
Abstract
Acquired brain injury (ABI) is a leading cause of disability, leaving survivors with lifelong challenges including mild to severe physical and cognitive impairments (Bruns & Hauser, 2003). Cognitive impairment is considered the most disabling and distressing impairment (Barman et al., 2016). Evidence suggests that up to 70% of stroke survivors have cognitive impairment (Sun et al., 2014), and approximately 65% of brain injury survivors have reported long-term problems with cognitive functioning (Rabinowitz & Levin, 2014).
Impaired cognitive functions are among the strongest predictors of lifelong disability, prolonged hospitalization, institutionalization, and poor quality of life (Jette et al., 2005; Nys et al., 2007). People with cognitive impairment may experience limitations in learning, processing, assimilating information, and developing life goals (Patel et al., 2003). These limitations often result in challenges with participation in society reflected in unemployment, limited social relationships, and limited access to community activities (Barman et al., 2016). Although people with cognitive impairment after ABI can benefit from regular rehabilitation services, evidence shows that they may not benefit as much as people without cognitive impairment (Rabadi et al., 2008). Rehabilitation programs that are tailored to the needs of people with cognitive impairment are therefore necessary.
One widely used rehabilitation approach to address cognitive impairment is neurocognitive functional training. This training approach focuses on restoring cognitive functions such as memory and attention (Merzenich et al., 2002). However, the effectiveness of neurocognitive functional training usually does not persist. In addition, limited evidence supports its effectiveness for activity and participation outcomes such as return to work, social interactions, and community participation (Kumar et al., 2017).
Because of the limitations of neurocognitive functional training, alternative training approaches have been developed (McEwen et al., 2010). Metacognitive strategy training, referred to as strategy training in this article, is one such approach (Dawson et al., 2013). During strategy training, practitioners guide clients to identify challenges in daily activities and to generate their own solutions to these challenges (Skidmore et al., 2015). Strategy training emphasizes the practitioner’s role as facilitator, guiding clients to learn through prompts and questions. Identifying problems and developing strategies to address them can promote clients’ self-efficacy and confidence in managing participation challenges (Dawson et al., 2017; Polatajko et al., 2012). Clients can also be guided to generalize the strategies they learn to other similar problems they encounter in daily life.
Strategy training has been applied with a variety of clinical populations, including adults with ABI (Dawson et al., 2013; McEwen et al., 2010; Skidmore et al., 2015). Although findings are still preliminary, strategy training has shown the potential to help clients achieve their treatment goals and even transfer the strategies they learn to real-world activities (Dawson et al., 2013; McEwen et al., 2010). Strategy training has also shown promise for improving functional independence (Skidmore et al., 2015), even among people with poor self-awareness who were believed to be unable to benefit from the intervention (Skidmore et al., 2018). However, it is unclear whether this training can improve client participation, the ultimate rehabilitation goal.
Strategy training has been studied primarily in Western countries. Culture plays a significant role in people’s perceptions of their illness and expectations for treatment (Banja, 1996). Strategy training focuses on clients’ empowerment, self-autonomy, and independence, which may not be emphasized as heavily in Chinese clinical contexts as in Western culture. Only one study has examined strategy training for children in an Asian context (Chan, 2007). Therefore, before this intervention approach could be introduced in a cross-cultural (Chinese) context, it was necessary to evaluate whether the approach would be acceptable to the target population or would require cultural adaptation (Banja, 1996).
The purpose of this study was to apply strategy training to improve participation outcomes of rehabilitation clients and to examine whether the intervention is feasible and acceptable within a Chinese clinical context. The specific aims of this study were to assess the feasibility and acceptability of the strategy training intervention for Chinese adults with cognitive impairment after ABI, to evaluate the preliminary effects of the intervention on participation outcomes, and to determine which cultural adjustments may be necessary for the intervention.
Method
Design
A single-group, repeated-measures design was adopted for this study. All participants received the participation-focused strategy training intervention and were administered assessments at baseline and postintervention. The study protocol was approved by the university institutional review board.
Participants
Adults with a primary diagnosis of ABI who were receiving outpatient rehabilitation services at four teaching hospitals were recruited for this study. Participants were included if they were age ≥20 yr, had a diagnosis of ABI, were able to understand Mandarin, had cognitive impairment (i.e., score of ≤25 on the Montreal Cognitive Assessment; Dong et al., 2010; Nasreddine et al., 2005), and were able to understand and provide informed consent. Potential participants were excluded if they had severe aphasia, were diagnosed with dementia before the ABI, or currently had major depressive disorder, substance use, or other psychiatric disorder that might impede their participation in the study. Two trained research assistants collaborated with therapists at the recruitment sites to screen for eligible participants through medical chart review and personal interviews and to ascertain interest in study participation. Informed consent was obtained from all participants.
Intervention
The intervention protocol was modified from the strategy training intervention protocol developed by Skidmore et al. (2015). Participants engaged in the intervention in addition to their usual outpatient rehabilitation (including occupational therapy, physical therapy, and speech therapy, 1–3 days/wk). Three trained research occupational therapists (Pei-Chun Yeh, Yi-Hsuan Wu, Wan-Chi Lin) delivered the intervention to participants following standardized procedures in a quiet room in the rehabilitation department of the hospital where participants were recruited. The principal investigator (PI; Feng-Hang Chang), who received training from an expert therapist (Chao-Yi Wu), provided consistent in-person training to the research therapists and supervised and provided feedback on the first two sessions with each participant.
At the beginning of the intervention, the therapists explained the meaning of participation (Chang & Coster, 2014) to the participants. Then, the therapists used the Canadian Occupational Performance Measure (COPM; Law et al., 2005) to facilitate the participants’ identification of three participation-related goals. Next, the therapists asked the participants to identify barriers to achieving these participation-related goals and taught them to use the Goal–Plan–Do–Check global strategy to address these barriers. The global strategy involves (1) setting a goal to address the barriers, (2) developing a plan to achieve the goal, (3) doing the plan, and (4) checking whether the plan worked or required revision. This procedure was repeated iteratively until each participant’s goal was met, and then the participant moved on to the next goal. At the end of each session, the therapists prompted participants to identify the principles they learned during the session and encouraged them to apply these principles in the next session. Each participant received one or two 45- to 60-min intervention sessions per week for a maximum of 10–20 sessions or until their goals were achieved.
Measures
All data were collected by a trained interviewer. Demographic variables were collected at baseline using a questionnaire developed by the research team. Clinical variables (e.g., diagnosis, time since onset) were retrieved from participants’ medical charts.
Feasibility Indicators
We assessed feasibility by examining the following:
Number of participants recruited and retained
Number of intervention sessions participants attended
Participants’ engagement in the intervention sessions, assessed by the research therapists using the Pittsburgh Rehabilitation Participation Scale, measured on a 6-point scale ranging from 1 (no engagement) to 6 (excellent engagement; Lenze et al., 2004)
Participants’ comprehension of the intervention content, assessed using a 3-point scale ranging from 1 (minimal understanding) to 3 (good understanding; Skidmore et al., 2014)
Participants’ satisfaction with the intervention, assessed using the 8-item Client Satisfaction Questionnaire, with total scores of 0–23 indicating poor to fair satisfaction and 24–32 indicating moderate to high satisfaction (Attkisson & Greenfield, 1994)
Research therapists’ adherence to the intervention protocol, measured by the Strategy Training Fidelity Checklist (Skidmore et al., 2014), for which an independent rater randomly selected 20% of sessions (excluding the first sessions, which were used as training sessions) to rate the therapists’ adherence to intervention protocol principles (yes or no) and competence in execution (inadequate, adequate, or exceptional).
Outcome Measures
The primary outcome of this study was change in participation performance, which was measured using the Participation Measure–3 Domains, 4 Dimensions (PM–3D4D; Chang et al., 2016). The PM–3D4D is a 19-item measure designed to evaluate three domains of participation—Productivity, Social, and Community—rated on four dimensions:
Diversity of participation (1 = yes, 0 = no)
Frequency (5- and 7-point scales from never to every day or almost every day)
Desire for change (1 = yes, 0 = no)
Difficulty (4-point scale from 1 = very difficult to 4 = not difficult at all).
Each dimensional score of the PM–3D4D can be separately summed for each domain. Psychometric properties of the PM–3D4D were established in rehabilitation populations (Chang, 2017; Chang et al., 2017). For the purpose of this study, the Diversity, Frequency, and Difficulty dimensions were used for analyses, with high scores indicating more diversity and frequency and less perceived difficulty with participation (minimal detectable change ranges from 0.11 to 4.57; Chang, 2017).
Participants’ improvement on the participation-related goals they identified during the intervention was scored using the COPM. The COPM asks respondents to rate their performance of and satisfaction with performance for each self-selected goal on a 10-point visual analog scale. This rating was conducted at baseline and postintervention. A change of 2 points or more on the COPM is considered clinically significant (Law et al., 2005).
Observational Data
All intervention sessions were audio recorded. Observational data and notes from the therapists, assessors, and research team meetings were collected and reviewed by the research team throughout the study.
Data Analysis
Data were analyzed using SAS Version 9.4 (SAS Institute, Cary, NC). Descriptive analyses were conducted to describe the frequency, percent distribution, mean, and standard deviation of all variables. We calculated the magnitude of change in the outcome variables using Cohen’s d effect size (Cohen, 1988). An effect size of 0.20 indicates a small effect, 0.50 indicates a moderate effect, and 0.80 indicates a large effect (Cohen, 1988).
Observational data were analyzed with the conventional content analysis approach (Hsieh & Shannon, 2005). Transcribed data were reviewed and coded by two independent coders, and the PI reviewed their coding results to ensure quality and consistency. Data relevant to challenges the therapists encountered while delivering the intervention were coded and sorted into categories.
Results
Figure 1 displays the recruitment and retention of participants in the various stages of this study. Of the 23 rehabilitation patients recruited from 2017 to 2018, 3 were ineligible and 20 completed baseline assessment procedures. Participant characteristics are shown in Table 1.
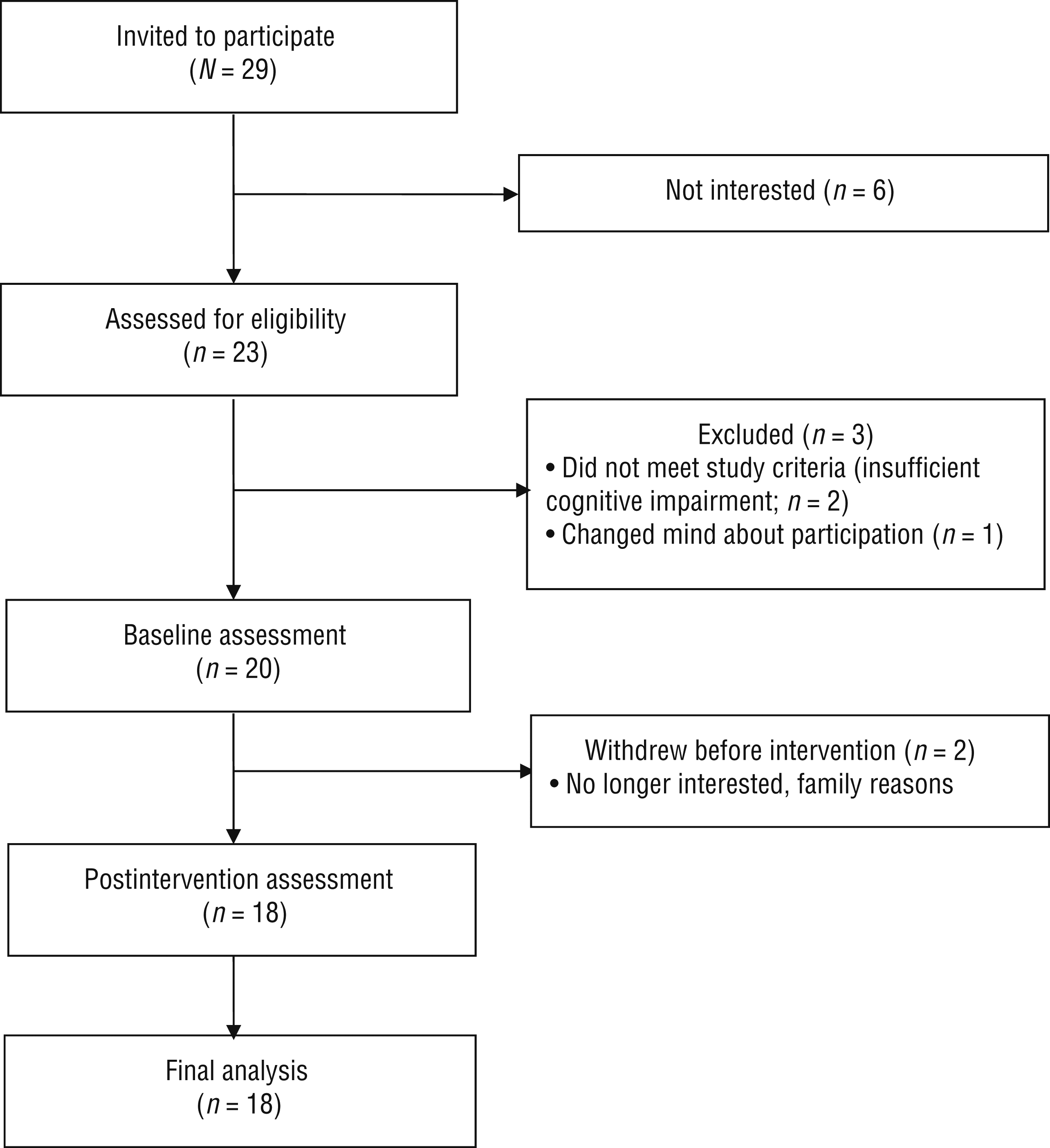
Flow diagram of participant recruitment and retention.
Participant Characteristics (N = 20)
Note. M = mean; MoCA = Montreal Cognitive Assessment; SD = standard deviation.
Feasibility
Of the 20 participants, 2 withdrew after baseline assessment (1 woman; mean [M] age = 64.5 yr), and the remaining 18 participants completed 100% of scheduled sessions (range = 8–17, M = 11.9, mode = 12). Participants’ average score for engagement in intervention sessions was 5.1 ± 1.0 on a 6-point scale, indicating that they engaged in all activities with maximal effort and finished all activities but passively followed directions (Lenze et al., 2004, p. 384). Participants’ average comprehension of the intervention was 2.4 ± 0.4 on a 3-point scale, indicating that they had some to good understanding of the intervention. All participants reported moderate to high satisfaction with the intervention (i.e., scores in the 24–32 range on the Client Satisfaction Questionnaire; M = 29.3 ± 3.3). Fidelity ratings for the sampled intervention sessions showed that the therapists adhered to the intervention protocol and demonstrated adequate or exceptional competence in all procedures.
Preliminary Efficacy
Change scores on the PM–3D4D and the COPM are displayed in Table 2. Positive changes were observed in the overall scores on the PM–3D4D Diversity, Frequency, and Difficulty dimensional scales as well as in subscale scores (M changes = 0.12–9.33), indicating that participants who received the intervention participated in more activities on a more frequent basis and perceived less difficulty with participation than they did before the intervention. The largest effects were observed in the Frequency scores (ds = 0.87–1.25), whereas the smallest effects were observed in the Difficulty scores (ds = 0.58–0.76).
Outcome Measure Results
Note. COPM = Canadian Occupational Performance Measure; M = mean; PM–3D4D = Participation Measure–3 Domains, 4 Dimensions; SD = standard deviation; T1 = baseline; T2 = postintervention.
Positive changes were also found in COPM Performance (M change = 2.49) and Satisfaction (M change = 3.12) scores. These change scores were clinically significant (i.e., >2.00; Table 3).
Participants’ Goals and Canadian Occupational Performance Measure Scores
Note. Scores for the Performance and Satisfaction scales of the Canadian Occupational Performance Measure could range from 1 to 10. Scores reported are the clients’ mean rating score for the goals they listed. T1 = baseline; T2 = postintervention.
Observations Related to Implementation in the Chinese Context
The content analysis showed that the research therapists encountered several challenges as they delivered the intervention. First, some participants had difficulty identifying their own goals during the intervention. To help participants identify goals, the therapists applied strategies in addition to using the COPM. For example, one strategy was to show participants a checklist of examples of life situations they might have experienced or wished to participate in, and another was to encourage participants to discuss meaningful goals with their family or significant others.
Second, many participants relied on their caregivers to manage their daily life and were not used to making plans for themselves. They required extra guidance from the therapists to discover their own strategies to achieve their goals. Furthermore, because many participation-related goals, such as walking in the park or going grocery shopping, occurred in the community, supervision or assistance by caregivers was necessary for safety reasons. After a few trials, the research therapists found that involving caregivers in the Plan–Do–Check process was frequently helpful.
Finally, most of the participants were used to receiving direct guidance from their therapists during rehabilitation. Many participants were unsure what to do when the therapists asked them to make their own plans to accomplish their goals. More explanation about why the participants were expected to identify their own strategies and additional guidance from the therapists were sometimes necessary.
Discussion
To our knowledge, this study is the first to apply a strategy training approach for improving participation among community-dwelling adults with cognitive impairment after ABI in an Asian country. Preliminary data from this study suggest that this intervention is feasible for delivery as an adjunct to outpatient rehabilitation. We were able to recruit and retain participants without significant loss to follow-up. At the end of the study, all participants reported moderate to high satisfaction with the intervention. Many expressed appreciation for the intervention because it was the first time they felt that they were able to do something they desired instead of being a “patient” who was disabled and highly restricted. Participants completed 100% of the scheduled intervention sessions, which was beyond our expectation. For all participants, it took 10–20 sessions to accomplish three to four participation goals. Our findings suggest that the number of sessions participants needed may have varied depending on their goals, their abilities, and the supportive resources and environment available in the community. These findings provide guidance for future intervention design.
Although preliminary, our findings regarding efficacy are promising. Participants who received strategy training showed improvement in overall diversity, frequency, and difficulty of participation performance. A previous study examining the efficacy of a participation-focused intervention for stroke survivors found no significant improvement in participants’ satisfaction with participation (Kessler et al., 2017). The authors attributed this finding to changes in participants’ expectations for participation over time, indicating that subjective perspectives of participation may not have reflected the actual changes that resulted from the intervention (Kessler et al., 2017). Our study suggests that both subjective (perceived difficulty) and objective (frequency and diversity) dimensions of participation were responsive to the intervention, although larger changes were observed in the objective dimensions. Further research with continued follow-up assessments is warranted to examine whether effects on participation can be maintained after the intervention.
Previous studies have shown that people receiving strategy training demonstrated improvement in COPM Performance scores for their self-selected goals, most of which were activity focused (Polatajko et al., 2012; Skidmore et al., 2011). Our participants had clinically meaningful improvement in both COPM Performance and Satisfaction scores for their participation-related goals. Future efficacy research is needed to provide evidence supporting the use of the Goal–Plan–Do–Check strategy for enabling participants to achieve self-selected goals that span activities and participation.
We identified two cultural adjustments that may promote the implementation of strategy training in a Chinese context. First, perspectives of independence and autonomy differ between Asian and Western cultures (Tseng & Chang, 2017). Although strategy training requires participants to select their own goals and self-identify strategies to achieve their goals, many of our participants reported difficulty with this aspect of the intervention. It was common for their daily lives to be planned and arranged by their caregivers (e.g., spouse, parents, children). In fact, some participants did not believe they were even capable of making their own decisions because they had rarely been allowed to do so since their injury. In Asian cultures, people (particularly older adults) with a disabling condition are likely to depend on family members, who are expected to provide care and make decisions (Tseng & Chang, 2017). After recognizing this cultural difference, we determined that involving caregivers in the intervention might both support participants and help caregivers understand the purpose and merit of the intervention.
Second, strategy training is very different from traditional rehabilitation delivered in Taiwan. Traditional rehabilitation focuses primarily on impairment remediation and activity-level functional restoration. Therapists usually assign task-specific training to clients instead of guiding them to set goals and develop plans. Participation is rarely the focus of outpatient rehabilitation because of the restrictions of hospital settings (Tseng & Chang, 2017). Because strategy training was foreign to most participants, the research therapists frequently reinforced the purpose and procedures of the intervention. For future studies, we recommend that therapists spend additional time during the first few intervention sessions to explain the intervention to clients and their caregivers. More thorough explanation may increase participants’ and caregivers’ familiarity and comfort with the intervention.
Limitations
This study was a feasibility study with a single-group design. Although our findings are promising, they are preliminary, limiting the ability to draw strong conclusions about the intervention effects. We did not control for confounders such as type and frequency of rehabilitation services participants received outside the intervention. Nonetheless, our preliminary findings provide insight supporting the potential effectiveness of this intervention for Chinese adults with cognitive impairment after ABI. A randomized controlled trial that is powered to detect effects will be necessary to evaluate the efficacy of this intervention in improving participation-related outcomes. Moreover, because we used a convenience sample, the generalizability of the study may be limited. Future research should examine the feasibility of the intervention for people with ABI who have a greater range of impairments and more diverse characteristics.
Implications for Occupational Therapy Practice
This study has the following implications for occupational therapy practice:
Participation-focused strategy training is feasible and acceptable for community-dwelling adults with cognitive impairment after ABI in an Asian context.
Participation-focused strategy training may help participants achieve higher levels of performance and satisfaction in meeting their self-identified goals and improvement on multidimensional participation outcomes.
Strategy training is different from traditional treatments delivered in rehabilitation settings in Asia. Although our results support the feasibility of delivering the intervention to the target population, additional instructions and discussion among the therapist, client, and caregiver may be needed in the early stages of the intervention.
Conclusion
This study demonstrated the feasibility of delivering participation-focused strategy training to people with cognitive impairment after ABI in an Asian country. The preliminary evidence shows that participants who received the strategy training intervention had positive changes in participation outcomes and in performance of their self-identified goals. On the basis of these findings, a larger clinical trial is warranted to evaluate the efficacy of the strategy training intervention.
Footnotes
Acknowledgments
We thank research team members Yi-An Lien, Yi-Cian Lai, and Yu Su (Taipei Medical University) for their contributions. We thank our collaborating hospitals, Shuang Ho Hospital, Wan Fang Hospital, and National Taiwan University Hospital. This study was funded by Taipei Medical University–Wan Fang Hospital (106TMU-WFH-04); the Ministry of Science and Technology, Taiwan (MOST105-2628-B-038-003-MY3 and MOST108-2314-B-038-030-MY3); and the National Health Research Institutes, Taiwan (NHRI-EX108-10819PC). This study is registered with ![]() (NCT03225768). We certify that we do not have a direct interest in the results of the research supporting this study and have identified all financial support for this research.
(NCT03225768). We certify that we do not have a direct interest in the results of the research supporting this study and have identified all financial support for this research.