
Abstract
The 1999 U.S. Supreme Court decision Olmstead v. L. C. (527 U.S. 581; Olmstead) ruled that unjustified segregation of people with disabilities is unlawful under the Americans With Disabilities Act of 1990 (ADA; Pub. L. 101-336). The court held that people with disabilities have a right to reasonable accommodations to enable them to live in the least restrictive community setting. The decision was a landmark for disability rights because it revealed the potential of the ADA to legislate the full inclusion of people with disabilities into their communities, with equal access to social participation and opportunities (Dinerstein, 2016).
The realization of the full potential of the ADA is limited by several factors, including variation in state compliance and enforcement and unequal application of community-based services and supports that enable people with disabilities to live in community settings (Eiken, 2016). Disability rights efforts have focused on Olmstead implementation through referrals, systems-level advocacy, and helping people transition from institutions into community settings. This work has been carried out by disability community organizations, including Centers for Independent Living (CILs), a national network of consumer-led nonprofit organizations. Today, a growing number of people with disabilities are transitioning from institutions—such as Medicaid-certified, long-term care nursing homes (herein, “nursing homes”); intermediate care facilities; and institutes for mental disease (herein, “institutions”)—into community settings (Irvin et al., 2017).
Although studies have been conducted regarding older adults’ transition into the community from these institutions (Allen et al., 2014; Leppin et al., 2014), little is known about the growing demographic of people transitioning who are younger than age 65 yr (Irvin et al., 2017), especially when those transitions are not from acute settings or involve people with disabilities other than strokes, traumatic brain injury, and spinal cord injury (Gustafsson & Bootle, 2013; Hall et al., 2012; Kraus, 2015). To best support this younger and growing demographic, researchers and practitioners need to understand their transition experiences, including the type and amount of supports needed to facilitate transition and long-term community living and participation (National Council on Disability, 2015, 2018).
Research in which first-person accounts are used to understand community participation for community-dwelling people with disabilities (Hammel et al., 2008, 2015) is useful as a starting point because it considers how people with disabilities themselves define full community participation. We are also able to draw from new research that aims to understand the complex and intersecting environmental factors that affect participation (Heinemann et al., 2013; Magasi et al., 2015; Mallinson & Hammel, 2010). Qualitative research has resulted in an emic conceptual framework to describe participation and the environmental factors that influence participation (Hammel et al., 2015). The model identified eight major environmental factors: built, natural, transportation, assistive technology, information and technology access, social support and societal attitudes, systems and policies, and economics. These findings suggest that rehabilitation models focused only on the microlevel (i.e., the immediate physical environment) may be insufficient because community- and societal-level factors are dynamic and have cumulative influences on participation.
Despite these advances in knowledge, there is an urgent need to examine participation during and after people transition into the community from institutions among a broader sector of people with disabilities, including those with multiple disabilities, and within broader communities. More research is needed to identify how they describe full participation, what supports or hinders it, and what their participation looks like over time as they seek community integration.
To address this gap, the Americans With Disabilities Act–Participatory Action Research Consortium (ADA–PARC), a unique collaboration among academic researchers, ADA centers, community stakeholders, and people with disabilities (Hammel et al., 2016), is implementing a multimethod, multiphase, participatory action research (PAR) study to gain an in-depth understanding of participation among people with disabilities who have transitioned into least restrictive community settings under Olmstead. PAR is an approach in which researchers and community members create a dynamic, sustained partnership to carry out research (Whyte, 1991). As part of the ongoing ADA–PARC study, we conducted qualitative interviews to explore the following research questions: How do people with disabilities describe full participation after transitioning from an institution to the community under Olmstead? What are the environmental barriers and facilitators to full participation during and after this transition?
Method
We used a PAR approach to design, conduct, analyze, and interpret semistructured qualitative interviews with 153 people with diverse disabilities who had moved out of an institution into the community under Olmstead. The ADA–PARC is a national-scale PAR study in which community partners include not only people with disabilities but also community organizations that advocate for the rights of people with disabilities. Specifically, ADA–PARC includes these three community partners: (1) ADA centers, which are funded by the National Institute on Disability, Independent Living, and Rehabilitation Research to provide regional information, guidance, and training on how to implement the ADA; (2) CILs, which are consumer-led, community-based, nonprofit agencies that provide independent living services; and (3) a national network of disability organizations, policymakers, service providers, and employers. Community partners were involved at every phase of the project, as described in detail in this section. Human subject consents were coordinated through the University of Illinois at Chicago, with additional institutional review board assessments by regional partner sponsors.
Participants and Setting
ADA–PARC community partners (seven ADA centers representing nine U.S. states and their affiliated networks of CILs, community organizations, and disability advocacy groups) coordinated recruitment and data collection for their catchment area. Community partners used multimodal methods (mailers, posters, events, social media posts, newsletters, email lists) to recruit a criterion-based sample of 153 people who self-identified as a person with a disability, transitioned in the past 5 yr from an institution (including public nursing homes) to the community, and were ages 18–65 yr at the time of transition (Hammel et al., 2016). Participant demographics are listed in Table 1.
Participant Demographics (N = 153)
Note. GED = General Educational Development.
All respondents transitioned to a community living setting before reaching age 65, but respondents could be age 65 or older at time of interview.
Respondents could choose more than one category.
Yearly income includes benefits, insurance payments, and subsidies.
Measure
The ADA–PARC community partners created and member checked a semistructured accessible interview guide (quantitative findings from the ADA–PARC study are reported separately), including open-ended questions addressing issues that the disability community deemed most important:
The impact on one’s life of the ADA and moving from an institution to the community
Personal definitions of full community participation
Desired home and community activities, including those with unmet support needs
Descriptions of everyday life, choices, and control in institutions versus the community
Factors that support or prevent one from fully participating in the community long term, during and after the transition out of an institution.
Procedures
Collaboratively, ADA–PARC academic and community partners trained 34 interviewers from local communities, including many interviewers with disabilities. From 2015 to 2017, interviewers obtained informed consent and conducted in-person interviews lasting 60–90 min each. In a few cases, interviews were conducted by phone when requested by participants for accessibility. Participants received a $25 gift card. Interviewers transcribed participants’ responses during the interviews. Academic researchers oversaw data management and cleaning.
Data Analysis
Four primary analysts used inductive, or “data-driven,” thematic analysis to independently code one-fourth of the data, creating an initial code scheme (Braun & Clarke, 2006). We then used an iterative process of coding additional data and revising codes on the basis of group discussion and comparison. At least two team members coded every interview using a semantic level of analysis focused on the explicit or surface meanings of the data. We then used a theoretical, or “analyst-driven,” thematic approach in which data were coded for specific research questions (Braun & Clarke, 2006), drawing from the emic conceptual framework for full participation described previously (Hammel et al., 2008, 2015). Last, we used a latent level of thematic analysis to identify underlying assumptions and ideologies (Braun & Clarke, 2006). Analysis at the latent level was particularly influential in regrouping and refining the overarching story. The themes were regularly presented to the full ADA–PARC team, including collaborating disability communities, for member checking.
Results
We identified four main themes, described in detail in this section, that depicted full participation in the context of transition (Figure 1). The sizes of the cogs in Figure 1 represent the frequency with which the themes were present in the data. The themes and subthemes were dynamic and interrelated, as shown by Figure 1 and Table 2.
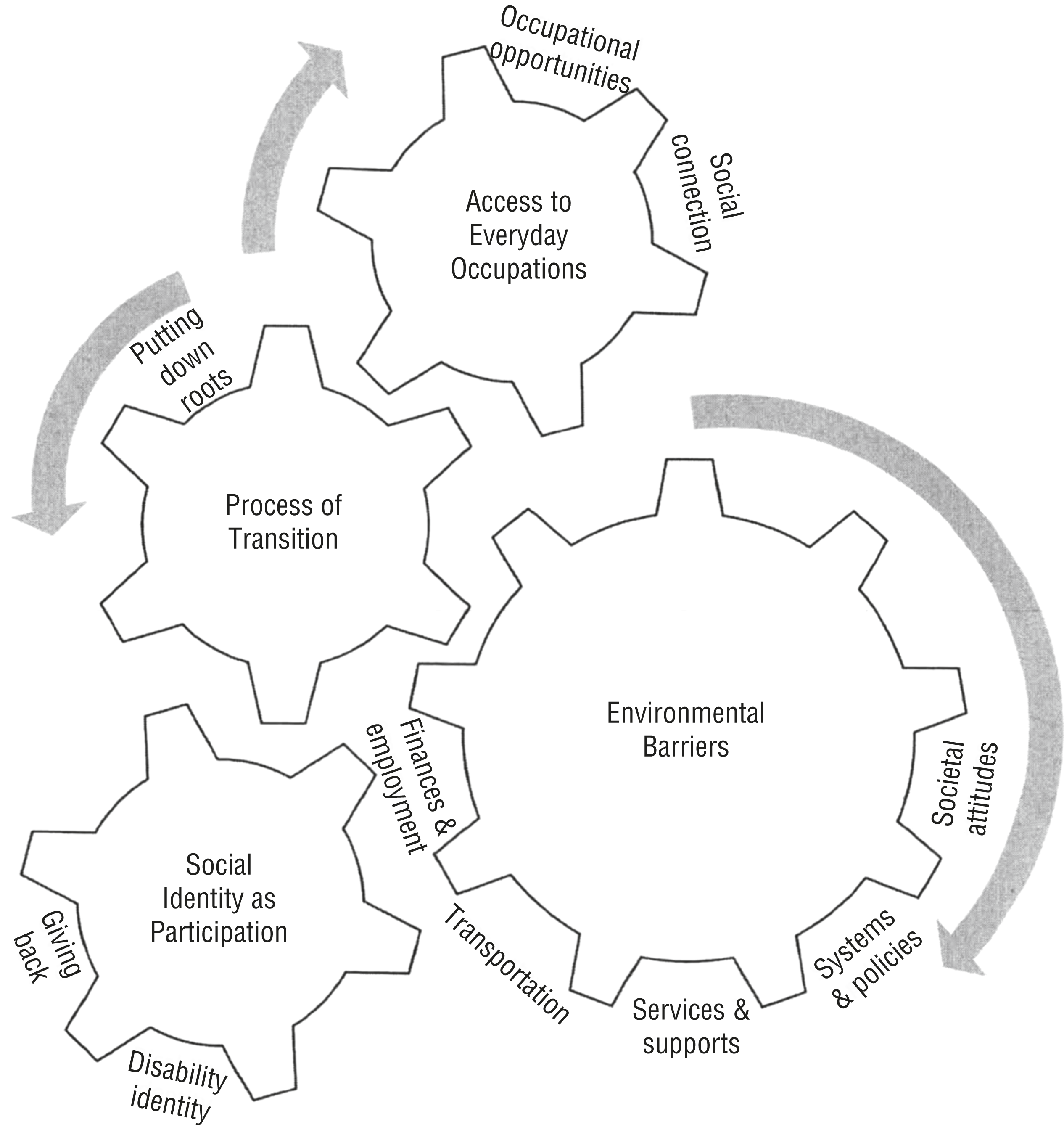
Full participation, as described by people with disabilities after transitioning from an institution to the community.
Commonly Linked Themes and Subthemes Showing Participation Barriers and Needs
Process of Transition: “It Takes a While to Get Back in the Swing of Things”
Participants spoke about transitioning from an institution to community living both as a one-time event and an ongoing, long-term process. They considered the transition, and full participation, as something they were still working toward. Full participation required time to learn their way around their new neighborhood and find the places where they needed to go: “At first, [it was] hard to know who to go to, what pharmacy to go to . . . It smoothed out.”
Putting Down Roots
We refer to this “settling in” as putting down roots. In addition to the time required to learn the new neighborhood and community, participants also had to adjust to the freedom and independence afforded in the community. This independence was often a stark contrast to being told while institutionalized that they were unable to do things independently. One participant said,
Living in [a] nursing home was so structured, having to do things at a certain time. When you live in your own apartment, you still feel that way. “Wait a minute, I can eat when I want?!” You’re free now. I tell people it takes a while to get back in the swing of things; it’s the total opposite. You have to learn or relearn a lot. It’s the little things that others take for granted. It can be very overwhelming.
As participants navigated this dramatic change, having access to everyday occupations was a grounding experience that facilitated their adjustment.
Access to Everyday Occupations: “Start to Live a Life”
Although the meaning of full participation varied among participants, a common underlying concept was access to specific, individually meaningful occupations. Being free to carry out everyday occupations was fundamental for their improved quality of life. Returning to such occupations was not simple or automatic after the transition but instead required ongoing supports in the form of occupational opportunities and social connection.
Occupational Opportunities
Participants frequently noted that everyday activities, such as shopping or cooking meals, were remarkably meaningful. They had been unable to do these things in the institution and were grateful to have the freedom to do them now in the community. Participants named a range of occupations they were doing, or wanted to do, that constituted full participation, including eating at restaurants; going to museums or the library; swimming; fishing; going to a gym; going to church; watching an event on TV at a bar; and participating in community events such as festivals, concerts, support groups, or protests. Notably, communities varied in the number and quality of such opportunities.
Another opportunity that participants linked to full participation was education, often a formal university or community college degree they wished to pursue. One participant said, “I would like to work and go to school, so that I could have my own place.” In a few cases a lack of reasonable accommodations prevented participants from completing a degree, contributing to their financial challenges: “Tried to get some certificates and degrees, but the trade schools did not provide support to pass the exams. [I’m] in a lot of debt to these schools.”
Everyday activities were critical for participants to feel they had begun to fully participate in their community. One participant, when asked what they would like to do that they were not currently doing, responded, “Take the dog on a walk. Get around without a walker, go to some stores without it being painful. Start to live a life [emphasis added].”
Social Connection
Everyday occupations were linked to social connection, including romantic relationships. One participant said that full participation was the ability to “go to a party and come back whenever you want, and have a companion stay overnight.” Another said, “It just feels better when you’re being with people and being a part of something.” Another defined participation as “socializing, building the links and the connections in the community.” Another emphasized the power of social connection: “It means I’m active, happy lifestyle, connecting, building trust, bonds, goodwill, and fellowship. Those are good things to have . . . they could save your life [emphasis added].”
Environmental Barriers: “I’m Not Really Participating as I Want to”
Participants described environmental barriers to participation, including finances and employment, transportation, services and supports, systems and policies, and societal attitudes.
Finances and Employment
A major barrier to participation was a lack of financial resources and employment opportunities. Although participants overwhelmingly preferred community living over institutionalization, some lacked enough money to meet their basic needs: “Sometimes I am running low on money and need to wait to buy food.” Others had their basic needs met but did not have the resources to participate in additional community activities: “A lot of stuff I would like to do, I can’t afford to.”
Participants linked their financial challenges to a lack of employment opportunities, and they wanted “to be able to work and socialize like everyone else.” When asked whether they were fully participating, a participant answered, “[I] would be if I was working.” However, they faced a dilemma: If they worked, they would lose their benefits but would still not earn enough to cover their basic expenses. This disincentive prevented them from looking for work and hindered full participation.
Transportation
A lack of transportation was also a major participation barrier. Although participants had more freedom in the community to come and go as desired, they struggled to find affordable and accessible transportation. This limitation prevented them from securing and maintaining jobs, visiting family and friends, and participating in activities: “Very important to have transportation to go out when you want and where you want. [I] had to quit my job because of a lack of transportation.”
Some participants were able to secure support for transportation, but this access did not constitute full participation because they remained dependent on the limited schedules and availability of others. In some cases, paratransit had to be reserved 2 wk in advance or could only be used for medical appointments, which further hindered spontaneous travel and socialization. Although these participants had some access to transportation, not having consistent, high-quality, affordable access limited their full participation. Many participants identified transportation as the sole issue preventing them from participating in their communities as desired: “No, I’m not really [participating as I want to]. I could be, but because of transportation . . . I’m not able to get to other events.”
Services and Supports
Although community living was a dramatic improvement from life in the institution for most, many reported that a lack of services and supports significantly hindered their participation. These supports included personal attendants, adapted and assistive technology, case management, and comprehensive health care. Not having a caregiver or personal attendant had significant consequences:
There are things I want to do but can’t because my help only comes when they want to come, instead of when I need them to come. I’ve missed going to church many times because people wouldn’t come early enough to help me get ready.
Another said, “If no one is around to help me cook then I don’t eat.” Trying to get support often required jumping through bureaucratic hoops:
I wish they hooked me up with a caregiver when they knew I was moving. [I talked to my case manager about a] motor scooter—that fell through. [The] case manager will suggest something but then tries to move it to my lap . . . My hands are tied.
Inadequate health care services were also a problem: “[Living in the community] is less stressful, happier, I get more sleep. But the setback is at least in the nursing home I was getting therapy services, and now I’m not because of transportation issues.” Participants described the high stakes of inadequate health care services: “During the transition . . . there were issues with getting prescriptions from the psychiatrist. This resulted in missing medication and having to be admitted to [an] inpatient psychiatric hospital to stabilize.” A participant who was unable to get a motorized wheelchair described the profound impact that it could have on their life:
I can take the bus places, but I’d have to have somebody with me. I don’t have an electric wheelchair. The community is not accessible without a motorized chair because of the cars, cracks in the sidewalks. I can’t carry anything, get on the bus or train and go places, businesses, shopping. [Having a motorized wheelchair] would change everything. It would prolong my existence for 10 years [emphasis added].
Systems and Policies
Despite describing ways that their lives had been improved through the ADA and Olmstead, participants also reported ADA violations they had observed in their own or others’ lives that affected their full community participation:
I’ve faced a lot of discrimination trying to get jobs. I’ve applied to many jobs but have seen these jobs be given to other people, often because they were able-bodied. I’ve lived in the same room for rent for 8 years. The landlady keeps telling me she will install an accessible shower, but it hasn’t happened.
Physical environments that were not compliant with the ADA prevented many from fully participating in their communities. Some were frustrated with what they felt was slow progress, or even backward movement, in seeing ADA rights monitored and enforced: “There are cutouts in the curb, some businesses are accessible. There have been some good things, there is still a lot to be done. Progress has moved very slowly, especially with all the technology we now have.”
Societal Attitudes
Many participants felt more accepted as part of their communities after the transition. However, many felt only partially accepted, describing the need for greater awareness and acceptance of disability as well as respect for people with disabilities as equal citizens. One participant described how societal attitudes can hinder participation: “Every time I divulge I have a diagnosis, I lose friends, jobs, etc.” Another said, “I wish people were educated about mental illness.” In summary, moving to the community, although a dramatic improvement from being institutionalized, did not automatically enable full participation because of the need for services and supports to address environmental barriers.
Social Identity as Participation: “I Can Make a Difference”
The final theme describes participants’ development of identity and sense of self posttransition. Institutionalization and the resulting loss of autonomy left participants to grapple with their self-concept and social identity. For some, reclaiming their identity, through giving back or connecting to the broader disability rights community, was a key participation facilitator.
Giving Back
Many participants described full participation as the ability to “give back,” creating a strong sense of identity by helping others. One participant said, “I’m able to use my talents. My goal is to make a difference. I’m helping friends, working in politics, taking care of somebody.” Community organizations, such as CILs, also facilitated full participation by enabling participants to give back to other people with disabilities. One participant said, “I want to help people with disabilities. They need help, and I need help.” Another said, “My journey has been hard, but I can help make someone else’s journey a little easier. I don’t want someone to go through what I went through.”
Disability Identity
A key tenet of disability rights is rejection of a biomedical view of disability, which locates the “problem” within the person (Charlton, 1998), instead viewing the environment as “disabling” and the disability community as an asset and strength. Some participants in our study proudly claimed a disability identity and viewed the problem as the environment. Their identity shift after transition to the community was associated with being integrated into advocacy communities, such as CILs.
Conversely, our analysis identified participants whose identity seemed strongly influenced by dominant societal views of disability, that is, viewing disability (rather than the environment) as the problem preventing participation. This notion is linked in disability studies literature with stigma and internalized oppression (Abberley, 1987). Some examples of participant comments are, “[I am] not able to participate in the community because my disability prevents [me]” and “There are things I want to do like skateboarding, bicycling, etc., but can’t because I don’t have legs.” Although this notion could be considered an attitudinal barrier to participation, a strong link was found between a positive disability identity and the support of the disability community, suggesting disability identity develops within the social context of the disability community.
Discussion
These qualitative findings, part of a larger PAR project, provide an in-depth understanding of the participation experiences of people with diverse disabilities across the United States transitioning from an institution to community living. Our findings fill a gap by including a national sample of people with a range of disabilities, including multiple and psychiatric disabilities, and examining participation after transition. The study design, part of a larger ongoing national PAR study, also fulfills a need for more research that is grounded in the perspectives and experiences of people with disabilities at every step of the process. With increasing numbers of people with disabilities transitioning after Olmstead, these findings highlight the urgent need for policymakers and service providers to consider transition as a process that requires ongoing and long-term supports and services.
Our findings confirm previous research indicating that post-ADA, there continues to be a need for financial support and appropriate, well-paying, accessible work opportunities; accessible, affordable, and readily available transportation; services, supports, and policies that are relevant and responsive to diverse and changing needs; and societal education, awareness, and respect for people with disabilities as equal citizens (Hammel et al., 2008, 2015; McDonald et al., 2015). Institutionalization has been compared with incarceration as a similar form of confinement that strips people with disabilities of choice, control, and a sense of positive identity (Ben-Moshe et al., 2014). Our findings expand on this literature by showing the deep and long-lasting effects of institutionalization, which include attempting to regain one’s self-confidence and social identity.
Although previous research has identified the importance of a social network for people transitioning to the community from an institution, our findings show how social connections with a disability community were critical for some participants to gain (or regain) a positive disability identity (Cott et al., 2007). Arntzen et al. (2015) also found that community integration after stroke was a long-term process in which people gradually “reposition participation,” that is, make incremental adjustments in specific contexts, to undergo a transformed sense of self. However, Arntzen et al. recommended extended professional support to facilitate participation and sense of self. Although our findings also point to the need for extended support, our participants reported a positive disability identity as emergent from the support of the disability community (and peer supports), not facilitated by professionals without disabilities. This finding highlights the key role of disability organizations in connecting people to resources and providing a shared lived experience and empowering identity long term after transitioning from institutionalization to the community. Future research could investigate the effectiveness of interventions that involve partnerships between occupational therapy and disability organizations.
Strengths and Limitations
The ADA–PARC study drew on the strengths and knowledge of disability communities by involving numerous geographically diverse collaborators across six ADA centers and their affiliated networks of community organizations. Although this network enabled us to capture first-person experiences of people with diverse disabilities across the United States, this study has some limitations: Using a large team of interviewers from multiple sites may have decreased fidelity, recording participant answers by hand may have resulted in errors, interviews done at one point in time did not allow us to readily study the direction of effects, and the range of disability types in our sample may have obscured particular disability experiences.
Implications for Occupational Therapy Practice
The results of this study have the following implications for occupational therapy practice:
People with disabilities may strongly prefer living in least restrictive community settings over institutions, and living in the community may better facilitate their community participation.
However, people with disabilities reported that the transition to the community itself was not enough to support their full participation.
The transition from an institution to the community may be an ongoing process requiring time, extended services, and formal and informal social supports, including local disability, independent living, and advocacy organizations.
Occupational therapy practitioners working in institutional and community settings could seek to partner with local disability advocacy communities to support their clients’ development or regaining of a sense of identity and self-confidence during and after transition to the community.
Conclusion
Although people with disabilities younger than age 65 yr are increasingly transitioning to the community under Olmstead, our findings show that the transition is not enough to facilitate their full participation long term. In addition to the need for ongoing services and supports, these findings reveal the critical role of social networks and supports. Disability advocacy organizations support the transition to the community not only by connecting people to resources and information about their rights but also by modeling a positive and empowering disability identity. Our findings indicate that transition should be thought of as a long-term process that is supported with individualized, consumer-driven, flexible transition plans that can be adjusted over time to support full participation.
Footnotes
Acknowledgments
We thank the entire ADA–PARC network of collaborators, especially the following organizations for their assistance and support of this research project: Access Living (IL), Accessible Resources for Independence (MD), Bay Area Center for Independent Living (MD), Liberty Resources (PA), North Carolina Statewide Independent Living Council, North Carolina Independent Living Centers, North Carolina Money Follows the Person, Thresholds (IL), Transitional Paths to Independent Living (PA), and Valley Associates for Independent Living (VA). We also thank Cesar Barreto, Peter Blanck, Roxy Funchess, Jenna Heffron, Robin Jones, Danbi Lee, Maren McDowel, Michael Morris, Vinh Nguyen, Pimjai Sudsawad, Barry Whaley, Sally Weiss, Pam Williamson, and Tom Wilson.
This work was supported by National Institute on Disability, Independent Living, and Rehabilitation Research (NIDILRR) Grants 90DP0026 and 90DPAD0001. The writing of this article was made possible by support from NIDILRR Grant 90AR5023. The contents of this article represent the opinions of the authors and not necessarily those of the NIDILRR, the Administration for Community Living, the Department of Health and Human Services, or the federal government.