
Abstract
Population health is a complex construct that has been defined as “the health outcomes of a group of individuals including the distribution of outcomes within the group,” as well as the “health outcomes, patterns of health determinants, and policies and interventions that link these two” (Kindig & Stoddart, 2003, p. 380). The Health and Medicine Division of the National Academies of Sciences, Engineering, and Medicine (2019; formerly the Institute of Medicine), through its Roundtable on Population Health Improvement, added that “while not a part of the definition itself, it is understood that such population health outcomes are the product of multiple determinants of health, including medical care, public health, genetics, behaviors, social factors, and environmental factors” (National Academies of Sciences, Engineering, and Medicine, 2019, “Working Definition of Population Health,” para. 2). Improving population health is one of three pillars (along with improving the patient experience of care and reducing the per capita cost of care) of the Triple Aim, a popular framework for optimizing health system performance (Berwick et al., 2008).
Occupational therapy can play an important role in promoting the health of populations. Occupational science theorists such as Wilcock (2005) have endorsed a broad perspective of occupational therapy that goes far beyond individualistic medical models of care. In a Health Policy Perspectives article, Braveman (2016) clearly articulated a role for occupational therapy in promoting population health, noting that occupational therapists are well established in a variety of public health, community, and school agencies in which they can have an impact on a range of health outcomes. However, Braveman noted that population health is less well understood within the profession than are the other two pillars of the Triple Aim and recommended that the profession be more explicit in articulating its role in population health.
Indeed, explicit attention to population health is now apparent in the American Occupational Therapy Association’s (AOTA’s; 2017) Vision 2025, which states that “as an inclusive profession, occupational therapy maximizes health, well-being, and quality of life for all people, populations, and communities through effective solutions that facilitate participation in everyday living” (p. 1). Moreover, the five pillars of Vision 2025 speak to occupational therapy’s role in creating system-level changes that are frequently at the heart of efforts to improve population health.
Recently adopted revisions to the Accreditation Council for Occupational Therapy Education (ACOTE®; 2018) accreditation standards, which take effect in 2020, include explicit attention to population health. Whereas the 2011 ACOTE standards included population-based interventions but not the term population health, the 2018 standards include the term in several places. Standard B.4.25 on interprofessional team dynamics indicates that students will be able to “perform effectively in different team roles to plan, deliver, and evaluate patient- and population-centered care as well as population health programs” (p. 33). Standard B.6.5 on ethical policies and procedures for research requires that students be able to either understand (for master’s-degree-level programs) or design and conduct (for doctoral-degree-level programs) “ethical policies and procedures necessary to conduct human-subject research, educational research, or research related to population health” (p. 37). Finally, Standard B.7.0 includes a description of overarching professional responsibilities that encompass “client engagement, judicious health care utilization, and population health” (p. 38). These population health standards admittedly represent just a small proportion of the standards that programs must meet as of 2020. However, when coupled with the population focus of AOTA’s Vision 2025, it is clear that thoughtful action is needed to ensure that occupational therapy programs contain the population health content that will meet accreditation standards and advance the profession toward its vision.
The next several years will be ones of change for entry-level occupational therapy programs. First, they must work to integrate the 2018 standards, including those related to population health, into their curricula. Second, consistent with changing degree structures in several health professions (Seegmiller et al., 2015), many occupational therapy programs are undertaking or contemplating the curriculum revisions needed to transition to an entry-level occupational therapy doctoral (OTD) degree. Given these two forces, the time is ideal for occupational therapy faculty to more fully integrate population health concepts into entry-level occupational therapy programs. However, the extent to which population health content is currently included is not known, nor do we understand what population health content occupational therapy educators believe should be included in their programs. Therefore, we conducted a survey of occupational therapy program directors to determine the current and desired coverage of population health concepts in entry-level occupational therapy programs accredited by ACOTE.
Method
Participants
We used the listing of ACOTE-accredited entry-level occupational therapy programs, as published on the ACOTE website on January 25, 2018, to determine the population of program directors to be surveyed. Although the list included 187 separately accredited programs, at five institutions, it appeared that the same person was the director of separately accredited master’s and OTD degree programs, which reduced the population of directors to 182. Sixty program directors (33.0%) responded to the survey.
Questionnaire Development
The Clinical Prevention and Population Health (CPPH) Curriculum Framework of the Healthy People Curriculum Task Force of the Association for Prevention Teaching and Research (APTR; 2015) was the conceptual framework for the study. Developed by an interprofessional team, the CPPH framework “provides a common core of knowledge for clinical health professions about individual and population‐oriented prevention and health promotion efforts” (p. 2). Occupational therapy is mentioned in two places in the framework—once when citing accreditation standards consistent with concepts in the framework and once when providing an example of an occupational therapy capstone experience focused on influencing the environment to improve public health. The CPPH framework includes 23 content domains organized into four components (Foundations of Population Health, Clinical Preventive Services and Health Promotion, Clinical Practice and Population Health, and Health Systems and Health Policy; Table 1). Although the 23 content domains in the CPPH framework can seem daunting at first, many are related to long-standing areas of emphasis in occupational therapy educational programs (e.g., content related to evidence-based practice and individual health promotion and disease prevention activities) and are not new areas for inclusion.
Components and Domains of the Clinical Prevention and Population Health Curriculum Framework as Described on the Questionnaire
Note. Based on Clinical Prevention and Population Health Curriculum Framework, by Healthy People Curriculum Task Force, Association for Prevention Teaching and Research, 2015. Retrieved from https://www.teachpopulationhealth.org/framework-download.html. Used with permission.
As the first step in questionnaire development, we used phrases from the topic areas and illustrative examples to create a short description of each domain that we believed would be understood by occupational therapy and physical therapy educators. The questionnaire was intended for use not only in this study but also in a companion survey of physical therapy program directors. In the second step, seven physical therapy and occupational therapy program directors participated in a developmental survey to determine whether each domain description was clear enough to evaluate whether it was or should be included in an entry-level curriculum. The pilot questionnaire was completed by six physical therapy and occupational therapy program directors; on the basis of the results, minor formatting changes were made to the final version of the questionnaire.
The final questionnaire included 50 items: 1 item indicating consent; 23 items asking participants to indicate the level of current coverage in their program, with options of strong, moderate, minimal, none, or uncertain; 23 items asking participants to indicate how strongly they agreed that each domain should be included in an entry-level occupational therapy curriculum, with options of strongly agree, agree, disagree, strongly disagree, or uncertain; and 3 items about program level (master’s or OTD), geographical location, and curricular approach to population health. Table 1 shows the CPPH components and domains as they were described in the questionnaire.
Distribution
The study was approved by the institutional review board at Cleveland State University. The Qualtrics survey platform (Qualtrics, Provo, UT) was used to distribute the questionnaire to program directors by means of email. Initial email invitations were sent in mid-March 2018; three follow-up invitations were sent to nonresponders, and the survey was closed in mid-April 2018.
Data Analysis
IBM SPSS Statistics (Version 25; IBM Corp., Armonk, NY) was used for data analysis. For the degree, geographical, and curricular model items, percentages were calculated. For items regarding the current program content, responses were coded as strong (4), moderate (3), minimal (2), and none (1); items about desired content were coded as strongly agree (4), agree (3), disagree (2), and strongly disagree (1). We excluded responses of uncertain from the analysis. The gap between desired and current coverage was calculated for each respondent for each of the 23 domains by subtracting current coverage scores from desired coverage scores. Thus, a positive gap score meant that respondents’ score for the desired inclusion of the domain was stronger than that for their program’s current coverage. Means and standard deviations for desired, current, and gap scores were calculated for each domain. Because of missing or uncertain responses for some items, the number of valid responses for the current coverage items ranged from 45 to 60, for the desired coverage items from 40 to 52, and for the computed gap variables from 38 to 52.
We also summed responses across the 23 domains to calculate three different total population health scores (and their means and standard deviations) for each response with complete data: one for current coverage (n = 50), one for desired coverage (n = 34), and one for the gap between current and desired coverage (n = 30). Finally, we used the total current population health score to provide a comparison measure between master’s (n = 38) and OTD (n = 7) programs; because of the low number of OTD programs, we did not compare master’s and OTD responses statistically. Because of isolated missing data points, only 4 OTD programs were included in the total desired coverage and total gap scores, so these values are not reported by degree level.
Results
Of the 60 respondents, 45 represented master’s degree programs, 8 represented OTD programs, and 7 did not specify program type. Respondents were distributed across all geographical regions: 13.5% in the West (compared with 11.0% in the population), 25.0% in the Midwest (28.0% in the population), 38.5% in the South (30.8% in the population), and 23.1% in the Northeast (30.2% in the population). Of those who specified a curriculum model, 44.2% concentrated population health content in one or more courses, 28.8% threaded it across the curriculum, and 26.9% indicated that it was an informal element of the curriculum.
Table 2 shows the means and standard deviations for desired, current, and gap coverage items, ordered within each CPPH component so that the items with the highest average desired content are listed first. Total population health desired, current, and gap curriculum scores are given in the bottom row of Table 2. The master’s programs had a mean population health current curriculum score of 66.0 points (n = 38; SD = 9.27, range = 46–87) and the OTD programs had an average score of 69.8 points (n = 7; SD = 4.87; range = 64–79). Note that both these means are higher than the overall mean of 65.3 reported in Table 2 because the overall mean included 5 programs for which the degree level was not specified; these 5 programs had a relatively low average total current curriculum score (53.6), which pulled the overall mean below those of both the master’s and OTD programs.
Means and Standard Deviations for Desired, Current, and Gap Coverage for All Domains
Note. M = mean; SD = standard deviation.
Figures 1 and 2 present the average desired and current ratings to allow for visual analysis of the relative desired importance placed on each domain compared with the current coverage. Across 21 of the 23 domains with desired coverage of 3.0 or greater, 10 had current coverage of less than 3.0. Of these 10, the five largest gaps between current and desired coverage were in the areas of global health (Domain 3.5, gap of 0.92), population health informatics (Domain 1.6, gap of 0.81), environmental health (Domain 3.3, gap of 0.78), emergency preparedness (Domain 3.7, gap of 0.73), and organization of health systems (Domain 4.1, gap of 0.73).
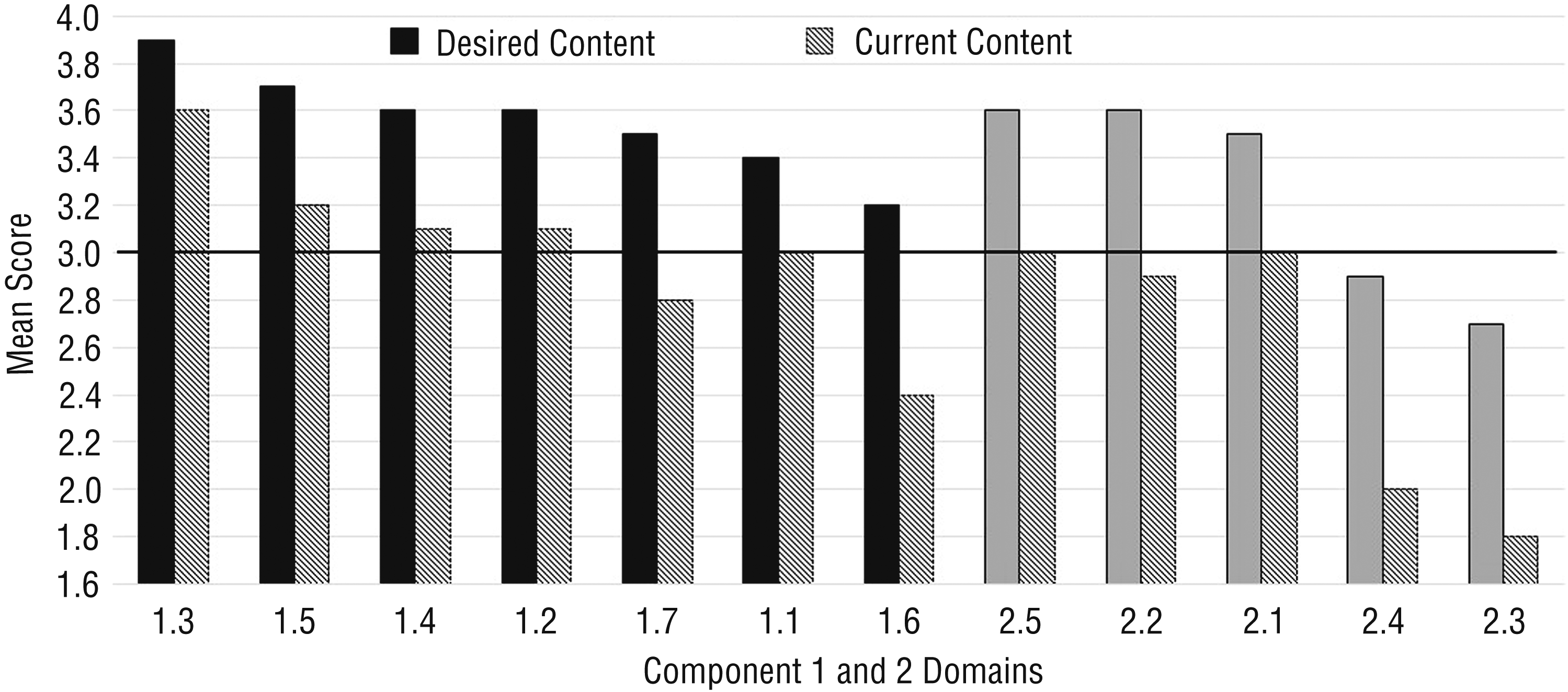
Mean values for Component 1, Foundations of Population Health (left), and Component 2, Clinical Preventive Services and Health Promotion Domains (right)
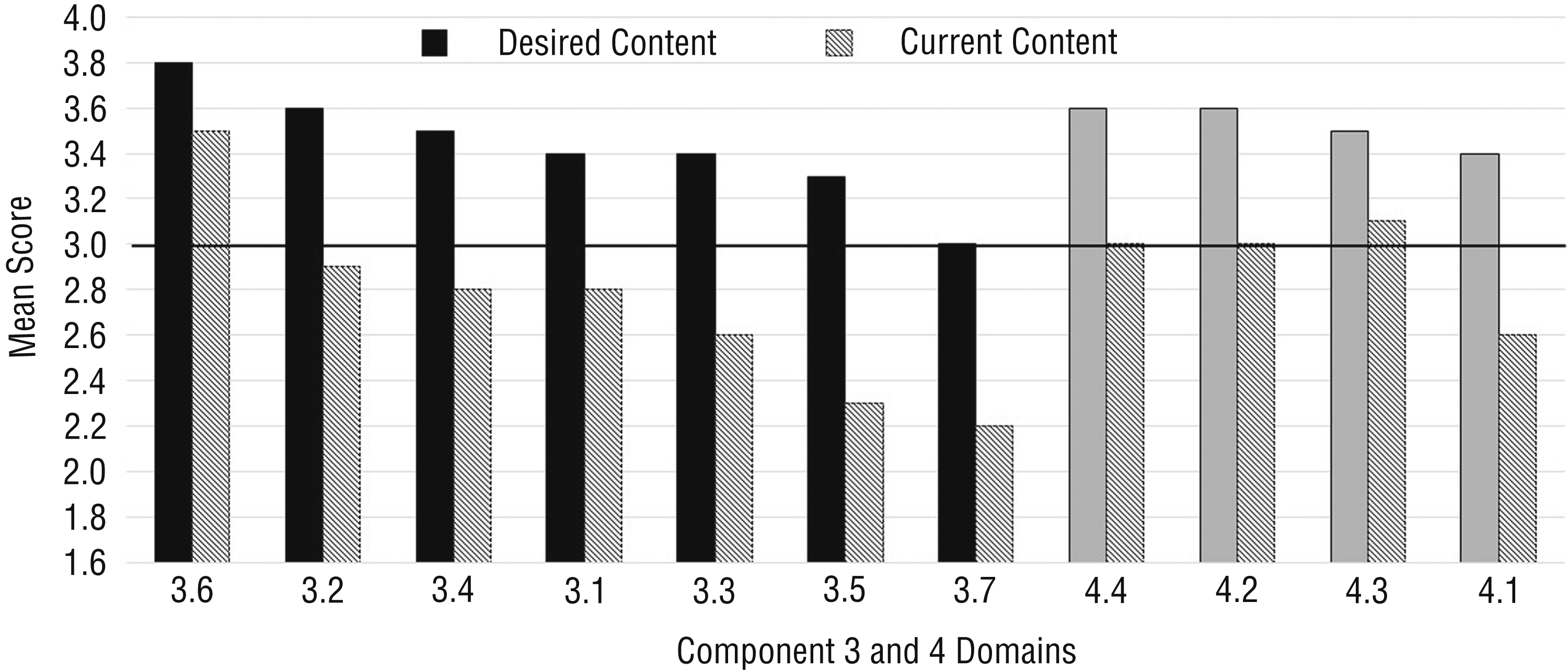
Mean values for Component 3, Clinical Practice and Population Health (left), and Component 4, Health Systems and Health Policy Domains (right)
Discussion
The occupational therapy program directors who responded to this survey generally indicated a high level of agreement that the population health content included in the CPPH framework should be included in entry-level occupational therapy curricula. Notable exceptions were preventive medication and immunizations. This high level of agreement with most of the framework domains suggests that the CPPH framework has face validity for use by occupational therapy faculty when updating the population health content of their programs.
Moreover, the occupational therapy program directors who responded to the survey indicated that, on average, many of the domains already had at least moderate inclusion in their current occupational therapy program. The framework is not exclusively about population health because it includes related foundational concepts, individual-level disease prevention and health promotion content, and health systems content. These concepts have been part of occupational therapy education and practice for some time, so it is not surprising that program directors reported good coverage, particularly in the foundations of population health and health systems and health policy components.
Our results show that the clinical practice and population health component has the most curricular coverage gaps. It is notable that this component seems to map most closely to the population-centered care that is new to the ACOTE standards. Three of the five domains (among domains with a desired coverage mean of 3.0 or more) with the largest gaps were from this component: global health issues, environmental health, and emergency preparedness. Moving forward, it will be important for occupational therapists to continue to articulate the ways in which practitioners incorporate population-based practice into their work and to further determine how to make this kind of practice come alive in the entry-level curriculum. Although emergency preparedness was identified as having one of the largest gaps, we should note that the desired coverage average for this domain was only 3.0. Given this, the current coverage of 2.2, representing an average rating of slightly more than minimal coverage, may be appropriate.
The final two domains with large gaps are population health informatics and organization of health systems. Health informatics is an emerging field, and it not surprising that programs have gaps in presenting content related to the subset of population health informatics. The health system continues to undergo rapid change in many areas, including payment models, practitioner shortages, access issues, technology and analytics, consumerism, and coordination of care (American Hospital Association, 2017). Thus, it is also not surprising that programs would identify gaps in the curriculum in this fast-changing arena. Individual programs may want to assess their own population health curricular strengths and weaknesses in light of these results to make curriculum development decisions.
We found that 27% of respondents indicated that population health was an informal element of their curriculum. Given the presence of population health in the ACOTE accreditation standards that will become effective in 2020, these programs may want to make their curricular approach to population health more formal. It will be interesting to see whether programs choose to concentrate population health content in one or more courses (as did 44% of our respondents) or whether they thread the content across the curriculum (as did the remaining 29% of our respondents).
This study has several limitations. First, the response rate of 33% was lower than desirable. However, it is within the range of norms identified by Sheehan (2001) in her review of email survey response rates. Second, only eight identified OTD programs were represented, and 7 respondents did not indicate the level of their program. Five program directors appeared to have dual responsibility for separately accredited master’s and OTD programs, but our survey design did not allow for multiple responses from the same individual; these program directors may not have participated or may be among the participants who did not indicate the level of their program. Whatever the reason, we did not have enough data from OTD programs to make meaningful comparisons between master’s and OTD programs. Third, program directors’ perceptions of population health content in their programs may not be accurate, and they may have limited familiarity with population health concepts. These two factors together may have interfered with their ability to accurately identify which population health domains are included in their programs.
Finally, several participants completed the initial survey items about their current curriculum but did not complete later items about the desired curriculum. We compared the data analysis reported in this article (using all respondents) with one in which we eliminated 8 respondents who did not complete the desired curriculum items. The current curriculum means were unchanged for 11 items and differed by only 0.1 point for the other 12 items; desired and gap means were unchanged. Because both analyses produced substantially similar conclusions, we chose to report the analysis that included the most responses.
Implications for Occupational Therapy Education
Entry-level occupational therapy programs are currently responding to changes in the degree structure of the profession and to a recent update of accreditation criteria that includes, among other things, explicit attention to population health. The results of this study may be useful to occupational therapy faculty as they respond to these changes.
The CPPH framework has face validity for occupational therapy programs and is a potentially useful framework for updating the population health content of occupational therapy programs.
Four domains in the CPPH framework with high scores for desired content and large gaps between current and desired content are potentially fruitful areas for initial curriculum development: global health issues, population health informatics, environmental health, and organization of health systems.
The substantial proportion of programs that currently take an informal curricular approach to population health may want to formalize this content, given the addition of population health to the ACOTE criteria.
Conclusion
Entry-level occupational therapy program directors who participated in this study agreed that 21 of 23 population health domains in the CPPH framework should be included in entry-level occupational therapy curricula, with 11 of the domains having at least moderate coverage in current programs. The largest gaps between desired and current coverage were in global health issues, population health informatics, environmental health, and organization of health systems. Occupational therapy faculty can use these results to develop their programs in response to changes in accreditation criteria and degree level.
Footnotes
Acknowledgments
We thank Julianne Laughlin for her participation in the initial design and analysis. This research was completed at Cleveland State University while Sarah K. Cooper and Robert J. Kleinhoff were students in the Master of Occupational Therapy program.