
Abstract
About 50 million people worldwide are living with dementia (World Health Organization [WHO], 2019). Dementia can take many forms; the most common types are Alzheimer’s disease, frontotemporal dementia, vascular dementia, and dementia with Lewy bodies (Dementia Care Central, 2018). All types of dementia are characterized by progressive loss of cognitive function, including changes in memory, judgment, reasoning, language, learning capacity, and orientation. Loss of cognitive function can greatly affect a person’s ability to problem solve, communicate, and perform activities of daily living, and it can often lead to dependence on others for care. Dementia has a considerable impact on caregivers and society at large. In 2015, the total societal cost of dementia care worldwide was estimated to be $818 billion, which is 1.1% of global gross domestic product (WHO, 2019).
Efforts to address the need for more cost-effective and improved dementia care have primarily been characterized by the development of pharmacological therapies (Burgener et al., 2015). A review of the effectiveness of the five U.S. Food and Drug Administration–approved medications for the treatment of dementia, known as cholinesterase inhibitors, revealed that medications provided only clinically marginal improvement in cognition (Raina et al., 2008). A patient with Alzheimer’s pays, on average, $3,000 per year for prescription drugs, in part because many people with Alzheimer’s have comorbid conditions (Stringfellow, 2018). With the steep price of medications, many of which may have only minor positive effects, a considerable need exists for more cost-effective and evidence-based interventions. In this article, we explore and describe a nonpharmacological approach to intervention that may prove beneficial for expanding occupational therapy practice and improving health outcomes for people living with dementia.
In the past 15 yr, many researchers have begun to investigate the effectiveness of nonpharmacological interventions such as cognitive stimulation, exercise, and mind–body practices for people with cognitive impairments (Burgener et al., 2015; Gaylord & Crotty, 2002; Horowitz, 2006). Research suggests that physical and mental exercise can preserve brain plasticity and prevent cognitive decline through various neurological mechanisms, such as increased cerebral blood flow (Horowitz, 2006). Nonpharmacological therapies with the strongest evidence for improving cognitive functioning include cognitive training, exercise, and music, whereas meditation, social engagement, and biofield therapies have moderate evidence supporting their effectiveness (Burgener et al., 2015). Much of the research has focused on the protective effect of nonpharmacological therapies against the development of pathological cognitive decline (Khalsa, 2012; Wells et al., 2013). Little evidence currently exists for whether these interventions can have positive effects on people who already have mild to severe dementia, which is an area of research this scoping review addresses.
One nonpharmacological therapy that has received particular attention in the health sciences field in the past 20 yr is meditation (Van Dam et al., 2018). Meditation involves turning one’s attention to a single object, thought, or bodily sensation (“Meditation,” n.d.). Common types of meditation include mindfulness, transcendental meditation, and guided visualization, all of which require focusing the mind on a single point of reference. Researchers investigating the effects of meditation on brain function and cognition have suggested that meditation practice contributes to improvement in memory, attention, executive function, and processing speed (Gard et al., 2014). Meditation has also been linked to stress reduction, including improvement in anxiety, depression, and pain (Goyal et al., 2014). The morphological brain changes that likely underlie these improvements include alterations in the hippocampus, anterior cingulate, and insula, which are the areas of the brain involved in memory, emotional regulation, and body awareness (Fox et al., 2014). Given the positive brain changes associated with meditation, an investigation of how these changes can positively affect people with cognitive decline is warranted. Meditation is also considered a cost-effective treatment that requires little to no equipment to administer (Khalsa, 2012).
Meditation-based interventions align with occupational therapy’s emphasis on holistic health and fall directly under occupational therapy’s scope of practice (American Occupational Therapy Association, 2014). Research indicates that mindfulness may have the potential to improve occupational engagement and provide the foundation for optimal experience of occupation (Elliot, 2011). Occupational therapy practitioners have begun to embrace meditation-based interventions in physical rehabilitation and mental health settings with positive results (Bormann, 2018; Hardison & Roll, 2016). Given the benefits of meditation for people with a wide variety of symptoms and diagnoses, it is worth investigating its usefulness with older adults with dementia. The purpose of this scoping review was to synthesize the available research on meditation-based interventions for people with dementia and to investigate the ways in which these interventions influence various aspects of quality of life (QOL) and health.
Method
The methodology framework proposed by Arksey and O’Malley (2005), which is a methodology recommended for research in the field of occupational therapy (McKinstry et al., 2014), was used to conduct this scoping review. A scoping review, which is useful for investigating topics for which strong evidence is lacking, was selected as the most appropriate methodology for this study because it allows for the incorporation of gray literature such as theses and dissertations. The following steps were taken: (1) identify a research question, (2) search for relevant studies, (3) select studies to be included in the review, (4) analyze the findings and identify gaps in the literature, and (5) summarize and report those findings.
The literature search attempted to answer the following question: “How do meditation-based interventions affect health and QOL outcomes for adults with dementia?” Searches were conducted of the following electronic databases: PubMed, CINAHL, Embase, Cochrane, and JumboSearch at Tufts University. Search terms included meditation, mindfulness, mind–body, dementia, and Alzheimer’s. Titles and abstracts of articles were screened for review, with at least two authors reviewing each abstract. Only articles that mentioned meditation, mindfulness, or mind–body therapies in addition to mentioning either dementia or Alzheimer’s were further reviewed.
We used the following inclusion criteria to determine final eligibility: (1) The article included at least one participant with early-stage dementia of any form, including Alzheimer’s disease; (2) the article included discussion of a meditation-based intervention or mindfulness practice; (3) the article was written in English or an English translation was available; and (4) the publication was a peer-reviewed article, non–peer-reviewed article, or doctoral thesis published between 1997 and 2018. We excluded articles using the following criteria: (1) The article did not exclusively include participants with subjective cognitive decline or mild cognitive impairment and (2) the article did not cover the use of meditation-based interventions for prevention of dementia.
All studies were reviewed by at least two different authors. Disagreements about the eligibility of a study were discussed as a group to reach consensus regarding final eligibility for inclusion. After the final set of eligible studies was determined, data extraction was performed. Initially, each author reviewed one-quarter of the selected articles and extracted basic findings. After basic findings were recorded, a second author cross-checked findings specific to one of four primary outcomes that emerged in the research. A reference chart created in Google Sheets was used to manage study selection and to record basic findings. The study selection process is shown in Figure 1.
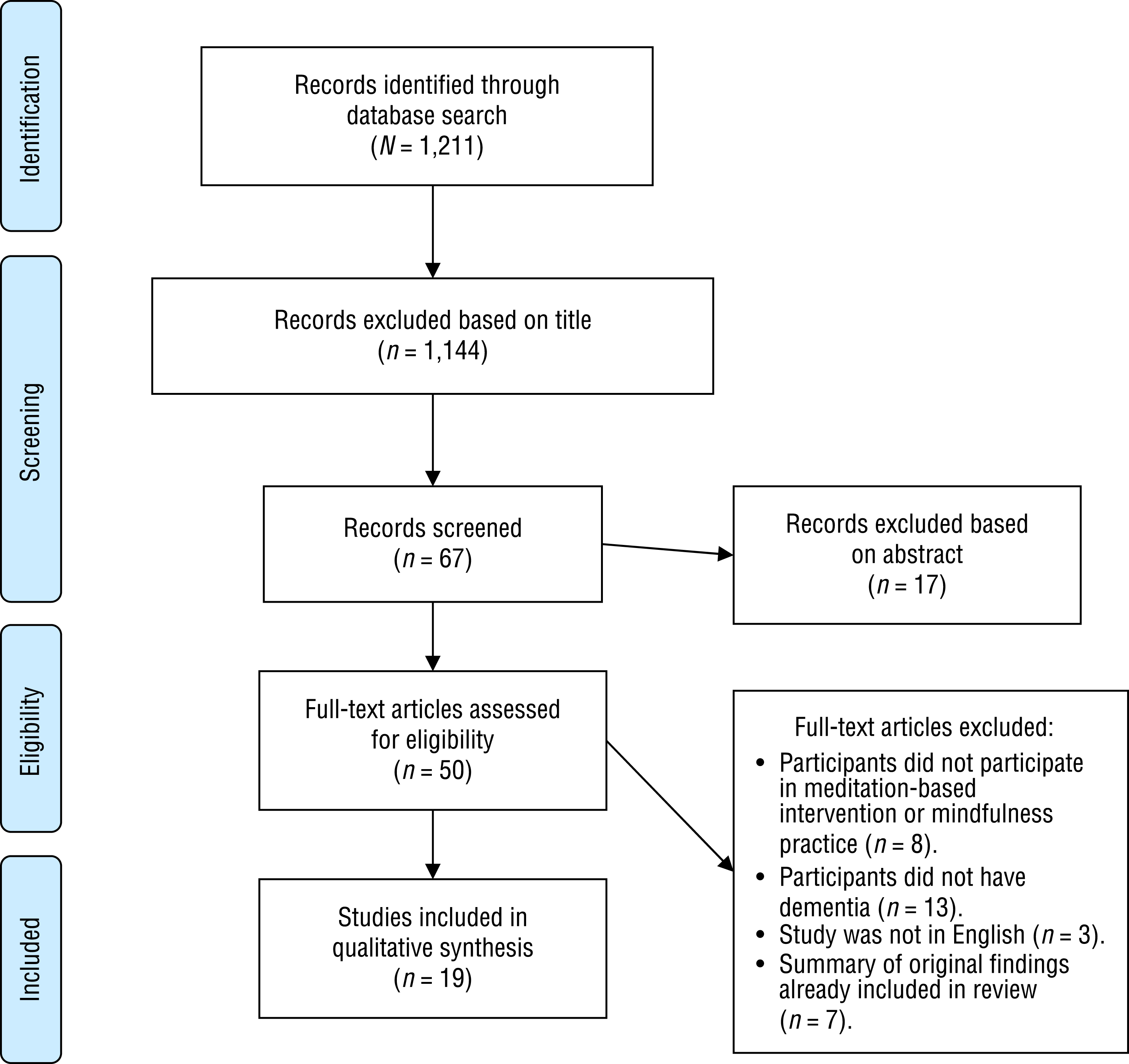
Flow diagram for inclusion and exclusion of peer-reviewed studies in the scoping review.
Results
The initial database search resulted in 1,211 articles. After screening and excluding articles on the basis of title and abstract, 50 full-text articles were assessed. Of these 50 articles, 19 met the inclusion criteria. Articles for further analysis included 11 peer-reviewed research studies with original findings, 1 program review, 1 study protocol description, 1 program manual, 3 literature reviews, and 2 doctoral dissertations. Four main outcomes of participation in meditation-based interventions emerged from the research, including improvement in QOL, mental health, cognitive-related functions, and functional abilities (Figure 2). The 11 empirical studies had variable research designs, participant demographics, measures, interventions, and outcomes (Appendix A).
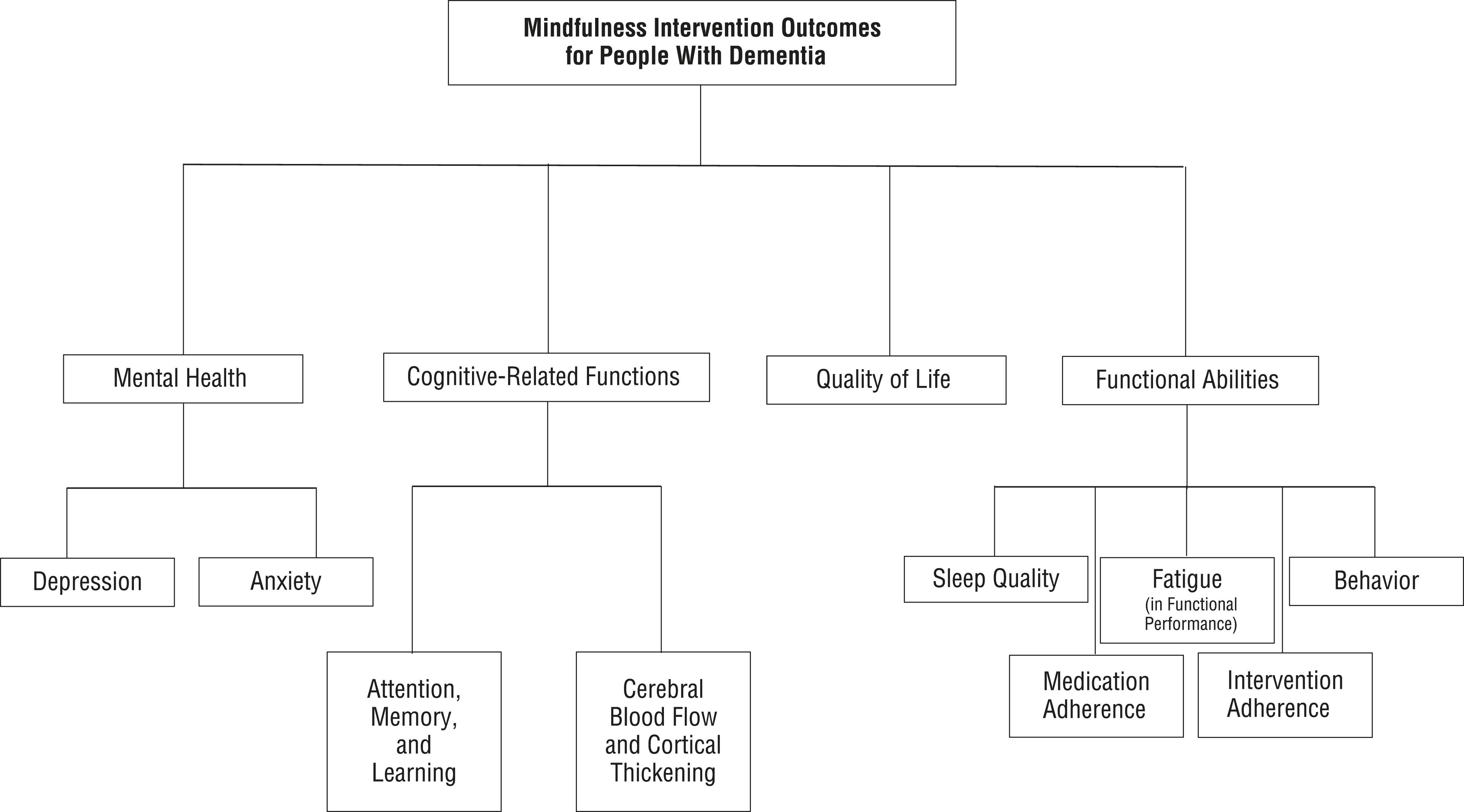
Four main outcomes of meditation-based interventions for participants with dementia: Improvement in quality of life, mental health, cognitive-related functions, and functional abilities.
Quality of Life
Of the 19 articles included in this scoping review, 7 discussed QOL outcomes. Of these 7 studies, all but 2 used the Quality of Life–Alzheimer’s Disease (QoL–AD) scales to measure changes in QOL (Aguirre et al., 2017; Chan et al., 2017; Churcher Clarke et al., 2017; Paller et al., 2015; Payne, 2017). This instrument contains 13 items pertaining to mood, energy, physical health, fun, friends, self, and life in general, which the participant rates on a 4-point Likert scale (Churcher Clarke et al., 2017; Paller et al., 2015). A maximum score of 52 points can be obtained on this measure, with higher scores corresponding to perceived higher QOL. This measure has been demonstrated to have good internal consistency and interrater reliability, and it is the preferred method for measuring QOL in people with dementia (Payne, 2017). One study assessed QOL with the Warwick–Edinburgh Mental Well-Being Scale, a 14-item assessment that requires participants to rate statements pertaining to positive mental health (Litherland & Robertson, 2014). Another study did not mention any specific standardized measures of QOL but reported changes in pain control, coping, emotional regulation, sense of self, and interpersonal relationships (Robertson, 2015).
Five articles discussed improvement in QOL as a result of meditation-based intervention. Two of these articles, an empirical study and the program manual for that study, pertained to a pilot study examining the effects of a 5-wk adapted mindfulness program and reported a significant positive change in QOL from baseline to postintervention as measured by the QoL–AD (Chan et al., 2017; Churcher Clarke et al., 2017). These articles also revealed a significant difference between treatment and control groups over time.
Another empirical study, conducted by Paller et al. (2015), also reported improvements in scores on the QoL–AD after participation in an adapted mindfulness program. The scores of participants in the intervention group increased, on average, by 2.1 points from pre- to posttesting on the QoL–AD. In addition, postintervention interviews revealed that 69% of participants felt less stressed than they did at the beginning of the program, 50% reported improvement in their relationships, and 75% reported increased ability to cope.
Litherland and Robertson (2014) researched the effects of an 8-wk mindfulness-based stress reduction (MBSR) course and found improved scores on the Warwick–Edinburgh Mental Well-Being Scale from pre- to postintervention. Robertson (2015) discussed this study in a literature review and further reported QOL benefits, including reduced anxiety as well as improved coping, emotional regulation, sense of self, and interpersonal relationships.
One empirical study, which was discussed in 2 of the 7 articles examining QOL outcomes, involved a pilot randomized controlled trial of an 8-wk adapted mindfulness-based cognitive therapy (MBCT) program for people with early-stage dementia (Aguirre et al., 2017; Payne, 2017). Participants in the intervention group did not have significant changes in QoL–AD scores from pre- to posttesting (Payne, 2017). Payne (2017) suggested that this finding may be because of the small sample size and because the QoL–AD is not very sensitive to change.
Mental Health
Many of the included studies examined the relationship between mindfulness interventions and participants’ mental health status with varied conclusions. Three empirical studies concluded that their interventions did not correlate with statistically significant improvement in depression or anxiety compared with control groups (Churcher Clarke et al., 2017; Moss et al., 2012; Noone, 2017). Only 1 of these studies included depression as an inclusion criterion for the study (Noone, 2017). Although Moss et al. (2012) did not find mindfulness interventions to correlate with specific improvement in anxiety or depression, they noted significant improvement in participants’ experiences of tension and fatigue and reported significant correlations between changes in baseline cerebral blood flow and changes in mood state.
Two other studies found that symptoms of depression and anxiety did improve to varying degrees for the participants in their interventions (Hanson et al., 2017; Paller et al., 2015). However, the results of Paller et al.’s (2015) study do not purely reflect changes in mental health for people with dementia because caregivers were included in the sample population. In addition, Paller et al. did not specifically use measures designed for people with dementia but rather used the Geriatric Depression Scale with all participants as a focal measure. In the other study, Hanson et al. (2017) noted that, in addition to decreased depression and anxiety, participants with Alzheimer’s disease additionally experienced increased feelings of serenity, improved emotional health, and decreased feelings of stress.
Six studies quantified participants’ mental health scores of depression, anxiety, or mood state through formal measures (Aguirre et al., 2017; Churcher Clarke et al., 2017; Lima et al., 2016; Moss et al., 2012; Noone, 2017; Paller et al., 2015). One study, however, included a discussion of how mindfulness interventions affected participants’ mental health through qualitative participant reporting of reduced anxiety (Litherland & Robertson, 2014). Of the studies examined, only 1 completed study had depression as part of the inclusion criteria (Noone, 2017).
Cognition
Of the articles included in the review, 13 included cognitive impairment as an area of interest (Aguirre et al., 2017; Anderson et al., 2017; Chan et al., 2017; Churcher Clarke et al., 2017; Lima et al., 2016; Marciniak et al., 2014; Moss et al., 2012; Newberg et al., 2010; Paller et al., 2015; Park, 2015; Payne, 2017; Quintana-Hernández et al., 2016; Robertson, 2015). Of the 13 articles, 6 were empirical studies that measured changes in cognition for patients with dementia after a meditation or mindfulness-based intervention (Aguirre et al., 2017; Churcher Clarke et al., 2017; Moss et al., 2012; Paller et al., 2015; Park, 2015; Quintana-Hernández et al., 2016). Of the 6 empirical studies, 3 studies reported no significant improvement in cognitive function after the intervention (Aguirre et al., 2017; Churcher Clarke et al., 2017; Paller et al., 2015), and 3 studies reported improvement or maintenance of cognitive-related functions (Moss et al., 2012; Park, 2015; Quintana-Hernández et al., 2016).
Seven studies measured neuropsychological elements of cognition, such as memory, attention, and learning. Two studies measured changes in cerebral blood flow, a cognitive-related function, through single-photon emission computerized tomography (Moss et al., 2012; Newberg et al., 2010). The included studies used many different neuropsychological measures to measure cognitive changes. Only 2 articles (Moss et al., 2012; Paller et al., 2015) shared the same outcome measure: Trail Making Test, Parts A and B. In addition to the Trail Making Test, Paller et al. (2015) also used the Repeatable Battery for the Assessment of Neuropsychological Status to evaluate changes in cognition. The other studies used various other measures. Churcher Clarke et al. (2017) used the Mini-Mental State Examination. Quintana-Hernández et al. (2016) used the Cambridge Mental Disorders of the Elderly Examination–Revised (CAMDEX–R). Aguirre et al. (2017) used the Cognitive and Affective Mindfulness Scale–Revised. Park (2015) used four measures, none of which were included in a systematic review of recommended measures for cognitive assessment of patients with dementia (Bossers et al., 2012).
Functional Abilities
Eleven of the articles examined the relationship between meditation-based interventions and functional abilities in people with dementia. Functional abilities included sleep quality, fatigue level, behavior, medication adherence, and intervention adherence (Anderson et al., 2017; Churcher Clarke et al., 2017; Innes et al., 2012; Lima et al., 2016; Litherland & Robertson, 2014; Marciniak et al., 2014; McBee, 2003; Moss et al., 2012; Paller et al., 2015, Robertson, 2015; Wilson et al., 1997). Three of the 11 articles discussed whether mindfulness techniques enhanced sleep quality (Anderson et al., 2017; Innes et al., 2012; Paller et al., 2015). One study found a statistically significant improvement in perceived sleep quality (Innes et al., 2012). Another study assessed sleep quality with the Pittsburgh Sleep Quality Inventory and reported 40% improvement in sleep quality among participants with Alzheimer’s disease in the intervention group (Paller et al., 2015). Fatigue level was assessed in 1 empirical study, which was discussed in 2 of the 11 articles (Marciniak et al., 2014; Moss et al., 2012). Participants in the intervention group had trend improvements in the fatigue categories of the Profile of Mood States compared with participants in a music listening group (Moss et al., 2012).
Studies also evaluated the role that meditation techniques play in the reduction of agitated behaviors. Two studies reported a reduction in disruptive behavior after participation in a meditation program that focused on calming and promoting a sense of self (McBee, 2003; Wilson et al., 1997). Both studies evaluated meditation programs in nursing homes with a small group of older adult residents with dementia. McBee (2003) also stated that the nursing home staff reported a decrease in behavioral problems, and a statistically significant reduction in agitation, measured by the Cohen–Mansfield Agitation Inventory, was reported.
The remaining 3 articles discussed other outcomes related to functional abilities, including medication adherence, intervention adherence, and restoration of general functional abilities. Lima et al. (2016) addressed the relationship between mindfulness and medication adherence using the Medication Adherence Report Scale. Results indicated that meditation held a mediator role between disease awareness and medication adherence in patients with mild Alzheimer’s disease by allowing the person to focus on the present moment. Meditation fostered a sense of awareness of the negative consequences of disease, which allowed the patient to prioritize medication use. Two articles evaluated the ability of people with dementia to participate in meditation-based groups by measuring intervention adherence of clients with dementia attending mindfulness programs (Churcher Clarke et al., 2017; Litherland & Robertson, 2014). Churcher Clarke et al. (2017) reported a mean attendance of 8.15 sessions (standard deviation = 2.46, range = 1–10) for their meditation intervention group sessions; however, a low level of compliance during home practice was found. Litherland and Robertson (2014) found that MBSR helped with the restoration of functional abilities such as cooking and leisure engagement as reported by participants during semistructured interviews (for a complete listing of findings, see Appendix A).
Discussion
Despite the high prevalence of dementia and the boom in mindfulness research in health care, few studies have examined meditation-based interventions for people currently living with dementia. Moreover, most of the research that does exist in this area has focused on meditation’s role in caregiver well-being or prevention of dementia. While reviewing the literature for this scoping review, we identified many studies pertaining to meditation and mindfulness programs for caregivers of people with dementia. Researchers are interested in the many potential benefits of mindfulness to reduce stress in caregivers, most of whom tend to experience high levels of stress (Liu et al., 2017). In addition, much of the research exploring the effects of meditation-based interventions on dementia have primarily focused on prevention of cognitive decline. Numerous studies that appeared in initial database searches had investigated meditation-based interventions for people with mild cognitive impairment. Despite the limited amount of research pertaining to meditation interventions for people currently living with dementia, findings indicate many probable benefits of meditation for this population.
The findings from this scoping review suggest that meditation-based interventions can have positive effects on the QOL, mental health, cognition, and functional abilities of people with dementia. However, more rigorous research is warranted to validate these findings. Moderate evidence supports QOL benefits of meditation-based interventions for people with dementia. The significant improvements in QOL reported by Churcher Clarke et al. (2017) indicate promising QOL benefits for people with dementia who undertake mindfulness practices, especially considering the study’s use of randomization, control participants, a manualized adapted mindfulness program, and valid instruments. However, the small sample size makes findings ungeneralizable, so further research is needed to validate these findings.
Mental health benefits of meditation are supported by minimal levels of research, with only one study reporting significant improvement in depression (Hanson et al., 2017). This study used a quasi-experimental design, which limits the validity of these findings. Other studies reported nonquantifiable changes in depression-like symptoms on the basis of subjective participant reports (Litherland & Robertson, 2014; McBee, 2003; Wilson et al., 1997), indicating that meditation may affect mood. Because only one study researching meditation’s effect on mental health required that participants meet diagnostic criteria for depression (Aguirre et al., 2017), little can be concluded about relationships between mental health outcomes and meditation-based interventions.
Improvement or maintenance of cognitive functions through meditation is the most strongly supported outcome. The majority of articles included in this review discussed cognitive benefits of meditation for people with dementia. The most rigorously designed study in this review, a randomized controlled trial with 502 participants, reported the maintenance of cognitive functions in people with dementia over a 2-yr period (Quintana-Hernández et al., 2016). All cognitive abilities, as measured by the CAMDEX–R (a measure of memory, comprehension, attention, orientation, praxis, calculation, and abstract thinking), were maintained in the mindfulness-based Alzheimer’s stimulation group but declined in the progressive muscle relaxation group and control group. This finding indicates that meditation-based interventions are effective for maintaining cognitive function in people living with dementia.
The evidence supporting improved functional abilities is highly variable. Of the five areas of functional abilities assessed in this review, the area with the most support was sleep quality. Two empirical studies examined the relationship between meditation and sleep quality, and one found statistically significant changes in sleep quality after an 8-wk meditation intervention (Innes et al., 2012). Improvement in other functional abilities, including medication adherence, intervention adherence, behavior, and fatigue level as a result of meditation practice, have little support. On the basis of all the findings included in this review, meditation-based interventions are likely to improve QOL and maintain cognitive functions of people with dementia. Further research is warranted, and professionals using meditation-based practices with their clients with dementia should consider collecting data on QOL and cognition changes.
Limitations of Existing Research on Meditation-Based Interventions and Dementia
Much of the research included in this scoping review is limited by weak research design, lack of consistent participant inclusion criteria, high variability in measurement of outcomes, small sample size, and lack of consistency in intervention. Only 11 of the 19 articles included in this review discussed an original empirical study investigating meditation-based interventions for people with dementia. The majority of those studies were conducted within the past 6 yr, with only 1 study conducted before 2012, indicating that this is an emerging area of research. Only 1 of the 11 empirical studies was a randomized controlled trial (Quintana-Hernández et al., 2016), and 2 feasibility studies included randomization and a control group with small sample sizes (Aguirre et al., 2017; Churcher Clarke et al., 2017). Because many of the studies identified in this scoping review lacked a rigorous research design, the findings are likely biased and ungeneralizable. Future research is desirable and should include a rigorous design with a large sample size, randomization, and an equivalent control group.
Researchers assessed many different outcomes and used several different tools to measure those outcomes. In total, 27 different instruments were used by researchers to assess outcomes such as QOL, mental health, cognition, functional abilities, and mindfulness. Not all outcome measures used have been proven to be sensitive to change (Payne, 2017), and many measures have not been validated for use with people with dementia (Churcher Clarke et al., 2017; Moss et al., 2012; Noone, 2017). There was also a lack of consistency in participant characteristics; severity ranged from early stage to late stage, and type of dementia also varied. Some studies included participants with different levels of severity within the intervention group. For example, in the study conducted by Paller et al. (2015), 9 participants had Alzheimer’s disease, 2 had mild cognitive impairment, 2 had memory loss because of multiple strokes, 3 had no clinical diagnosis but complained of memory deficits, and 1 had frontotemporal dementia. Only 8 studies included a comparison group.
In addition to variability in study design, participants, and outcome measures, many different types of meditation-based interventions were used. Of the 11 original empirical studies identified, 1 included an MBCT intervention (Aguirre et al., 2017), 2 included interventions that were based on MBSR (Litherland & Robertson, 2014; Paller et al., 2015), 3 used Kirtan Kriya meditation-based interventions (Innes et al., 2012; Moss et al., 2012; Newberg et al., 2010), 1 included a program that used mindfulness-based techniques (Hanson et al., 2017), 2 included adapted mindfulness-based interventions (Churcher Clarke et al., 2017; Wilson et al., 1997), 1 used mindfulness-based Alzheimer’s stimulation (Quintana-Hernández et al., 2016), and 1 used a meditation tool from Harvard Medical School (Park, 2015). Variation in intervention type indicates that the type of meditation-based intervention that is best for people with dementia is not yet known, and comparative data in this area are needed.
Limitations of This Scoping Review
This scoping review has limitations. Studies that included at least 1 participant with dementia were included in this review, which allowed for the inclusion of multiple studies in which 1 or more participants had mild cognitive impairment or subjective cognitive decline. Results of these studies may not fully reflect the experiences of people with a formal diagnosis of dementia. In addition, only meditation-based practices that were defined by the words mindfulness or meditation were included in this review. The inclusion of articles that were not peer reviewed may also limit the findings of this scoping review because results may be biased. Last, a few articles were excluded because they were not available in English, but they may have included significant findings. Further research could be enhanced by distinguishing between results related to each severity level of dementia and developing search terms that encompass more types of meditation and mindfulness practices.
Implications for Occupational Therapy Practice
Occupational therapy practitioners can best support their clients with dementia by implementing evidence-based interventions that improve QOL and daily functioning. This scoping review suggests that meditation-based interventions may offer promising health and QOL benefits to people with dementia. Given that the promotion of health falls within the scope of occupational therapy practice, practitioners are well-positioned to administer mindfulness interventions for the purpose of maintaining occupational performance in both community-based practice and one-on-one interventions (American Occupational Therapy Association, 2014). With the potential to maintain cognitive abilities and increase QOL, meditation-based interventions for clients with dementia may be a cost-effective strategy for reducing the burden of dementia care.
None of the interventions discussed in this scoping review were carried out by occupational therapy practitioners, but opportunity exists for practitioners to involve themselves in this emerging area of research. Practitioners are uniquely trained to address their clients holistically (Hardison & Roll, 2016), taking into account the interaction of mind and body and its effect on occupational performance. Meditation, which is a mind–body therapy, seems a natural fit for occupational therapy intervention. Rigorous investigation of its effectiveness as an occupational therapy intervention for clients with dementia is warranted and will further develop occupational therapy’s evidence base for dementia treatment.
Occupational therapy practitioners can apply the results of this scoping review to their practice in the following ways:
Implement mindfulness and meditation practices in occupational therapy intervention for clients with dementia and track changes in health and QOL to further investigate meditation as an evidence-based intervention for dementia;
Develop a standardized protocol for adapted meditation programs to ensure consistency in a variety of settings;
Educate caregivers and staff about the potential benefits of meditation, and train staff members to administer meditation-based activities; and
Advocate for more rigorous research in the area of meditation intervention for people with dementia.
Conclusion
This scoping review addressed the effects of meditation-based interventions on clients with dementia, finding that the incorporation of these interventions in clients’ treatment can have beneficial results. The literature highlighted noticeable gaps, including a need for stronger research design, greater consistency in measurement of outcomes, larger sample sizes, more stringent inclusion criteria, and the development of standardized meditation protocols for people with dementia. These gaps in the research made it difficult to generalize conclusions across research studies in the areas of mental health and functional abilities. Further research will help make findings of QOL benefits for this population more generalizable. The most strongly supported outcome identified in this scoping review was the effectiveness of meditation-based interventions in maintaining cognitive function in people living with dementia (Quintana-Hernández et al., 2016). Opportunities exist for occupational therapy practitioners to advocate for and contribute to a growing body of research investigating the use of meditation and mindfulness as an evidence-based intervention for people with dementia.
Footnotes
Acknowledgments
We thank Teresa May-Benson for her support and guidance.
Appendix
Articles on Meditation-Based Interventions for Adults With Dementia Included in Scoping Review
| Author/Year | Study Design and Participants | Intervention | Outcome Measures | Results |
| Aguirre et al. (2017) |
Study protocol for randomized controlled feasibility study N = 32 participants with early-stage dementia and comorbid mild to moderate depression |
8-wk program adapted from MBCT; weekly 1.5-hr sessions, including assignments for daily home practice |
• CSDD • PHQ–9 • QoL–AD • CAMS–R • GAD–7 • RAID |
Results reported by Noone (2017) and Payne (2017) |
| Anderson et al. (2017) |
Integrative review All study samples included people with dementia |
See Innes et al. (2012), Moss et al. (2012), Newberg et al. (2010), and Paller et al. (2015) for interventions. |
See Innes et al. (2012), Moss et al. (2012), Newberg et al. (2010), and Paller et al. (2015) for outcome measures used. |
Analysis of 4 studies: Newberg et al. (2010), Moss et al. (2012), Innes et al. (2012), and Paller et al. (2015) Concluded that MBIs may be beneficial for the mental and physical health of people with dementia |
| Chan et al. (2017) |
Program manual |
Mindfulness program with 10 group-based sessions in care-home settings; 1-hr sessions, 2×/wk, recommended group size of 5; sessions focused on mindful breathing, listening, and movement |
Not applicable |
Not applicable; see Churcher Clarke et al. (2017) for results of the pilot study using this protocol. |
| Churcher Clarke et al. (2017) |
Feasibility pilot study with randomization and control participants Participants with mild to moderate dementia, N = 31 |
Adapted mindfulness program based on protocol listed in Chan et al. (2017) |
• CSDD • RAID • QoL–AD • MMSE • PSS–13 • MBAS |
Significant improvement in quality of life compared with the control group |
| Hanson et al. (2017) |
Pilot study with quasi-experimental pretest–posttest design Clients with a diagnosis of Alzheimer’s disease, N = 38 |
10-wk mindfulness program with weekly 2-hr sessions (comparison group attended Memory Club) |
Not specified |
Significant improvement in emotional health and depression from pre- to posttest In comparison with the Memory Club group, participants in the mindfulness program had significantly reduced anxiety, depression, and stress; they also had improved emotional health and increased serenity. |
| Innes et al. (2012) |
Pilot study with one-group pretest–posttest design N = 10 (5 community-dwelling people with MCI or early-stage Alzheimer’s disease and their caregivers) |
8-wk Kirtan Kriya meditation program; participants instructed to meditate 11 min daily |
• PSS • POMS • PANAS • DRS • GSDS • SCS • MFQ |
Statistically significant improvement in perceived stress, sleep quality, retrospective memory function, and systolic blood pressure (patients and caregivers pooled for analysis) |
| Lima et al. (2016) |
Cross-sectional quantitative study Clients with mild Alzheimer’s disease, N = 128 |
Not applicable; participants’ level of mindfulness was measured using CAMS–R and correlated with medication adherence |
• MARS • CAMS–R |
Medication adherence positively correlated with mindfulness. |
| Litherland & Robertson (2014) |
Pilot study with qualitative analysis Clients with dementia, N = 12 |
MBSR; 8-wk program with 2.5-hr sessions |
• WEMWBS • Semistructured interviews at middle, end, and 3 mo postintervention |
Participants reported reduction in anxiety, help with pain control, help with coping, help with emotional regulation, improved sense of self, improved cognitive functioning, restoration of functional abilities, improved awareness and appreciation, and improved interpersonal relationships. |
| Marciniak et al. (2014) |
Literature review See Innes et al. (2012), Moss et al. (2012), and Newberg et al. (2010) for participant information |
See Innes et al. (2012), Moss et al. (2012), and Newberg et al. (2010) for interventions. |
See Innes et al. (2012), Moss et al. (2012), and Newberg et al. (2010) for outcome measures. |
Analysis of 3 studies: Newberg et al. (2010), Moss et al. (2012), and Innes et al. (2012) Concluded that meditation may be an appropriate intervention for people with cognitive decline |
| McBee (2003) |
Program review Members with moderate to severe dementia in each MBSR group at a nursing home, N = 5–10 |
Modified MBSR program; 1-hr sessions |
Semistructured interviews, included 2 questions from the Coop Inventory on pain and general life satisfaction |
Participants reported feeling less sad. There was a trend toward less pain and feeling reconnected to spiritual heritage. |
| Moss et al. (2012) |
Quasi-experimental pretest–posttest with 2 groups Clients receiving meditation intervention, N = 15 (patients with Alzheimer’s disease, n = 3; patients with MCI, n = 5; patients with age-associated memory impairment, n = 7) Music listening comparison group, N = 5 |
8-wk Kirtan Kriya meditation program; participants instructed to meditate 12 min per day, every day, using a CD at home |
• SPECT scan • STAI • POMS • INSPIRIT • PILS • M-scale • Quest Scale • Category Fluency Task • WAIS • DSST • LM test • TMT, Parts A and B |
Improvement trends in mood, anxiety, tension, and fatigue that correlated with changes in cerebral blood flow Significant improvements in the tension and fatigue categories of the POMS Significant change on the STAI |
| Newberg et al. (2010) |
Pilot study, pretest–posttest with control participants N = 15 (same participants as Moss et al., 2012) |
8-wk Kirtan Kriya meditation program |
• CFT • WAIS • DSST • LM test • TMT, Parts A and B • SPECT scan |
Significant improvement in category fluency in naming of animals compared with the control participants |
| Noone (2017) |
Feasibility study with randomization and control participants (doctoral thesis) Participants with mild dementia who met criteria for depression based on the PHQ–9, N = 20 |
8-wk MBCT program, 1×/wk for 90 min |
• CSDD • RAID • GAD–7 |
No significant reductions in depression and anxiety compared with the control participants |
| Paller et al. (2015) |
Quasi-experimental pretest–posttest N = 17 (clients with Alzheimer’s disease, n = 9; clients with MCI, n = 2; clients with frontotemporal dementia, n = 1; clients with memory loss because of multiple strokes, n = 2; clients with complaints of memory loss with no clinical diagnosis, n = 3); caregivers participated |
8-wk mindfulness program based on MBSR, behavior therapy, and acceptance and commitment therapy; 1 session/wk for 90 min |
• QoL–AD • GDS • PSQI • BAI • TMT, Parts A and B • RBANS • RMPBC • SF–36 • ADLQ |
Nonsignificant improvements in quality of life and depression |
| Park (2015) |
Comparative study Clients with dementia, N = 60 |
Meditation tool from Harvard Medical School |
• BioMed • KDSQ • AMNESIA • VaD |
Statistically significant improvement in dementia-related attributes in the meditation–herbal medicine group at 1 and 2 mo of intervention |
| Payne (2017) |
Pilot RCT (doctoral thesis) Participants with mild dementia who met criteria for depression based on the PHQ–9, N = 20 |
8-wk adapted MBCT intervention with weekly 90-min sessions; included formal home practice (using audio recordings) and informal home practice |
• QoL–AD • MMSE |
No significant improvements in quality of life or cognition |
| Quintana-Hernández et al. (2016) |
Longitudinal RCT with 3 experimental groups and 1 control group Clients with a diagnosis of Alzheimer’s disease, N = 502 |
Three 90-min weekly sessions of stimulation based on MBSR, Kirtan Kriya meditation, sensory stimulation, and chair yoga for 2 yr |
• CAMDEX–R cognitive assessment • CAMCOG • MMSE |
Significant positive changes in cognition for the mindfulness group compared with the control participants and muscle relaxation group; scores equivalent to the cognitive stimulation therapy group |
| Robertson (2015) |
Literature review |
Not applicable |
Not applicable |
Discussion of Innes et al. (2012), McBee (2003), Newberg et al. (2010), Moss et al. (2012), Marciniak et al. (2014), Quintana-Hernández et al. (2016), Paller et al. (2015), and Litherland et al. (2014) Concluded that meditation may help maintain mental capacities of people with dementia |
| Wilson et al. (1997) |
Experimental pretest–posttest design; program review Clients with dementia, N = 14 (mean MMSE score of 8 for intervention group, n = 8) |
Groups of 8–10 nursing home residents met weekly for 1 hr over 12 wk; program focused on modified meditation, relaxation, and guided imagery |
CMAI |
Statistically significant reduction in agitation in the intervention group compared with control participants |
Note. ADLQ = Activities of Daily Living Questionnaire; BAI = Beck Anxiety Inventory; CAMCOG = Cambridge Cognition Examination; CAMDEX–R = Cambridge Mental Disorders of the Elderly Examination–Revised; CAMS–R = Cognitive and Affective Mindfulness Scale–Revised; CFT = Category Fluency Test; CMAI = Cohen–Mansfield Agitation Inventory; CSDD = Cornell Scale for Depression in Dementia; DRS = Dispositional Resilience Scale; DSST = Digit Symbol Substitution Test; GAD–7 = Generalized Anxiety Disorder 7-item scale; GDS = Geriatric Depression Scale; GSDS = General Sleep Disturbance Scale; INSPIRIT = Index of Core Spiritual Experiences; LM test = Logic Memory test; MARS = Medication Adherence Report Scale; MBAS = Meditation Breath Attention Scores; MBCT = mindfulness-based cognitive therapy; MBIs = mindfulness-based interventions; MBSR = mindfulness-based stress reduction; MCI = mild cognitive impairment; MFQ = Memory Functioning Questionnaire; MMSE = Mini-Mental State Examination; M-scale = Mysticism Scale; PANAS = Positive and Negative Affect Scale; PHQ–9 = 9-item Patient Health Questionnaire; PILS = Purpose-in-Life Scale; POMS = Profile of Mood States; PSQI = Pittsburgh Sleep Quality Inventory; PSS = Perceived Stress Scale; PSS–13 = 13-item Perceived Stress Scale; QoL–AD = Quality of Life–Alzheimer’s Disease; RAID = Rating Anxiety in Dementia scale; RBANS = Repeatable Battery for the Assessment of Neuropsychological Status; RCT = randomized controlled trial; RMPBC = Revised Memory Problem and Behavior Checklist; SCS = Self-Compassion Scale; SF–36 = 36-item Short Form Health Survey; SPECT = single-photon emission computerized tomography; STAI = State-Trait Anxiety Inventory; TMT = Trail Making Test; WAIS = Wechsler Adult Intelligence Scale; WEMWBS = Warwick–Edinburgh Mental Well-Being Scale.
*
Indicates studies included in the scoping review.