
Abstract
As the U.S. population becomes increasingly multicultural, occupational therapy practitioners must be adept at working with diverse populations. For the past 15–20 yr, many occupational therapy scholars have recognized this need, and in response, they have promoted cultural competence training. Although cultural competence has provided an important initial conceptual framework for the field, I argue that it is time to move toward a practice of cultural humility, which is defined by flexibility; awareness of bias; a lifelong, learning-oriented approach to working with diversity; and a recognition of the role of power in health care interactions. In this article, I present three main arguments why cultural humility is a more useful and critical conceptual framework than cultural competence, and I review preliminary research that examines the influence of cultural humility on patient experience. I conclude by briefly describing how cultural humility can be incorporated in occupational therapy curricula and applied in clinical and community practice settings.
Past research in occupational therapy has primarily focused on cultural competence as a conceptual roadmap for working in diverse contexts (Beagan, 2015; Muñoz, 2007; Murden et al., 2008; Odawara, 2005; Suarez-Balcazar et al., 2009). A scoping review of cultural competence in occupational therapy found that it is defined by having “knowledge that is specific to each culture,” self-reflection on one’s own culture, and the ability to “create a balance between adherence to cultural norms and introduction of new frames of reference” (Awaad, 2003, p. 357). Cultural competence research initiated a much needed effort in occupational therapy to become more sensitive to cultural aspects of health and wellness. However, I argue that the occupational therapy profession should shift from an emphasis on cultural competence, which implies that culture is a finite construct to be understood and mastered, to a practice of cultural humility.
Cultural humility is defined by a lifelong, learning-oriented approach to working with people with diverse cultural backgrounds and a recognition of power dynamics in health care (Tervalon & Murray-Garcia, 1998). Since the term was coined by Tervalon and Murray-Garcia (1998), it has maintained core components of openness, self-awareness, egolessness, supportive interaction, self-reflection, and critique (Foronda et al., 2016). It differs from cultural competence in several important ways. These differences are outlined in Figure 1. They include an emphasis on learning rather than knowing, recognition of patient and client cultural perspectives as equally valid, and critical reflection on how systemic issues and power differences affect health care.
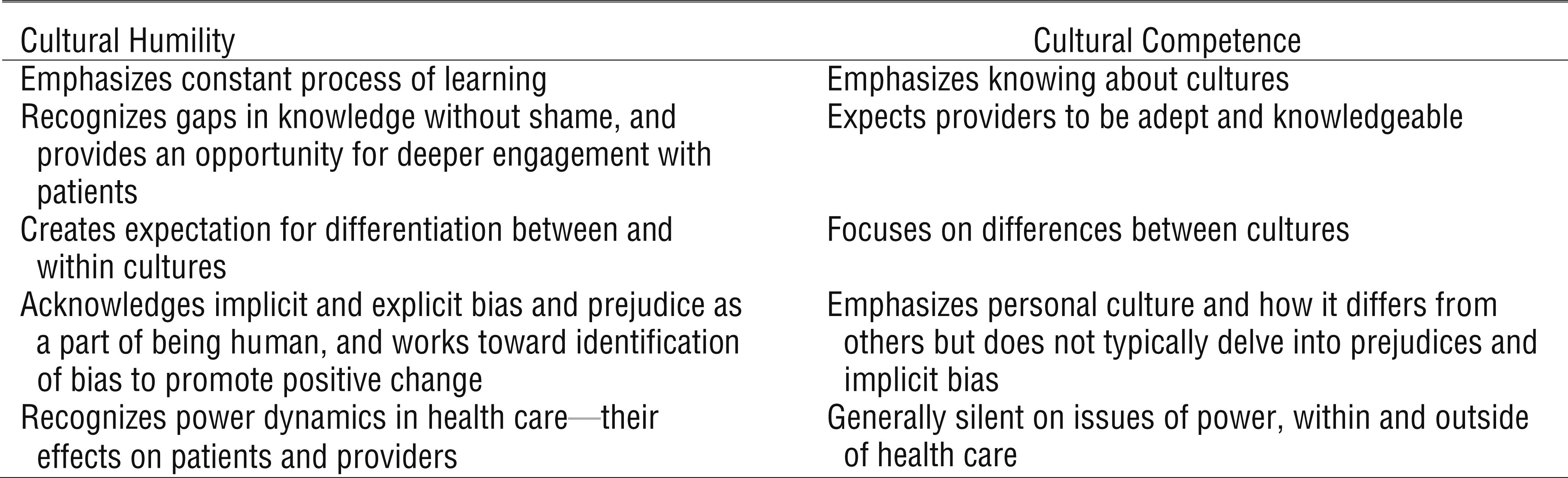
Theoretical differences between cultural humility and cultural competence.
Despite its potential to enhance occupational therapy among diverse populations, a literature review on approaches to culture and diversity within occupational therapy (Beagan, 2015) revealed that only two articles had explicitly addressed cultural humility in relation to occupational therapy practice (Beagan & Chacala, 2012; Hammell, 2013). I build on this work by describing why cultural humility is a more useful and critical concept than cultural competence, and I conclude by describing some steps that practitioners can take to incorporate cultural humility into occupational therapy curricula. This article does not provide an exhaustive review of cultural humility and competence; rather, it furthers the dialogue on how the terms differ and what is of greatest use to the field of occupational therapy.
The Problem of Plurality: Cultures Are Complex, Contradictory, and Evolving
Although culture is often erroneously equated with race and ethnicity, it is in fact a much broader concept that encompasses “any dimension of diversity, including class, gender, sexual orientation, and ability” (Hammell, 2013, p. 224). To complicate matters further, we are all members of multiple cultural groups, with intersecting, multilayered identities. Intersectional cultural identities affect perspectives on occupation, health, and wellness. By recognizing the true complexity of culture, it becomes clear how perceived cultural competence has the potential to lead to stereotyping or cultural assumptions (Edwards, 2016; Kleinman & Benson, 2006; Tervalon & Murray-Garcia, 1998). When people think that they “know” a culture or “understand” it, it is easy for them to fall into essentialist notions about what people of that culture do (Fisher-Borne et al., 2015). “Knowing” can lead to misunderstanding.
I have observed this stereotyping while working as an occupational therapist in skilled nursing rehabilitation facilities. Providers who attempt to recognize the role of culture in their description of a patient or a patient’s situation often do so in a way that treats culture as singular. This behavior is exemplified in comments such as “She is strict because she is Japanese” or “His family is going to take care of them because they are Filipino.” Although these cultural assumptions are not necessarily false, they treat patients as a cohesive unit in relation to their ethnic identity rather than as individuals (Kleinman & Benson, 2006).
This conduct exemplifies how perceived cultural competence can limit recognition of within-group diversity (Edwards, 2016). Cultures are not monolithic, although they are most easily understood that way. In addition to within-group diversity and intersectionality, culture is complicated by contradictory cultural scripts and cultural evolution over time. Cultural evolution has been well substantiated within cultural psychology. Maynard et al. (2015) found that over the course of 43 yr in a Mayan community in Chiapas, Mexico, children’s cognitive abilities changed along with their occupations and their environment. This evidence that cultural roles, and related cognitive abilities, collectively morph over generations suggests that cultural humility is a useful lens even when occupational therapy practitioners are familiar with a particular culture, because it emphasizes having the perspective of a life-long learner with no fixed endpoint. Cultural humility is a process-oriented, ongoing approach to interacting with evolving, culturally defined beliefs, ideas, and behaviors. These examples indicate why, in therapeutic practice, the idea of competence can fall short.
Cultural humility, in contrast to cultural competence, allows and welcomes inconsistencies (Fisher-Borne et al., 2015), indicating an openness to diversity within and across cultures (Hook et al., 2013). Within this framework, occupational therapy practitioners are not expected to know all the details of a particular culture or anticipate how cultural scripts will affect a client’s viewpoint. Rather, the practitioner is encouraged to approach client interactions with a dialogical approach that notices, recognizes, and responds to different viewpoints on health, wellness, family, and role expectations as they play out in individual lives. Practitioners can begin by engaging clients with open-ended questions about their goals and expectations while also considering questions that illustrate how systemic pressures and issues affect the client. Beagan (2015) has provided a list of critically reflexive questioning for practitioners that includes items such as, “How does available public transport affect my client?” and “What assumptions do I make that may not fit for working-class or impoverished clients?” (p. 277). These questions fit within the framework of cultural humility by encouraging a consistent examination of structural issues and of the provider’s own assumptions.
We Are Affected by Our Own Culture . . . and Our Biases
Both cultural humility and cultural competence emphasize that people are affected by their own culture (Danso, 2018; Ekelman et al., 2003), but cultural competence does not require deep introspection on implicit and explicit biases. Ample research suggests that health care provider discrimination on the basis of race (Paradies et al., 2014), weight (Phelan et al., 2015), mental illness (Thornicroft et al., 2007), and several other factors affect how providers treat their clients. This behavior can have significant consequences for health outcomes and engagement in care, and it suggests that encouraging providers to actively examine their biases can have important implications for quality of care and reduction of health disparities. It encourages practitioners to do the work of dismantling deeply held assumptions that may be affecting their relationships with clients, whether they realize it or not.
I now share an example of how my own biases, which stem from cultures and subcultures that I identify with, affected my own practice as an occupational therapist. While working as a home health therapist in New York City, one of my clients, whom I will call Ruby, had severe multiple sclerosis that had progressed to the point that she was unable to leave her bed. She had some controlled movement of her head and neck as well as minimal controlled movement in her hands. Ruby was very sharp intellectually, and she frequently participated in teleconference-type classes on her portable phone. She was interested in and knowledgeable about art and history, but she had stopped going to museums because of her mobility limitations.
When I asked Ruby what she wanted to do that she was not currently able to do, she described that she wanted to use her hands better and that past therapists had done pegboard activities with her (grasping and removing pegs from a soft foam palette). Having studied occupational therapy in a program that discouraged rote activity and encouraged occupation-based treatments, my own inclination was to encourage a goal that related to participation in home or community. I asked Ruby whether she was interested in leaving the apartment. She had a power wheelchair, a caregiver, and a Hoyer lift that would help her get from the bed to the wheelchair. It was entirely possible for her to leave her room and do something in the community that she had enjoyed when she had greater mobility, such as going to the Metropolitan Museum of Art or to a nearby restaurant. However, she was not interested. It took almost a month of visits for her to finally say to me, “I don’t want to leave. I am happy here.”
It was then that I realized that it was actually my fears and biases that were motivating my suggestions for her goals. When she described watching the tree change out the window and participating in teleconference discussions, these were the deep details of her life, her valued occupations. Although Ruby did not have a background different from mine ethnically, she did have a vastly different cultural experience as a homebound woman with multiple sclerosis. The subcultures I adhere to as a traveler, therapist, dancer, and academic center on constant movement and change. My values are also reflective of the capitalist system I was raised in—one that values doing over being, and meritorious actions over inherent worth. Because of my own worldview, which is based on my identity and culture, I felt that she needed to be rescued, and it took several months for me to believe her when she said that she did not. That was the result of my own limited vision, bias, and fear.
With this anecdote, my intention is to illustrate that cultural humility requires deep and continuous self-reflection as well as recognition of how one’s own biases are aligned with dominant cultural narratives. Up to that point, I had participated in many activities designed to promote cultural competence that encouraged me to explore my own culture, but nothing prepared me for this encounter. Cultural humility requires ongoing introspection that can lead to identification of one’s assumptions, biases, and reactions in relationship to others (Charles et al., 2017). Sometimes, those reactions will bring up negative emotions or internal conflicts or dilemmas. Such reactions should not be shied away from as a signal of “cultural incompetence” but rather addressed and embraced as an issue to grapple with. Researchers and academics in occupational therapy can institutionalize this honest approach among practitioners by sharing their own reactions in practice, pedagogy, and writing. Recognizing such reactions humanizes our work, opens up opportunities for dialogue, and allows us to conscientiously develop our approach to diversity within our field.
This example illustrates one of cultural humility’s core differences from cultural competence, which asserts that the more comfortable providers are, the more competent they are (Beagan, 2015). Providers should not necessarily find the decisions of their clients reasonable or immediately understandable. It is expected that uncomfortable feelings and biases will arise as providers work cross-culturally. However, this discomfort is important because intervention research on changing implicit bias indicates that developing awareness of bias is a first and crucial step (Devine et al., 2012). Courageous self-reflection in occupational therapy requires developing institutional and professional cultures that make space for honest reaction and examination of the challenges of working in emotionally difficult, multicultural situations. However, as Beagan and Chacala (2012) have pointed out, cultural humility does not require practitioners to accept or agree with all the decisions that clients make or to adhere unconditionally to their perspectives. Rather, cultural humility involves a recognition that both patient and client perspectives are culturally rooted and that both patient and client are operating within institutions and systems with subcultures that shape their views and their opportunities, which may or may not promote their health.
Power Dynamics Matter
The third crucial difference between cultural competence and cultural humility is that cultural humility explicitly recognizes the role of power in health care interactions (Beagan & Chacala, 2012; Fisher-Borne et al., 2015; Hammell, 2013; Tervalon & Murray-Garcia, 1998). Unfortunately, interactions with health care providers can unintentionally increase a sense of powerlessness, and powerlessness can negatively affect health (Seeman & Lewis, 1995). In a review of health and social science research on powerlessness and health, Wallerstein (1992) determined that powerlessness was a “broad-based risk factor for disease” (p. 197). Although a full review on power in health care encounters is beyond the scope of this article, powerlessness is reinforced when groups in power (in this case, usually health care providers) take actions to maintain control.
Two methods of maintaining social control are direct coercion and ideologic hegemony (Gramsci & Buttigieg, 1992). Direct coercion may occur in health care settings through actual control over clients’ bodies or health care interactions (via restricted movement to prevent falls, forced medication, etc.), whereas ideologic hegemony is more nuanced and subtle. It may involve pressuring clients to change their behaviors or make specific choices based on what the provider deems is necessary or good. Inevitably, these perspectives are culturally informed, and they are not necessarily negative. Part of an occupational therapy practitioner’s job is to promote client safety and encourage health-promoting activities. It is important to be aware of how power is affecting interactions with clients. Moreover, all health care providers, including practitioners, take part in institutions where they are also affected by the power dynamics. These dynamics include pressures from management, reimbursement structures, and workplace norms (Faulkner & Laschinger, 2008; Fisher-Borne et al., 2015).
Cultural humility encourages occupational therapy practitioners to see and learn about these power dynamics, consider how they influence engagement with clients, and attempt to promote a more collaborative, client-oriented, empowering approach. This practice reflects the basic premise of humility, as described by Templeton (1997): “Humility is knowing you are smart, but not all-knowing. It is accepting that you have personal power but . . . inherent in humility resides an open and receptive mind . . . it leaves us more receptive to learn from others” (pp. 162–163). Cultural humility does not prescribe specific changes but encourages practitioners to see how power dynamics affect their work and the lives of their clients.
Initial Implications and Ideas for Pedagogy
Research on cultural humility in clinical settings shows that it can increase and improve the therapeutic alliance (Hook et al., 2013), and similar ideological shifts from cultural competence to humility have begun in social work, nursing, and physician training (Chang et al., 2012). For those convinced that this paradigm shift is useful, the following logical question should be answered next: How should occupational therapy practitioners be trained to be culturally humble? Researchers and professors in public health, social work, and medicine have found that cultural humility cannot be taught using standard didactic methods. Just as culture is not a finite body of knowledge to be memorized and recited, neither is cultural humility. It is a practice skill, and it is entirely possible for students to recite the main aspects of cultural humility without changing their interactions with clients.
In fact, research on cultural humility pedagogy shows that medical students are poor at assessing their cultural skills via survey method. In a group of medical doctor residents, students rated themselves high on cultural adeptness and humility both pre- and postintervention (indicating they had nothing to learn); however, on the basis of clinical observations, their behavior did change (Juarez et al., 2006). After participating in a cultural humility curriculum that incorporated several experiential aspects, reflective exercises, and didactic training on racism and bias in health care, the medical students became more client oriented during clinic visits, asked more open-ended questions of their clients, and asked more questions that related to culturally rooted beliefs (Juarez et al., 2006).
Schuessler et al. (2012) also found that a journaling-based cultural humility curriculum was effective at increasing students’ awareness and changing their perspective from one of “knowing” to one of “learning.” The journaling exercises were paired with discussions and didactic material and occurred in relation to fieldwork experiences that students were having in clinics and hospitals. These two approaches give some insight into how cultural humility might be taught (combining experiential, reflective, and didactic approaches), although there is a need for the development of cultural humility pedagogy specific to occupational therapy.
Conclusion
Although the concept of cultural competence provided a useful starting place, it is time to develop a more radical and nuanced position to working in a multicultural society. Both cultural competence and cultural humility are focused on increasing awareness of one’s skills and behaviors while working in multicultural situations. However, important differences exist. Cultural humility provides a more critical and effective approach to working with clients with diverse perspectives. This shift in practice has the potential to increase the effectiveness of health professionals, reduce health disparities that fall along cultural lines, and increase the relevance of occupational therapy as it develops globally.
Footnotes
Acknowledgments
I thank Karen Whalley Hammell for providing comments and for sharing her expertise in this area.