic sites: NMES (n = 54; 94.7%), TENS (n = 48; 84.2%), FES cycle (n = 34; 59.6%), UE neuroprosthetic (n = 24; 42.1%), and biofeedback-triggered NMES device (n = 26; 45.6%). Figure 1 illustrates respondents’ clinical rationale for using ES on clients with SCI, and Figure 2 shows the activities most often performed by clients in conjunction with ES. More than half of the respondents (n = 31; 54.4%) reported using ES on inactive muscle groups.
Participant Demographics (N = 57)
Note. CEU = continuing education unit; ES = electrical stimulation; SCI = spinal cord injury.
Information on the number of occupational therapists and occupational therapy assistants was not collected.
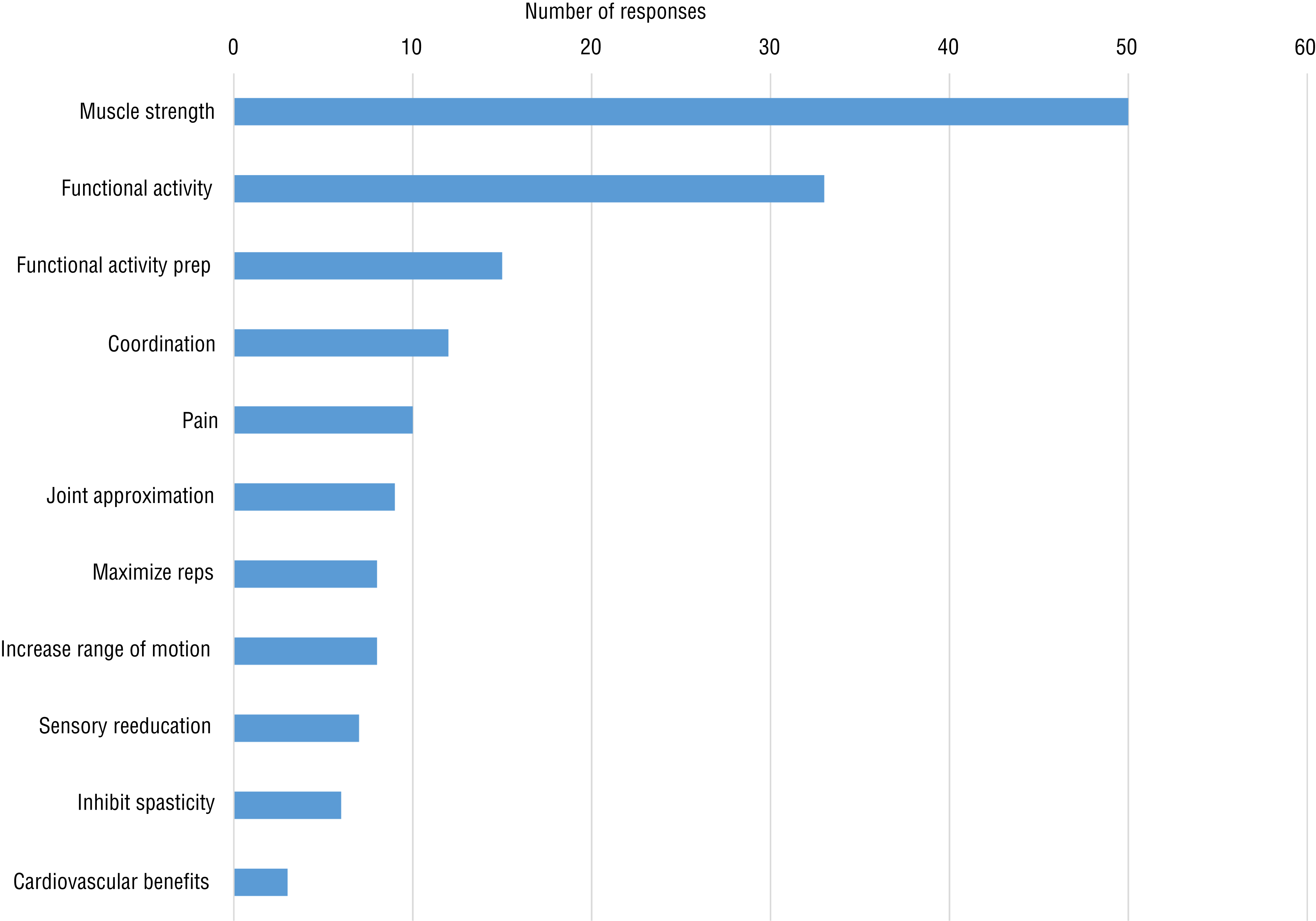
Clinical rationale reported by occupational therapy practitioners (N = 57) for using electrical stimulation (ES) on clients with a cervical-level spinal cord injury (SCI).
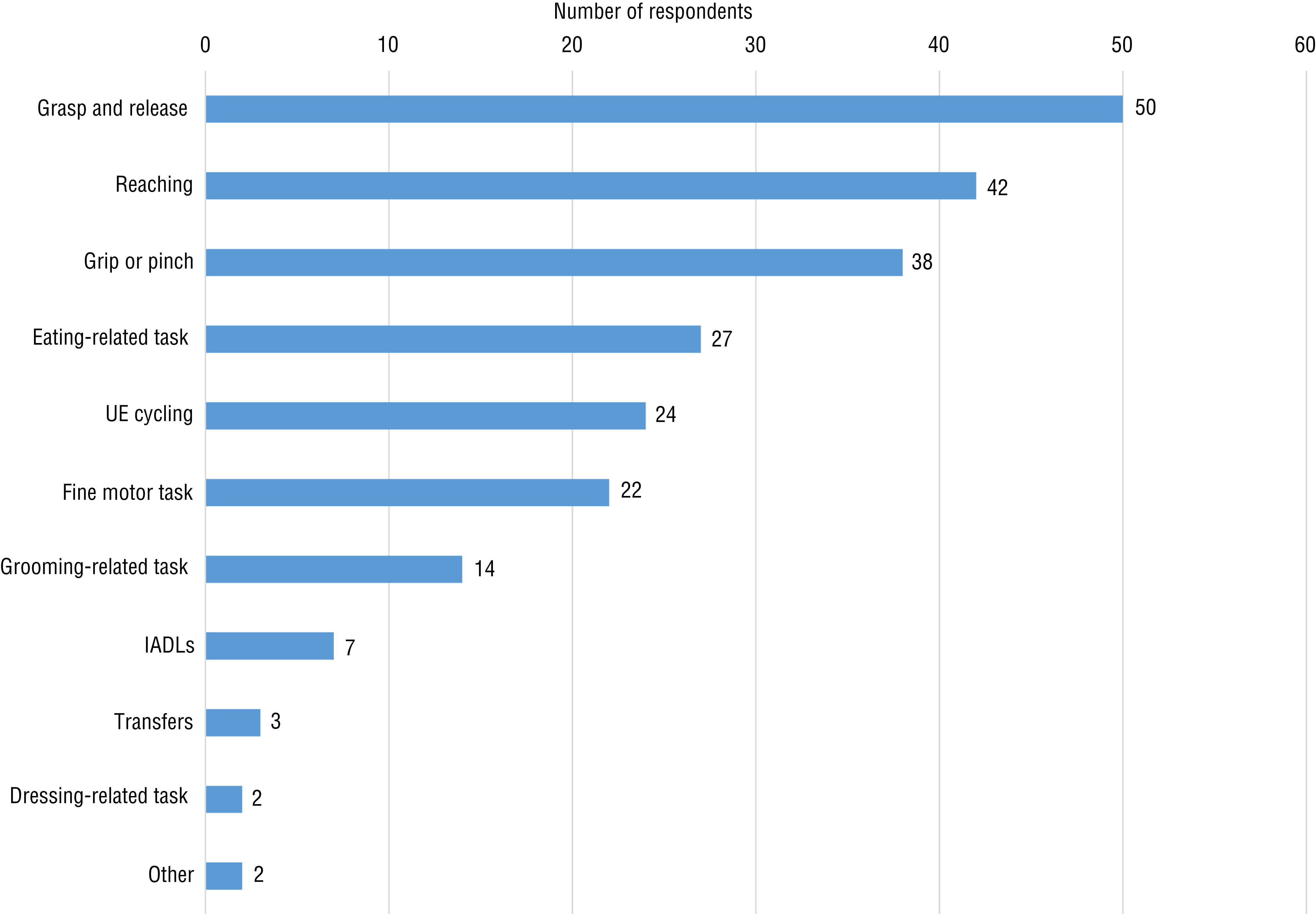
Functional activities used by occupational therapy practitioners (N = 57) during the application of electrical stimulation (ES) on clients with cervical-level spinal cord injury (SCI).
The open-ended questions regarding ES parameter settings elicited a range of responses. The mean lowest amplitude level (n = 43) was 24.2 mA (range = 1–45 mA), and the mean maximum level (n = 44) was 40 mA (range = 15–80 mA). Almost 90% of the respondents (n = 38/44; 86%) used a pulse duration between 250 and 350 µs. The mean lowest frequency (n = 43) was 35.0 Hz (range = 1–80 Hz), and the mean maximum frequency (n = 43) was 40.8 Hz (range = 20–80 Hz). For duty cycle, 38.3% (n = 18/47) reported using 1:1, 23.4% (n = 11/47) reported using 1:3, and 19.1% (n = 9/47) reported using 1:2. Twenty respondents reported using asymmetrical waveforms, 18 reported using symmetrical waveform, and 6 reported using both waveform patterns.
More than half of the respondents (n = 32/56; 57.1%) used a protocol to guide their ES treatment sessions. The basis for their ES protocols came from a variety of sources: anecdotal recommendations (n = 23/56; 41.1%), equipment manuals provided by manufacturers (n = 19/56; 33.9%), published evidence (n = 16/56; 28.6%), and facility-specific protocols (n = 12/56; 21.4%). Respondents reported a range of ES intervention schedules, with a mean duration of 27.0 min per session (range = 15–60 min), a mean treatment frequency of 3 sessions per week (range = 1–6), and a mean treatment duration of 4.8 wk (range = 1–12 wk).
Respondents reported greatest confidence with selecting appropriate patients (91.1% confident or very confident), initiating ES treatment sessions (82.2% confident or very confident), placing electrodes (82.2% confident or very confident), and selecting ES parameters (77% confident or very confident). Respondents were least confident deciding when to discontinue ES (28.6% neutral or unconfident) and documenting goals for ES interventions (32.1% neutral or unconfident). The five most frequently reported methods of monitoring functional progress associated with ES treatments included clinical observation (n = 52/56; 93.0%), manual muscle test (n = 40; 71.4%), patient subjective report (n = 38/56; 67.9%), grip and pinch strength (n = 28; 50.0%), and FIM™ (n = 26/56; 46.4%). The three most frequently reported barriers to using ES were “time required to follow a specific protocol” (n = 33; 60.0%), “patient tolerance” (n = 32; 57.1%), and “patient motivation” (n = 13; 23.2%).
Discussion
We believe this is the first study to report data from occupational therapy practitioners about their use of ES with clients who have SCI. The data reflect the perspectives of practitioners from specialized SCI settings. The results suggest that clinical deployment of ES is not uniform across clients and settings. Our findings indicate that more than 40% of the survey respondents were not using a specific treatment protocol, and more than 70% were not basing their interventions on published research, suggesting that ES was not being deployed by practitioners as a true evidence-based intervention. The wide range in parameter settings reported by participants could have contrasting interpretations. On the one hand, the range possibly reflects lack of treatment fidelity across practitioners; on the other hand, the range might reflect an appropriately graded customization of ES parameters on the basis of client factors and treatment goals.
Approximately half of the respondents reported using ES on inactive muscle groups. Historically, researchers have suggested that applying ES to a limb with no muscle activation (i.e., a manual muscle testing score of 0) has no therapeutic benefit because of denervation in the central nervous system (Gordon & Mao, 1994; Maffiuletti, 2010). However, this finding is controversial, and there may be patient-specific situations in which stimulation to an inactive muscle supports an opportunity for muscle function restoration.
In summary, the findings indicate that the clinical deployment of ES appears to lack a clear decision-making process that is based on research evidence. This ambiguity suggests the need for a guide that describes individual-centered ES interventions that are consistent with research data, client treatment goals, and principles of adapting interventions to meet individual needs to foster consistent patient outcomes. Such a guide could meet the needs of both experienced and novice practitioners by including, for example, introductory sections describing underlying physiology and mechanisms of action, clear definitions of terminology, electrode placement instructions, suggested parameter settings for different muscle groups and activity goals, expected functional outcomes, adaptive strategies for novel client circumstances, and troubleshooting strategies.
Limitations
Although survey items were designed to minimize respondent burden, the number and diversity of questions may have discouraged survey completion and introduced unknown bias to the results. The relatively small sample size limits discipline-wide generalizability. In addition, participants were not asked to specify whether they were an occupational therapist or occupational therapy assistant. We did not believe it was necessary to differentiate between the two as long as individual respondents were practicing within their state’s practice act. We ascertained the latter criterion in Question 6 of the survey: “Are you eligible by the rules and regulations of your State Practice Act to administer electrical stimulation?” Respondents who answered “no” to this question were unable to continue the survey. Finally, the data were collected in 2014 and therefore may differ from practice at the time of publication. In the absence of more recent published data, the findings here nonetheless provide insights that remain useful to current occupational therapy practice considerations.
Implications for Occupational Therapy Practice
The results of this study have the following implications for occupational therapy practice:
When using ES interventions on clients who have SCI, occupational therapy practitioners rely heavily on information from colleagues, manufacturer manuals, and ambiguous guidance from the rehabilitation literature.
Many occupational therapy practitioners do not use a protocol when using ES, and the data suggest that treatment parameters are not uniformly applied.
These factors introduce unknown effects on client outcomes.
Conclusion
Among occupational therapy practitioners working with the SCI population, ES is regularly used because of its perceived benefit for clients engaged in functional activities. However, many practitioners do not use a protocol to guide their ES interventions, and only a minority use the research literature to inform their treatments. Implicitly, these latter factors introduce unknown effects on client outcomes, do not reflect a truly evidence-based treatment, and suggest the need for the development of clinical practice guidelines that support practitioners who use this intervention, particularly practitioners who are novice ES users. An occupational therapy–specific clinical practice guideline would establish a convention for ES implementation, foster consistent clinical decision making, and support systematic scientific evaluation.
Footnotes
Acknowledgments
We acknowledge the Shirley Ryan Ability Lab (formerly the Rehabilitation Institute of Chicago), which financially supported this research through the Buchanan Fellowship Fund. We also thank our colleagues from the Shirley Ryan Ability Lab who provided insight and expertise that greatly assisted the research.