
Abstract
Sensory integration modalities, such as weighted blankets, are used in occupational therapy practice to assist with emotional and physical regulation (Mullen et al., 2008). A weighted blanket is a sensory modulation intervention tool that is noninvasive and self-directed (Champagne, 2010; Champagne et al., 2015). The use of weighted blankets is a form of deep pressure stimulation (DPS; Mullen et al., 2008). Encouraging evidence suggests that DPS may result in an increase in parasympathetic arousal of the autonomic nervous system and a simultaneous reduction in sympathetic arousal (Chen et al., 2016; Reynolds et al., 2015). An increase in parasympathetic arousal is thought to have a calming influence, and evidence suggests that sympathetic arousal is directly associated with emotional and other cognitive processes, including attentional control, working memory, and fluid intelligence (Chen et al., 2016; Field et al., 2010; Kimball et al., 2007; Mullen et al., 2008; Reynolds et al., 2015). Occupational therapy practitioners use DPS, including weighted blankets, as an intervention to facilitate a patient’s recovery process via increased reality orientation, soothing, distracting, encouraging engagement, and teaching coping skills and grounding techniques (Champagne, 2006; Champagne et al., 2015).
DPS encompasses different types of tactile sensory input, and it includes the use of weighted blankets for therapeutic purposes. The use of squeezing, brushing, and massage requires human application, which is not always in concert with the needs of some clients or client populations, such as victims of trauma or people on the autism spectrum (Bower & Sivers, 1998; Little et al., 2018; Riquelme et al., 2016). Although the use of DPS might be calming to some of these patient populations, others may prefer not to be touched, especially when emotionally activated. Therefore, it was deemed optimal to separate hands-on tools from those that could be used independently in creating this synthesis.
In alignment with the trauma-informed care model, sensory modulation intervention modalities, such as weighted blankets, are being recommended as humane therapeutic devices for crisis prevention and intervention and also to reduce the need for seclusion and restraint (Champagne et al., 2015; Substance Abuse and Mental Health Services Administration, 2014). Trauma-informed care, a treatment approach model that has been evolving over the past few decades, is intentional about both the psychological and the physiological effects of trauma and is being used in inpatient and outpatient mental health settings (Bowen & Murshid, 2016; Champagne et al., 2015). The trauma-informed care framework takes a holistic approach to care, integrating an understanding of the prevalence of trauma with knowledge about distinctive types of trauma and how trauma can be expressed (Greene, 2018). The idea of trauma-informed care began with the research of Dr. Vincent Felitti into adverse childhood experiences and is now heavily supported by national and government services (Damian et al., 2017; Greene, 2018). If found to be effective, weighted blankets would fit neatly within a trauma-informed care framework and speak directly to the need for alternatives to medication-based interventions for people in crisis (Champagne et al., 2015).
Compelling evidence to support the use of weighted blankets is limited, despite anecdotal support by parents, caregivers, and therapeutic staff (Champagne & Stromberg, 2004; Mullen et al., 2008). People are referred to occupational therapy practitioners to use weighted blankets for numerous clinical indications, but there are no clear guidelines or protocols for weighted blanket use within the medical and, specifically, mental health communities. The objective of this systematic review was to identify, evaluate, and synthesize this literature to help develop the impetus needed to launch a research study into the effectiveness of using weighted blankets to decrease anxiety and insomnia.
Method
This systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Moher et al., 2009). The following question guided selection of articles for the review and interpretation of the findings: What published literature currently exists related to the use and effectiveness of weighted blankets?
A broad search of the literature was conducted between January 23, 2018, and March 1, 2018. Databases and sites searched included the Cochrane Library, PubMed, PsycINFO, CINAHL, OTseeker, Web of Science, and Nursing Reference Center Plus. Search terms were developed by the first two authors, who then consulted the additional review authors with experience in completing systematic reviews. Search terms included weighted blanket, deep pressure, and occupational therapy as well as combinations of these terms. This review was limited to peer-reviewed articles published in English between January 1, 1987, and December 31, 2017. Studies were included if the intervention measured weighted blanket use as the modality of DPS. The review excluded data from presentations, conference proceedings, non–peer-reviewed literature, dissertations, and theses.
The initial search yielded 308 articles related to the research question (Figure 1). Using the references, we were able to find an additional 11 articles pertaining to the research topic for a total of 319 articles. After duplicates were removed, 298 articles remained. A systematic review of articles pertaining to weighted blankets was then conducted by the first two authors. A total of 186 articles were excluded because they were presentations, conference proceedings, not peer reviewed, dissertations, theses, or unrelated to weighted blanket use. Abstracts were filtered for inclusion and exclusion criteria with additional authors being consulted if questions regarding inclusion or exclusion criteria arose. After abstract review, 77 articles were excluded because the abstracts were unrelated to weighted blanket use. Full-text versions of potential articles were then retrieved and reviewed. After full-text review, 27 articles were excluded because they were unrelated to weighted blanket use. Overall consensus by the research team was used as the final determinant for inclusion.
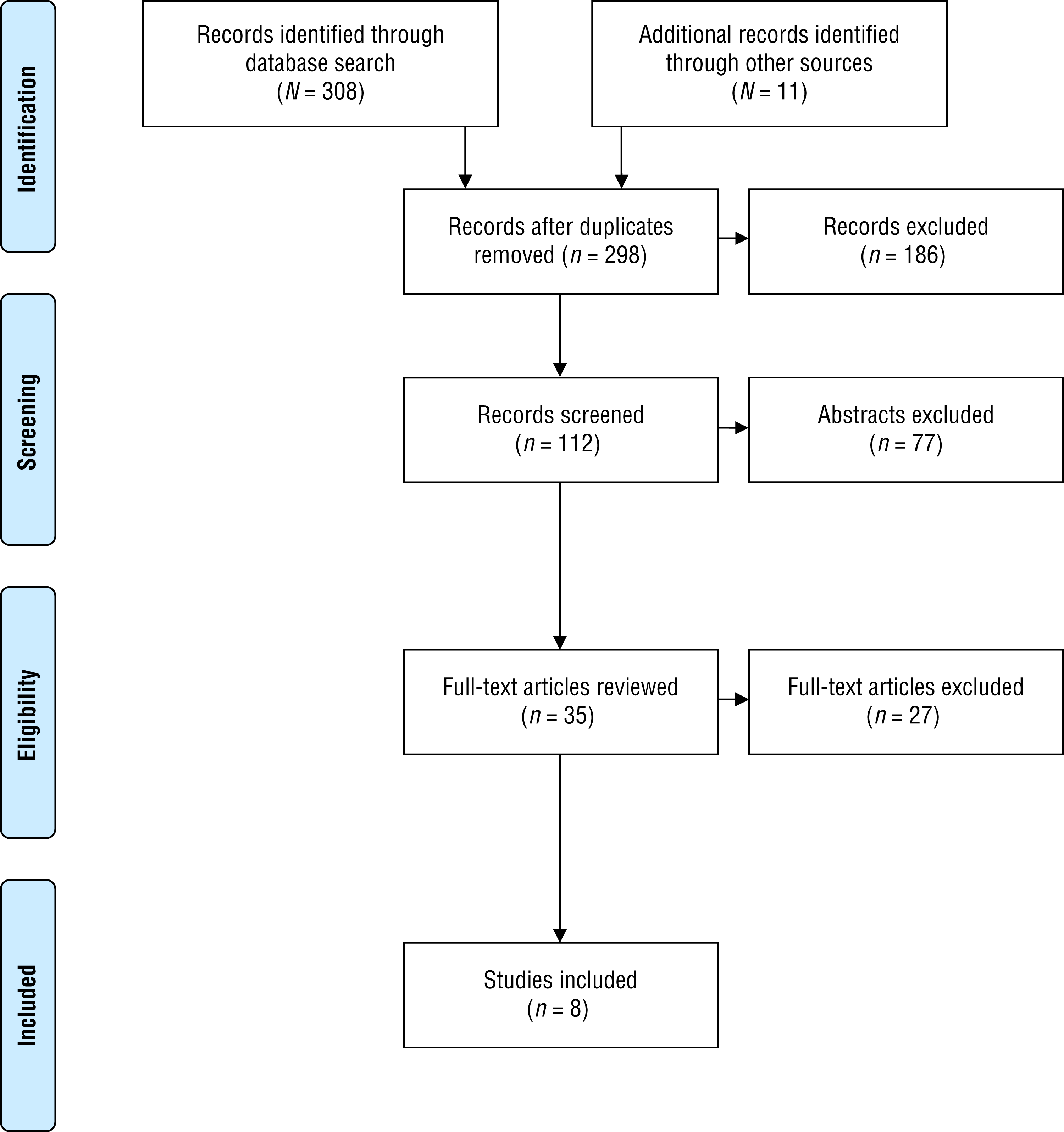
Flow diagram for inclusion and exclusion of peer-reviewed studies in the systematic review.
Analysis of study design, outcomes, and risk of bias determined level of evidence. Because of the heterogeneity of studies under review, a meta-analysis was not possible; therefore, results are presented qualitatively.
Results
This systematic review included a final count of 8 weighted blanket studies: 4 Level I studies, 2 Level III studies, and 2 Level IV studies. The articles were reviewed according to their quality, scientific rigor, risk of bias, and levels of evidence. They were then clustered into two areas of treatment and intervention: (1) anxiety and (2) insomnia and sleep disturbance. A full evidence table is provided in Appendix A (Table A.1). The Cochrane risk-of-bias guidelines were used to assess bias of individual studies (Table A.2; Higgins et al., 2011).
Anxiety
Of the 8 weighted blanket studies, 5 evaluated the use of weighted blankets for anxiety: 3 Level I studies, 1 Level III quasi-experimental study, and 1 Level IV single-subject design study (see Table A.1). Four studies found that weighted blankets decreased anxiety (Champagne et al., 2015, Level I; Chen et al., 2013, Level III; Chen et al., 2016, Level I; Mullen et al., 2008, Level I), whereas the fifth showed inconclusive results in a small sample of 3 participants (Losinski et al., 2017, Level IV). Two studies provided Level I evidence that the use of a weighted blanket is safe for adults and effective at reducing anxiety (Champagne et al., 2015; Mullen et al., 2008).
Specifically, Mullen et al. (2008) performed a feasibility study that evaluated the safety and effectiveness of weighted blanket use in 34 nonhospitalized adults with no apparent physical or medical conditions. Thirty-pound weighted blankets were used for a 5-min time frame to obtain study results. Outcome measures used for physiological safety included vital sign metrics (pulse rate, blood pressure [BP], and pulse oximetry), and those used to measure effectiveness included electrodermal activity (EDA), the 10-item State–Trait Anxiety Inventory (STAI–10), and exit survey questions. It was determined that pulse rate, BP, and pulse oximetry did not cause participants to move into an unsafe physiological range. EDA data were nonsignificant because only 33% of participants exhibited anxiety reduction through skin conductance when using a weighted blanket. Per the STAI–10, 63% of participants self-reported lower anxiety with weighted blanket use. Overall, participants felt more relaxed using the weighted blanket.
Chen et al. (2013) evaluated the effects of weighted blankets on anxiety in 15 adults undergoing dental treatment. Blanket weights were approximated up to or equal to 10% of participants’ weight. An occupational therapy practitioner then adjusted the pressure according to individual requirements. Physiological outcome measures included EDA and heart rate variability (HRV). Behavioral outcome measures included the Numeric State Anxiety Scale (NSAS) and the Dental Anxiety Scale (DAS). The results of this study indicate that the use of a weighted blanket provides DPS to modulate the activity of the parasympathetic nervous system and manage the coordination of autonomic nervous system function during stress, such as dental treatment.
Champagne et al. (2015) evaluated the safety and effectiveness of weighted blanket use in 30 adults within an acute inpatient mental health unit. The same 5-min administration time, 30-lb blanket size, and outcome measures were used as in Mullen et al.’s (2008) study. Weighted blankets were shown to be safe for 100% of participants and effective at reducing anxiety for 60% of participants, as measured by the STAI–10 and a self-report anxiety tool. Mullen et al. had found no notable link between EDA and weighted blanket use; however, Champagne et al. determined the use of weighted blankets to be 33% more effective in lowering EDA.
Chen et al. (2016) examined the use of weighted blankets for anxiety in 60 healthy adults undergoing wisdom tooth surgery. Blanket weights were calculated at 10% of participants’ weight. Outcome measures included heart rate (HR), percentage of low-frequency (LF) HRV, percentage of high-frequency (HF) HRV, and LF–HF HRV ratio. Results of this study showed an increase in HF HRV, demonstrating activated balanced sympathovagal responses, with weighted blanket use during wisdom tooth surgery. This finding indicates that DPS can increase the flexibility in and regulation of parasympathetic activity and autonomic nervous system modulation, which are associated with enhanced behavioral regulation and calming processes (Chen et al., 2013, 2016).
Losinski et al. (2017) compared the effects of two types of DPS (compression vest and 6-lb weighted blanket) with that of antecedent exercise (riding a stationary bike) on stereotypical behaviors (e.g., hand flapping, echolalia, blinking, moving fingers in front of the eyes, and rocking) of 3 students with autism spectrum disorder because stereotypical behaviors are thought to be a result of increased arousal or anxiety. Outcome measures included observational analysis. Results showed that the two types of DPS examined were largely ineffective. One of the students refused to use the weighted blanket at all; 1 student refused to use the weighted blanket on one occasion, but it reduced stereotypical behaviors slightly; and there was no change in behavior or attention for the 3rd student.
Limitations of these studies include narrow sampling methodology and small sample sizes, with the largest study having only 60 participants (Chen et al., 2016). One study was limited to only women (Chen et al., 2013) and 1 study to only boys (Losinski et al., 2017). In addition, the studies varied in their approaches to the weight of the blankets. Two of the studies used 30-lb blankets for all adult participants (Champagne et al., 2015; Mullen et al., 2008), 1 study used 6-lb blankets for all pediatric participants (Losinski et al., 2017), and the other 2 studies calibrated the blanket weights to approximately 10% of the participants’ body weights (Chen et al., 2013, 2016). All 5 studies differed in the amount of time between application of the weighted blankets and outcome measurements (e.g., EDA, HRV), ranging from 5 to 40 min (Champagne et al., 2015; Chen et al., 2013, 2016; Losinski et al., 2017; Mullen et al., 2008). A limitation of this modality, evident in the two randomized controlled trials (RCTs), is the inability to blind the intervention (Champagne et al., 2015; Chen et al., 2016).
Insomnia and Sleep Disturbance
Three of the 8 studies on weighted blanket use addressed insomnia and sleep disturbance (see Table A.1): 1 Level I RCT (Gringras et al., 2014), 1 Level III quasi-experimental study (Ackerley et al., 2015), and 1 Level IV single-subject design study (Gee et al., 2016). Two of the 3 studies found that weighted blankets decreased insomnia and sleep disturbance (Ackerley et al., 2015; Gee et al., 2016). In the Level I study, weighted blankets were not found to improve overall sleep quality; however, they were still favored by participants and subjectively contributed to better sleep (Gringras et al., 2014). Weighted blankets were found to improve sleep quality in people with insomnia, in both subjective and objective parameters, in the Level III study (Ackerley et al., 2015). The results from the Level IV study indicated that participants experienced an increase in overall quantity of sleep and a decrease in time to fall asleep (sleep latency; Gee et al., 2016). Ultimately, despite some personal preference by participants, the results regarding weighted blanket use for insomnia and sleep disturbance were inconclusive (Ackerley et al., 2015; Gee et al., 2016; Gringras et al., 2014).
Specifically, Gringras et al. (2014) conducted an RCT involving 67 pediatric participants with autism spectrum disorder. The control blankets were matched in color, size, and texture of the material to 2.25-kg or 4.5-kg weighted blankets, which were provided on the basis of the child’s size according to manufacturer and therapist recommendations. Objective outcome measures included actigraphy, specifically focusing on total sleep time (TST), sleep onset latency (SOL), and sleep efficiency. Subjective outcome measures included TST and SOL, as measured by parental sleep diary. Additional subjective outcomes included ratings by both parents and children as well as data from six questionnaires: the Composite Sleep Disturbance Index (CSDI), the Aberrant Behavior Checklist, the Sensory Behavior Questionnaire, the Children’s Sleep Habits Questionnaire, the Social Communication Questionnaire, and the Short Sensory Profile Caregiver Questionnaire. Gringras et al. determined that a weighted blanket was no more effective than a control blanket when looking at parameters of sleep, including quality and quantity; however, both parents and children supported their use.
Ackerley et al. (2015) examined the efficacy of weighted blankets in 31 men and women with chronic insomnia. Blankets were a chain-weight design in 6-kg, 8-kg, and 10-kg sizes, and participants were allowed to select the weight. Objective outcome measures included continuous actigraphy and polysomnography recordings in the participants’ own homes, and subjective outcome measures included sleep quality, environmental factors, and comments recorded in a daily sleep diary using the Karolinska Sleepiness Scale. This study determined that overall sleep time increased and movement (restless sleep) decreased with weighted blanket use. Participants indicated that they found it easier to fall asleep, enjoyed sleep more, and felt more refreshed with weighted blanket use.
Gee et al. (2016) studied the efficacy of weighted blankets for 2 children with autism spectrum disorder. Weighted blankets were calculated to be approximately 10% of participants’ body weight. Outcome measures were reported in a daily online survey completed by caregivers of each participant during the 30-day course of the study. Results of the study showed that both participants achieved a slight increase (1–3 hr) in total sleep per night and a slight decrease in time to fall asleep per night, indicating that weighted blankets can assist in improving overall sleep quality for children with autism spectrum disorder.
Limitations in the insomnia and sleep disturbance studies include narrow sampling methodology, small sample sizes, and low-level designs in 2 studies (Ackerley et al., 2015; Gee et al., 2016). The main limitation of the RCT was an inability to blind the experimental and control groups because of obvious weight differences in the blankets (Gringras et al., 2014). Because of the materials embedded in them, weighted blankets look and feel physically different than typical blankets, taking more effort to carry and manipulate. Gee et al.’s (2016) results were based on subjective assessments completed by caregivers; therefore, lack of objectivity could present an issue. Finally, in all three studies, different procedures were used to assign blanket weights to participants, which could have affected the meaning of measurable outcomes.
Discussion
The results of this systematic literature review suggest that use of the DPS modality of weighted blankets can show some success in reducing or relieving anxiety; however, the results regarding insomnia and sleep disturbance were inconclusive. Anxiety is one of the most common psychological conditions, influencing an estimated 5%–25% of the global population (Alonso et al., 2018). The impact of anxiety disorders can be devastating emotionally and physically (Alonso et al., 2018; Simpson et al., 2010). Anxiety disorders are a major cause of the burden of chronic disease and are often comorbid with other health issues (Alonso et al., 2018; El-Gabalawy et al., 2016). Psychotherapy, medication, exercise, and other tools are all used to treat anxiety disorders in both inpatient and outpatient settings (Ströhle et al., 2018). Anxiety treatment can be problematic because it needs to encompass awareness of the patient’s personal situation and preferences; practitioners also need to possess knowledge of the condition and its severity and expectations of possible treatment side effects. Therefore, any new method to address anxiety, such as the use of weighted blankets, would be invaluable (Ströhle et al., 2018).
There appears to be a close relationship between anxiety and disordered sleep that is mutually influencing, although anxiety disorders and sleep disorders are considered psychopathologically separate (Jansson & Linton, 2006). Chronic insomnia or sleep disturbance can have serious health consequences, including endocrine dysregulation, insulin resistance, behavioral disorders, and mood swings (Buysse et al., 2017). Current treatment of insomnia and sleep disturbance includes medication, exercise, psychotherapy, and natural remedies such as melatonin (Buysse et al., 2017). Estimates suggest that insomnia and sleep disturbance affect 4%–35% of the population worldwide. Hence, effective modalities to assist with providing quality sleep could substantially benefit millions of people (American Psychiatric Association, 2013; Hartescu & Morgan, 2019).
These results suggest that DPS assists in maintaining sympathovagal balance, which is the adjustment of the autonomic nervous system, by decreasing sympathetic activity while increasing parasympathetic activity (Chen et al., 2016; Field et al., 2010; Kimball et al., 2007; Reynolds et al., 2015). Research has posited that when the pressure receptors underneath the skin are activated, cortisol and skin conductance decrease and vagal tone increases (Chen et al., 2016; Field et al., 2010; Mullen et al., 2008; Reynolds et al., 2015). Increasing parasympathetic response improves symptoms associated with anxiety (Chen et al., 2016).
Implications for Occupational Therapy Practice
The results of this study have the following implications for occupational therapy practice:
Weighted blankets have the potential to be beneficial in limited settings and populations.
Although it is encouraging that individual practitioners and institutions are exploring nonpharmacological interventions to treat anxiety and sleep problems, there is an ongoing need for studies that systematically examine the effectiveness of weighted blankets and other DPS modalities across adult and pediatric populations.
Given that this systematic review revealed promising results in support of the use of weighted blankets to reduce anxiety and, to a lesser extent, insomnia and sleep disturbance, it is particularly important to further examine the usefulness of DPS across diverse adult and pediatric mental health settings.
There is emerging evidence to support the effectiveness of weighted blankets as a tool for early intervention in mental health care treatment (Champagne et al., 2015).
Safety parameters created for the use of weighted vests and backpacks have started to be applied for the use of weighted blankets (Olson & Moulton, 2004). Several researchers have offered a recommendation of a blanket weight of approximately 10% of body weight; however, definitive guidelines regarding the prescription and therapeutic use of weighted blankets have yet to be established (Chen et al., 2013, 2016; Gee et al., 2016).
Implications for Education
Given the favorable potential for the use of weighted blankets across a multitude of settings and populations, it would be beneficial for occupational therapy academic programs to work with experienced practitioners to train and educate future practitioners as experts on DPS modalities to expand the profession's clinical reach and to support implementation of occupational therapy–based and evidence-based treatment modalities. Formal education about DPS modalities across occupational therapy academic programs and collaboration with current occupational therapy practitioners with expertise in DPS modalities allow for increased inquiry, comprehension, and flexibility among practitioners to then implement these types of interventions.
Implications for Research
It is imperative, when possible, that occupational therapy practitioners strive to apply high levels of research and evidence-based practice in daily routines. Although extensive anecdotal support for weighted blanket use exists from parents, caregivers, and therapeutic staff, especially in regard to children with autism, this evidence is not yet robust enough to justify the widespread implementation of this DPS modality (Champagne & Stromberg, 2004; Mullen et al., 2008). Higher levels of evidence are needed in many areas of occupational therapy, and the use of weighted blankets is one of those areas. The strongest research design possible should be applied to optimally evaluate the effectiveness of this intervention. Only four studies gathered for this review were high-quality, rigorous Level I studies (Champagne et al., 2015; Chen et al., 2016; Gringras et al., 2014; Mullen et al., 2008). The remaining studies were Levels III and IV, indicating a need for higher levels of research in regard to the effectiveness of weighted blankets (Ackerley et al., 2015; Chen et al., 2013; Gee et al., 2016; Losinski et al., 2017). Research designs with relatively low levels of evidence severely limit confidence in study findings.
The small number of studies ultimately deemed acceptable for this systematic review illustrates the limited research in the field of occupational therapy related to DPS through the use of weighted blankets. Of these studies, many were conducted by the same researchers and on similar populations. Many weighted blanket studies are geared toward populations with autism spectrum disorder (Edelson et al., 1999; Gee et al., 2016; Grandin, 1992; Gringras et al., 2014). Although it is important to focus efforts on this population, especially as they relate to sensory-based interventions, weighted blanket use has been left unexplored within many other populations, including people with attention deficit hyperactivity disorder, bipolar spectrum disorders, and eating disorders. Occupational therapy practitioners need to expand on and explore other possible populations that have the potential to benefit from DPS through weighted blanket intervention.
Moreover, a more cohesive protocol needs to be derived for the appropriate use of weighted blankets. Lack of a consistent protocol may lead to studies that are difficult to translate into a clinical setting. To establish guidelines and protocols, researchers and practitioners need to gain a further understanding of the mechanism of action underlying the use of weighted blankets. Although the literature supports the use of weighted blankets for anxiety reduction, there is no agreement concerning systematic consultation, application, and measurement (Chen et al., 2013). Additional research is required to gain a neuroscientific and biological understanding of how DPS works to calm the body and increase parasympathetic tone (Chen et al., 2016).
The evidence regarding the use of weighted blankets for insomnia and sleep disturbance is inconclusive. This issue stems, in part, from the considerable variety of ways used to measure sleep, including quality, quantity, number of interruptions, and time to fall asleep (Ackerley et al., 2015; Gee et al., 2016; Gringras et al., 2014). In addition, numerous tools were used to measure sleep, such as actigraphy, comprehensive polysomnography recordings, the KSS, and the CSDI (Ackerley et al., 2015; Gee et al., 2016; Gringras et al., 2014). Although the comprehensive results regarding the use of weighted blankets for anxiety showed that it was an effective intervention, it was not possible to compare outcome measures. As with sleep, several tools were used to measure emotional state, including EDA, HRV, the NSAS, the DAS, stereotypical behavior, attention to task, BP, pulse rate, pulse oximetry, and the STAI–10 (Champagne et al., 2015; Chen et al., 2013, 2016; Losinski et al., 2017; Mullen et al., 2008). The ability to compare research designs with different scales of measurement is limited.
Strengths and Limitations
The strengths of this systematic review include consistency with the PRISMA guidelines (Moher et al., 2009) for conducting searches and refining the results, consultation with qualified researchers experienced in conducting systematic reviews, and the use of well-described definitions for weighted blanket and deep pressure. The low level of some of the included studies limited the ability to report results in accordance with the full PRISMA guidelines.
Conducting a synthesis did not overcome any limitations that were inherent in the design and execution of the primary studies (Munthe-Kaas et al., 2018). This synthesis resulted in the review of only eight studies, which is a limited amount of data. Given that 11 additional records were originally identified (but ultimately excluded) through other sources, there is the possibility that other studies related to this topic failed to be identified. The grouping of studies required some subjectivity, but the aggregated effect of these groups may change the impact of the original intent of the study, data, or outcomes.
Conclusion
Credible research suggests that weighted blankets may be an appropriate therapeutic tool. The intervention was reviewed for use in relieving anxiety and insomnia symptoms, and it was found to demonstrate some success in reducing anxiety; however, the results pertaining to sleep were inconclusive. Further research is necessary to define rigorous guidelines for the use of weighted blankets within clinical practice and to further investigate the underlying mechanism of action. In addition, investigation of the use of weighted blankets for larger and more diversified populations remains uncharted territory, requiring further structured and focused study.
Footnotes
Acknowledgments
We acknowledge Figaro Loresto, Jr., Sonia Napravnik, and Mary Beth Makic for their guidance throughout this process.
Appendix
*
Indicates studies that were systematically reviewed for this article.