
Abstract
Most people with cancer have difficulties related to their functioning (Lindahl-Jacobsen et al., 2015). In this review, functioning refers to the ability to complete tasks required for activities of daily living (ADLs; Baum & Edwards, 1995), which could include self-care, instrumental activities of daily living (IADLs), work, and leisure activities. Decreased functional independence in people with cancer may be caused by cancer symptoms and treatment-related side effects or impairments (Peoples et al., 2017).
Occupational therapy practitioners working in oncology can facilitate client independence and ongoing participation in ADLs (Occupational Therapy Australia, 2015; Taylor, 2018). Occupational therapy for clients with cancer is linked to positive outcomes, including improvement and satisfaction with how they complete ADLs along with increased ability to participate in everyday tasks (Peoples et al., 2017; Pergolotti et al., 2015; Sleight & Duker, 2016; Taylor, 2018). Practitioners treat clients with cancer in various locations, including the home, palliative care settings, rehabilitation units, community-based centers, and hospitals (Longpré & Newman, 2011; Occupational Therapy Australia, 2015). In addition, practitioners provide tailored interventions to clients throughout their cancer stages, from diagnosis to posttreatment to end of life (Occupational Therapy Australia, 2015).
Rijpkema et al. (2018) reported a lack of research on oncology occupational therapy interventions and a need for further studies in this area. They specifically suggested a need for more research around the efficacy of occupational therapy in oncology in increasing ability with everyday tasks. With limited evidence currently available on occupational therapy and oncology (Sleight & Duker, 2016), this review is most valuable for occupational therapy practitioners practicing in oncology who are considering group interventions. Occupational therapy–based group interventions have been found to be valuable to patients, providing peer support and the opportunity to work together on goals (Patterson et al., 2017). Knowledge of the benefits of occupational therapy group interventions for clients with cancer could influence oncology occupational therapy practice. Therefore, the purpose of this review was to determine whether occupational therapy groups are associated with improved functional ADL outcomes for adults with cancer. Functional outcomes in this review are defined by improvement and increased engagement in ADLs.
Method
A scoping review was chosen for this study to explore all existing and accessible peer-reviewed evidence on the topic and to determine the need for further research (McKinstry et al., 2014). This review was based on the recommended structure for scoping reviews as presented by Arksey and O’Malley (2005), with an aim to provide a clear and reproducible methodology (McKinstry et al., 2014).
Determining the Research Question
In this study, the PIO (population, intervention, and outcome) structure was used for the research question (Richardson et al., 1995). The population was defined as adult inpatients and outpatients with cancer, interventions were group-based occupational therapy or ADL-based groups, and the outcome was improved functioning. On the basis of this structure, the following research question was posed: Are occupational therapy groups associated with improved functional outcomes for adult patients with cancer?
Determining the Inclusion and Exclusion Criteria and Identifying the Studies
Studies were identified and retrieved from the following databases from 1997 to 2018: MEDLINE, CINAHL, AMED, OTseeker, Health Source: Nursing/Academic Edition, and OTDBase. MeSH terms and subject headings were used when possible. OTDBase and OTseeker searches were limited manually (because of no option to automatically limit the search). Key words were defined, and a search strategy was used for each database. For instance, the CINAHL search strategy was (Occupational Therapy [Heading]) OR “occupational therap*” OR ADL OR Activities of Daily Living [Heading] OR “activit* of daily living”) AND (group OR “group therapy” OR “group intervention” OR “group program”) AND (Cancer Patients [Heading]) OR (patient or client or service user or individual) AND (cancer OR oncology OR neoplasm OR tumo#r OR malignancy) AND (function* OR independen* OR ability OR performance). The database search strategy, including search terms used and the number of articles found, is presented in Table 1. Reference lists of relevant systematic reviews in oncology occupational therapy (found in the database search) were also searched (Hunter et al., 2017; Neo et al., 2017). The reference lists of all included studies from the database search were also reviewed. This process involved manually scanning the reference lists and abstracts to identify relevant articles. All published studies meeting the following selection criteria were chosen:
• Article type: Qualitative, quantitative, and mixed-methods articles that were peer-reviewed
• Language: English
• Interventions: Occupational therapy or ADL group-based interventions (including multidisciplinary group interventions with an occupational therapy component)
• Population: Adult patients with a diagnosis of cancer.
Databases and Search Terms Used to Identify Articles Included in the Scoping Review
Note. ADL = activities of daily living.
On the basis of inclusion criteria, 34 articles were included for full text review, and CiteThisForMe (Santa Clara, CA; https://www.citethisforme.com/) was used to store the references. Figure 1 shows the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram and full search details.
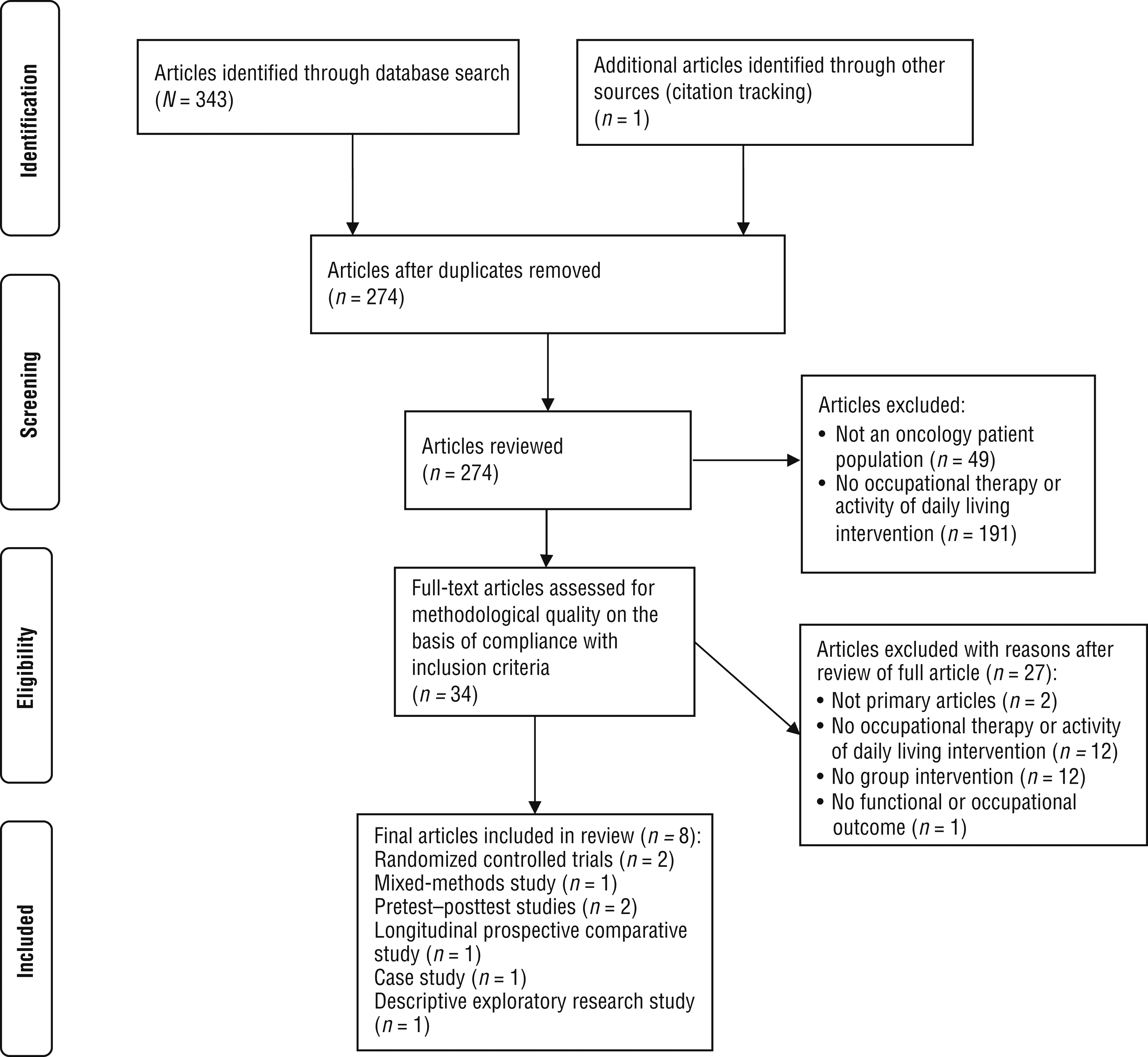
Flow diagram for inclusion and exclusion of peer-reviewed studies in the scoping review.
Charting the Data and Analysis
An evidence table was used to record key data from each article (Appendix A). This table recorded author, year, and country of publication; study design and participants (including diagnosis, group numbers, gender, diagnosis, and stage); group intervention; data collection methods (including outcome measures); results; and reported limitations. The data extraction was completed by the first author and then checked by the coauthors. Participant information from the studies was reviewed and compared by all the authors. This involved reviewing the demographic characteristics such as age, gender, sample size, as well as type and stage of cancer. The type and duration of the group interventions were also described and compared (Arksey & O’Malley, 2005). The results of occupational therapy groups with similar content (e.g., leisure-based activity groups) were reviewed together.
Results
The literature search yielded 343 articles. After duplicates (n = 69) were removed, the abstracts of 274 articles were screened for inclusion in this review. A total of 240 articles were excluded because of irrelevancy (see Figure 1). For example, some articles did not have an oncology patient population (Sackley et al., 2006), and others did not have an occupational therapy practitioner facilitating the group (Bourmaud et al., 2017). An additional article was included via citation tracking, and then 27 articles were excluded after review of the full article because they did not meet the inclusion criteria (e.g., not primary articles, did not include an occupational therapy or group intervention, presented no functional outcomes).
Study Characteristics
The articles reviewed included 2 randomized controlled trials, 1 case study, 1 descriptive exploratory research study, 1 mixed-methods study, 2 pretest–posttest studies, and 1 longitudinal prospective comparative study. The oldest study was published in 2005 (Ream et al., 2005), and the most recent studies were published in 2018 (Maher & Mendonca, 2018; Petruseviciene et al., 2018). Studies were conducted in Turkey (n = 1), Sweden (n = 1), the United States (n = 2), England (n = 2), Iceland (n = 1), and Lithuania (n = 1).
Group numbers in the studies ranged from 4 (Haltiwanger et al., 2011) to 72 (Maher & Mendonca, 2018). More than half of the studies included only female participants (n = 5), with 1 study including only male participants (Huri et al., 2015). Both studies that had male and female participants had a higher proportion of female participants than male participants. No studies compared male and female participants. Recruitment was by means of occupational therapy departments, support groups, community centers (Haltiwanger et al., 2011; Maher & Mendonca, 2018; Palmadottir, 2010; Petruseviciene et al., 2018), nurse specialist referrals (Saarik & Hartley, 2010), a palliative day program and home service (Svidén et al., 2009), and advertising (Ream et al., 2005). All groups were held in an outpatient or community-based setting. The age range of participants was 25–85 yr.
Some studies had participants with only one diagnosis, including prostate cancer (n = 1), breast cancer (n = 3), and lymphoma (n = 1). The remaining studies had a range of cancer diagnoses or did not specify the diagnosis (n = 3). The studies used different systems to indicate the cancer stage. The “T” in the TNM staging system describes the size of the tumor and any spread of cancer into nearby tissue (National Cancer Institute, 2015). In 1 study, all participants were at later cancer stages (T3 or T4; Huri et al., 2015). Although not specifically stated, it can reasonably be assumed that another study also had patients in the later cancer stages, because it was conducted in a palliative care setting (Svidén et al., 2009).
The number staging is another system, which commences at Stage 0 (presence of irregular cells) and finishes at Stage IV (a tumor that has metastasized; National Cancer Institute, 2015). In 1 study, most participants with cancer in the group (90.9%) were at an earlier cancer stage (Stages 0–II; Petruseviciene et al., 2018). The remaining studies (n = 5) did not specify participants’ cancer stage.
Interventions
All interventions described in the research articles were based in outpatient or community settings. One study did not describe the occupational therapy group provided or duration (Palmadottir, 2010). The studies made use of groups that we categorized as leisure-based activity groups, groups focusing on a range of activities, or fatigue oriented.
Leisure-Based Activity Groups
These groups were focused on activities such as art, including craft and reflective poetry (Maher & Mendonca, 2018; Svidén et al., 2009); art therapy (Petruseviciene et al., 2018); and reflection after an artistic activity (Haltiwanger et al., 2011). Other activities included dance (Maher & Mendonca, 2018) and gardening (Svidén et al., 2009); however, these were not extensively described. Socializing was a part of one group, with day trips and joint meals key features (Svidén et al., 2009). Another group had socializing in their sessions; however, it was not reported what this socialization involved (Petruseviciene et al., 2018). Group duration for the leisure activities ranged from 1 wk (Maher & Mendonca, 2018) to 6 wk (Petruseviciene et al., 2018). Length and frequency of the groups ranged from 1.50 hr once per week (Petruseviciene et al., 2018) to 4 hr per day (Maher & Mendonca, 2018). One study did not provide these details (Haltiwanger et al., 2011).
Groups Focusing on a Range of Activities
One study noted part of the group was focused on personal, leisure, and productive activities, although the specific details were not described (Huri et al., 2015). This same group had relaxation and education along with occupational therapy that was based on cognitive–behavioral therapy. No specific information was provided about these interventions. This group ran for 12 wk, with two weekly 1-hr sessions.
Fatigue-Oriented Groups
One fatigue-oriented group included three occupational therapy group sessions as well as a joint occupational therapy and physiotherapy session (Ream et al., 2005). It was not reported what the occupational therapy sessions specifically entailed. The other fatigue-based group focused on education and discussion around patients’ own fatigue goals (Saarik & Hartley, 2010). The fatigue groups ranged from 6 wk of three 150-min workshops (Ream et al., 2005) to 4 wk of weekly 2- to 3-hr sessions (Saarik & Hartley, 2010).
Measurement and Instruments
The key outcomes of the studies (considering both quantitative and qualitative designs) included occupational engagement, performance, and satisfaction; functioning; and fatigue (Huri et al., 2015; Maher & Mendonca, 2018; Petruseviciene et al., 2018; Ream et al., 2005; Saarik & Hartley, 2010; Svidén et al., 2009). Qualitative data collection methods included interviews, observations, recorded reflections, and art pieces (n = 3). Relevant study assessment methods were included in this scoping review if they had a functional component. For example, the World Health Organization Quality of Life–Brief Version (WHOQOL–BREF) has items directly related to functioning in work and ADLs (WHOQOL Group, 1995). Participants’ self-reports were used for the following quantitative data collection measures:
• Canadian Occupational Performance Measure (COPM; n = 2)
• European Organization for Research and Treatment of Cancer–Quality of Life Questionnaire–Core 30 (EORTC–QLQ–C30; n = 4)
• Engagement in Meaningful Activities Survey (EMAS; n = 1)
• Brief Fatigue Inventory (BFI; n = 1)
• 36-item Short Form Health Survey (SF–36; n = 1)
• WHOQOL–BREF (n = 1)
• Saarik and Hartley’s (2010) fatigue scale (n = 1).
Study Outcomes
Occupation-Based Outcomes
Occupation-based outcomes included occupational performance, satisfaction, and engagement. Occupational therapy group interventions led to a significant increase in self-rated occupational performance and satisfaction scores on the COPM (p < .05; Huri et al., 2015; Maher & Mendonca, 2018). The EMAS assessment also found significantly increased engagement in meaningful activities after a community occupational therapy group (Petruseviciene et al., 2018). In 1 qualitative study, the importance of engaging in an occupation for the maintenance of health as well as physical and emotional well-being was highlighted (Palmadottir, 2010). It was also suggested that occupational therapy groups provided participants with confidence in participating in valued occupations (Haltiwanger et al., 2011). For example, participating in an art-based occupation was reported as highly satisfying for a participant of one group (Haltiwanger et al., 2011). Participating in occupations also facilitated maintenance of valued roles. For example, 1 participant noted joy in being able to create art in the group (Haltiwanger et al., 2011). During the occupational therapy groups, communicating with peers undergoing similar experiences with cancer was also considered to be useful (Haltiwanger et al., 2011; Palmadottir, 2010; Ream et al., 2005).
Functioning
EORTC–QLQ–C30 scores in physical, role, social, and cognitive functioning increased after occupational therapy group interventions (Huri et al., 2015; Petruseviciene et al., 2018; Ream et al., 2005). The WHOQOL–BREF and SF–36 showed no changes in physical scores after the occupational therapy group (Maher & Mendonca, 2018). The mixed-methods study (Ream et al., 2005) noted that participants self-reported increased ability with ADLs (including shopping and work tasks) after occupational therapy fatigue group sessions, and they also reported improved sleep.
Fatigue
Three studies found a decrease in fatigue on the basis of the EORTC–QLQ–C30 and Saarik and Hartley’s (2010) fatigue scale (Petruseviciene et al., 2018; Ream et al., 2005; Saarik & Hartley, 2010). Other studies found no significant fatigue level changes on the EORTC–QLQ–C30 or BFI after an occupational therapy group (Ream et al., 2005; Svidén et al., 2009). Through the BFI, 1 study also found that fatigue interfered less with participants’ work after the occupational therapy group (Ream et al., 2005). Some studies obtained presented additional outcomes alongside functioning, including mood, emotional well-being, and anxiety levels (Ream et al., 2005; Saarik & Hartley, 2010; Svidén et al., 2009). Because these outcomes were unrelated to the research question, they were not reported for this review. Appendix A provides a summary of the key findings.
Discussion
This is the first known scoping review of oncology occupational therapy groups. This review found that oncology occupational therapy groups resulted in functional ADL improvements. These improvements included an increase in occupational performance and satisfaction (Huri et al., 2015; Maher & Mendonca, 2018) and engagement (Petruseviciene et al., 2018), along with improvements in physical and role functioning (Huri et al., 2015; Petruseviciene et al., 2018; Ream et al., 2005) and reductions in fatigue (Ream et al., 2005; Saarik & Hartley, 2010).
It has been suggested that rehabilitation for people with advanced cancer can lead to an increase in everyday independence (Barawid et al., 2015). In this scoping review, 2 studies included patients in the later stages of their cancer (Huri et al., 2015; Svidén et al., 2009). One study found no differences in functional ADL outcomes after an occupational therapy group (Svidén et al., 2009), whereas the other found that an occupational therapy group resulted in significant increases in functioning, occupational performance, and satisfaction (Huri et al., 2015). The study that found no differences was based in a palliative care day unit (Svidén et al., 2009). The goal of occupational therapy in a palliative care unit may be to maintain functioning, so an improvement in functioning would not likely be expected. Because maintenance in functioning may be a successful outcome for this group of patients, it could explain why these patients did not improve after the group therapy.
Most studies focused on leisure ADLs (n = 4). Of these, 3 studies found significant increases in occupational performance and satisfaction as well as increased participation and engagement after occupational therapy groups (Haltiwanger et al., 2011; Maher & Mendonca, 2018; Petruseviciene et al., 2018). This outcome suggests that after cancer treatment, patients wish to focus their time on ADLs that they find valuable and enjoyable, including participating in new and different leisure activities (Fleischer & Howell, 2017). It could be suggested that as people with cancer finish treatment, they have more time to pursue leisure occupations. They would also likely no longer be experiencing the side effects that some treatments have (such as fatigue), thus enhancing their ability to engage in leisure activities. It is therefore essential that occupational therapy practitioners consider the value of leisure when providing oncology group interventions.
All quantitative studies in this review used self-rated assessment tools, highlighting that the results are based on patients’ self-evaluation of their functioning. The COPM demonstrated significant occupational improvement and satisfaction after an occupational therapy oncology group (Huri et al., 2015; Maher & Mendonca, 2018). The COPM is based on the Canadian Model of Occupational Performance and Engagement, which is frequently used by occupational therapy practitioners (Townsend et al., 2007). This model highlights the ongoing interconnecting relationship among a person, his or her environment, and occupation. Because of its client-centered nature and focus on satisfaction alongside performance, the COPM is suggested for further studies on oncology occupational therapy groups. The EORTC–QLQ–C30 detected a positive functional impact along with a decrease in fatigue after occupational therapy groups (Huri et al., 2015; Petruseviciene et al., 2018; Ream et al., 2005).
However, other studies found no significant changes to overall fatigue levels after the occupational therapy group on the basis of the EORTC–QLQ–C30 and BFI measures (Ream et al., 2005; Svidén et al., 2009). Fatigue is one of the most common symptoms for people with cancer (Bower, 2005). Further research exploring the relationship between fatigue and ability with ADLs is therefore required. The EMAS found an increase in engagement after an occupational therapy group for people with cancer (Petruseviciene et al., 2018). This result highlights that a group-based occupational intervention can also achieve ADL engagement, which is an essential feature of oncology occupational therapy (Rijpkema et al., 2018).
Participants in several studies reported improved occupational engagement. The participant in the case study reported increased satisfaction after participating in meaningful occupations (Haltiwanger et al., 2011). Participants also valued being in a group setting and sharing their experiences with others (Haltiwanger et al., 2011; Palmadottir, 2010; Ream et al., 2005). After oncology occupational therapy groups, patients returned to valued occupations and achieved functional goals (Haltiwanger et al., 2011; Palmadottir, 2010; Ream et al., 2005). These are pertinent findings because they suggest that people perceive great benefits from being in an oncology occupational therapy group.
Recruitment difficulties and small sample sizes were the most frequently cited limitations in the studies (n = 5). This challenge is common to cancer studies because of patients’ changing medical conditions (Harrison-Paul & Drummond, 2006). Because of the small and heterogeneous samples of the studies, their findings were also not able to be generalized to the wider oncology population (Huri et al., 2015; Palmadottir, 2010). Most studies also included only women (n = 5) or otherwise had a female majority of participants (n = 2). This distribution can be problematic, because most cancer health services typically treat both men and women (see Appendix A for the reported limitations of each study).
We also acknowledge this review’s limitations. The studies retrieved varied significantly in study designs, participant characteristics, and group frequency and content. Because of these study variations, we were unable to compare clearly defined outcomes. Participants’ cancer stages and diagnoses also differed, and some studies omitted this information. It is recommended that these demographic details be included in future studies.
This review retrieved 8 articles, reflecting the limited existing research on this topic. Only 3 studies used a qualitative approach. Further qualitative research on oncology occupational therapy groups will provide useful and deeper insight into patients’ perceptions of how the groups meet their personal functional goals. Finally, because this was a scoping review, the quality of the articles was not analyzed.
Further research is required, exploring the usefulness and impact of oncology occupational therapy groups. It has been reported that issues with ADLs are more predominant for inpatients with cancer than for outpatients (Neo et al., 2017). Moreover, inpatients with cancer often have medical complications (such as neutropenia) requiring a long inpatient stay (Schilling et al., 2011). This finding suggests a need for future studies on oncology occupational therapy groups within the inpatient setting. It is also recommended that future studies on oncology occupational therapy groups review IADLs. In this scoping review, no studies addressed IADLs (such as household tasks, using transport, and shopping), despite half of people with cancer requiring assistance with this area (Neo et al., 2017).
Implications for Occupational Therapy Practice
The results of this scoping review have the following implications for occupational therapy practice:
• This scoping review demonstrated that occupational therapy groups in oncology lead to positive patient outcomes. These include enhanced occupational performance and engagement as well as reduction in fatigue.
• The findings from this review not only are applicable to occupational therapy practitioners in oncology-related settings but also are relevant for practitioners who work with patients with cancer in other settings, because patients with cancer are treated both in general hospitals and units as well as in cancer-specific centers (Longpré & Newman, 2011).
• Patient satisfaction is also pertinent for occupational therapy practitioners, and this review highlights that patients found value in the group setting and sharing of experiences. Findings from this review support the implementation of group-based interventions for oncology patients.
Conclusion
This scoping review found that occupational therapy groups are linked to improved functional ADL outcomes for adults with cancer. Study participants self-reported achieving improvement and gaining satisfaction through participating in valued ADLs. Enjoyment of the shared experience of a group setting was also highlighted. This review is important for occupational therapy practice because most adults with cancer experience functional ADL decline that needs to be addressed. Further research in this area is required, particularly in an inpatient oncology setting that includes all genders.
Footnotes
Appendix
Appendix A. Articles on Occupational Therapy Group Interventions in Oncology Included in the Scoping Review
| Author/Year/Country | Study Design and Participants | Group Intervention | Data Collection Methods | Results | Reported Limitations |
|
Haltiwanger et al. (2011)
United States |
Case study N = 4 women with metastatic cancer Outpatient with metastatic lymphoma (stage not stated), n = 1 (age = 57 yr) |
Weekly art-based support group; duration not stated. |
• Telephone interviews • Observations • Transcribed reflections • Artifacts • Thematic data analysis |
The group enabled participation in valued roles and occupations; sharing with others was also valued. | None stated |
|
Huri et al. (2015)
Turkey |
RCT (pretest–posttest) Male outpatients with metastatic prostate cancer, N = 34 (cancer stage: T3 or T4; participants in each stage not stated) Intervention group, n = 19 (M age = 70.89 yr) Control group, n = 15 (M age = 70.27 yr) |
OT group based on cognitive–behavioral therapy, ADL intervention, relaxation, and cancer education; duration of 12 wk, ×2 weekly 1-hr sessions |
• COPM • EORTC–QLQ–C30 • Prostate cancer component (EORTC–QLQ–PR25) |
Significant increase was found in COPM performance and satisfaction (p < .05) at final evaluation for the intervention group. No significant difference was found in COPM mean performance and satisfaction for the control group. EORTC–QLQ–C30: Intervention group showed significant improvement (p < .05) in functioning (physical, role, emotional, social) and quality-of-life scores compared with the control group. EORTC–QLQ–PR25: Sexual activity, urinary symptoms, and hormonal treatment–related symptoms were significantly lower in treatment group; control group showed no significant differences. |
Small sample size and short group duration |
|
Maher & Mendonca (2018)
United States |
One group, pretest–posttest, prospective study Female outpatients, N = 71 (ages 25 to >85 yr; 39% were ages 55–64 yr; cancer diagnosis and stage not stated) |
Activity-based OT program; duration of 1 wk, 5 days (4-hr sessions) per week |
• SF–36 • WHOQOL–BREF • COPM |
No significant differences were found pretest to 6 wk after the program for WHOQOL–BREF subscales and SF–36; COPM performance and satisfaction significantly increased (p < .001) 6 wk after the program. | Difficulty contacting participants after they left the group, retainment issues after patients left the group, length of assessments used |
|
Palmadottir (2010)
Iceland |
Descriptive exploratory study Female outpatients with breast cancer diagnosis, N = 18 (Mdn age = 53 yr; cancer stage not stated; however, all patients finished treatment) |
Nature of OT group not specified |
• Data collection: interviews • Data analysis: interviews that were qualitatively coded |
OT group led to an increase in physical and emotional health; shared discussions were also valued. | Sole author only completing data analysis, participants self-recruiting to the group |
|
Petruseviciene et al. (2018)
Lithuania |
RCT Female outpatients with breast cancer, N = 22 Community OT patients (intervention group) n = 11 (ages 18–59 yr, n = 6 [54.5%]; ages 60–80 yr, n = 5 [45.5%]; cancer stage of 0, I, or II, n = 10 [90.9%]; cancer stage of III or IV, n = 1 [9.1%]) Usual support group patients (control group), n = 11 (ages 18–59 yr, n = 5 [45.5%]; ages 60–80 yr, n = 6 [54.5%]; cancer stage of 0, I, or II, n = 7 [63.6%]; cancer stage of III or IV, n = 4 [36.4%]) |
Community OT activity group; duration of 6 wk, 1.5-hr sessions per week |
• EORTC–QLQ–C30 • Breast cancer module (EORTC–QLQ–BR23) • EMAS (community OT participants only) • OT group participants |
EORTC–QLQ–C30 and EORTC–QLQ–BR23: After 6 wk, the community OT group showed a significant increase in function compared with the control group (physical, role, cognitive, fatigue). EMAS: Increased engagement in meaningful activities was found after the community OT group (p < .05). |
Short length of group |
|
Ream et al. (2005)
England |
Mixed-methods study Female outpatients with breast cancer, N = 6 (M age = 54 yr; 5 patients with localized cancer, and 1 patient with metastatic cancer; cancer stage not stated; all patients finished treatment) |
Multidisciplinary (including OT) fatigue group; duration of 6 wk; 3 150-min workshops included ×3 OT sessions and ×1 PT and OT session |
• EORTC–QLQ–C30 • BFI • Qualitative data collection: telephone interviews with thematic data analysis |
BFI: No significant change was found in fatigue levels; less fatigue interference with work was found postgroup and 6 wk postgroup compared with pregroup. EORTC–QLQ–C30: Function (physical and social) increased and fatigue decreased from pregroup compared with postgroup and 6 wk postgroup; significance was not reported. Qualitative themes: Sharing with others was valued; own goals were achieved; and patients noted improved ADLs, community ADLs, and sleep. |
Difficulties recruiting patients |
|
Saarik & Hartley (2010)
England |
Preexperimental study, one group, pretest–posttest Outpatients, N = 28 (n = 23 women, n = 5 men; ages 37–82 yr; various cancer diagnoses; various stages; most patients were months posttreatment) |
Fatigue management OT and PT program; duration of 4 wk, weekly 2- to 3-hr sessions | Saarik and Hartley’s own fatigue-level scale ranging from 0 (no tiredness) to 10 (totally exhausted) |
• Mild fatigue ◦ Pregroup: 0% of patients ◦ Postgroup: 35% of patients • Moderate fatigue ◦ Pregroup: 65% of patients ◦ Postgroup: 59% of patients • Severe fatigue ◦ Pregroup: 35% of patients ◦ Postgroup: 6% of patients Significance was not reported. |
Difficulties recruiting patients (e.g., some patients unable to attend because of treatment the prior day) |
|
Svidén et al. (2009)
Sweden |
Longitudinal comparative descriptive study Outpatients, N = 35 (cancer diagnoses and stage not stated) Day care group, n = 23 (4 men, 19 women; age: <49 yr, n = 3; 50–69 yr, n = 16; 70–89 yr, n = 4) Comparison group (in-home palliative services only), n = 12 (2 men, 10 women; age: <49 yr, n = 1; 50–69 yr, n = 8; 70–89 yr, n = 3) |
Palliative care day program with OT-facilitated group activities; duration of 5 wk, 2–5 hr daily (frequency not stated) | EORTC–QLQ–C30 | No significant differences were found between day-program patients and in-home-service patients regarding self-reported function and symptoms as per the EORTC–QLQ–C30. | Small participant sample size |
Note. ADLs = activities of daily living; BFI = Brief Fatigue Inventory; COPM = Canadian Occupational Performance Measure; EMAS = Engagement in Meaningful Activities Survey; EORTC–QLQ–BR23 = European Organization for Research and Treatment of Cancer–Quality of Life Questionnaire–Breast Cancer; EORTC–QLQ–C30 = European Organization for Research and Treatment of Cancer–Quality of Life Questionnaire–Core 30; EORTC–QLQ–PR25 = European Organization for Research and Treatment of Cancer–Quality of Life Questionnaire–Prostate Cancer; M = mean; Mdn = median; OT = occupational therapy; PT = physiotherapy; RCT = randomized controlled trial; SF–36 = 36-item Short Form Health Survey; T3/T4 = describes the size of the tumor and any spread of cancer into nearby tissue; WHOQOL–BREF = World Health Organization Quality of Life–Brief Version.
*
Indicates studies included in the scoping review.