
Abstract
After nearly 3 decades of extensive discussion and promotion, principles of mental health recovery have emerged as a mainstream framework for the provision of mental health services. Unlike the traditional medical definition of recovery, which highlights cure and removal of symptoms, mental health recovery stresses the manifestation of individual potential and the fulfillment of personal goals (Bellack, 2006). A well-known definition of recovery is “a deeply personal, unique process of changing one’s attitudes, values, feelings, goals, skills, and/or roles” (Anthony, 1993, p. 15). People with mental illness tend to experience multiple relapses in their lifetime, making recovery a nonlinear process, and they can embark on a recovery journey at any time, regardless of illness stage or symptoms. A key principle of recovery is that it coexists with symptoms; mental illness does not define the person or keep the person from pursuing recovery (Anthony, 1993; Davidson et al., 2005).
The number of recovery programs for people with mental illness has been growing. A recent meta-analysis showed that recovery programs may improve recovery, hope, and empowerment for people with mental illness (Thomas et al., 2018). One program, Pathways to Recovery (PTR), based on the book Pathways to Recovery: A Strengths Recovery Self-Help Workbook (Ridgway et al., 2002), highlights personal strengths and encourages users to set personal recovery goals and plans. Green et al. (2013) examined a PTR program led jointly by peers (people with mental illness) and professionals and found significant improvements in participants’ feelings of hopefulness, social relationships, and symptoms. Another study conducted a peer-led PTR recovery group and found significant improvements in self-esteem, self-efficacy, social support, well-being, and symptoms (Fukui et al., 2010).
Occupational therapy and mental health recovery have many similarities, in that both highlight a holistic approach and client-centered practice. Occupational therapy stresses the health benefits of participating in occupations (American Occupational Therapy Association [AOTA], 2014), and recovery principles stress that participation in meaningful activities is essential for recovery. Recovery goals set by people with mental illness often include such key occupations as employment, health management, and education. Only through participation in meaningful activities can people with mental illness recover and lead a satisfactory life (Davidson et al., 2005; Ridgway, 2001). It is evident that occupational therapists can play a major role in mental health recovery.
Little published research exists on mental health recovery programs in Taiwan (Hsiao et al., 2010; Lin et al., 2013), and many Taiwanese people with mental illness are unfamiliar with the concept of recovery. A recovery group that explains and demonstrates recovery concepts may therefore be beneficial to these people. However, because mental health recovery originated in the Western world, it highlights individualism, self-determination, and personal choices, concepts that are at odds with ethnic Chinese society, which stresses submission to seniority and authority (Davidson & Tse, 2014; Mak et al., 2016). Because most studies of recovery programs have been conducted in Western countries (Thomas et al., 2018), studies exploring the cultural adaptation of recovery programs to non-Western countries are needed. We addressed these research and treatment gaps by developing a recovery group for people with mental illness in Taiwan and investigating its feasibility and acceptability.
Method
Participants
Study eligibility criteria were as follows: having a diagnosis of mental illness, being age 20 yr or older, living in the community, receiving services from the collaborating agency, and being able to participate in a recovery group and follow the group rules. People who could not fill out the scales independently were excluded.
Intervention
We designed a recovery group tailored to Taiwanese people with mental illness that was based on the PTR program (Ridgway et al., 2002) and mental health recovery literature (Davidson et al., 2005; Ridgway, 2001). The group gathered for a 1-hr session once a week for 18 wk. The curriculum included two phases. In the first phase (recovery profile), the main objective was to introduce the concept of recovery, including hope, empowerment, taking responsibility, self-redefinition, meaningful activities, and personal strengths. In the second phase (recovery plan), the main objective was to encourage participants to begin their recovery journey, including discussing published recovery stories, setting and executing recovery plans, and writing their own recovery stories. During the development process, participants were invited to offer suggestions about the group’s implementation in the last session of each phase.
On the basis of participants’ feedback, we added recovery stories and role exploration to our curriculum. Given participants’ unfamiliarity with the concept of recovery, the group spent the first phase learning about the concept itself. Many participants, however, still expressed frustration with understanding the concept, saying it was abstract, and demanding more examples to facilitate their understanding. Therefore, in the second phase, one indigenous recovery story was provided every week for participants to read at home and discuss with peers at the start of the next session.
Along with being introduced to the concept of recovery, many participants learned of concept of self-redefinition for the first time and realized its importance. Self-redefinition stresses that mental illness is only part, not all, of a person. People with mental illness should not focus on the patient role while neglecting other important roles and personal strengths (Jacobson & Greenley, 2001; Ridgway, 2001). To help participants further understand this concept, we added role exploration, which is not included in PTR, to the second-phase curriculum. We used the Role Checklist (Liu et al., 2004; Oakley et al., 1986) to help participants identify their past, present, and desired future roles. Then, to serve as a basis for their formulation of recovery goals, we discussed capabilities and occupations for their desired roles.
Because participants’ language was Mandarin, they could not read the PTR curriculum. Therefore, authors Chang and Su, who were familiar with mental health recovery concepts, translated the main titles or themes of each chapter of the PTR workbook and some forms or scales for course practice or homework and then designed a Chinese-language manual. The group content was taught by a senior occupational therapist (Su). Participants were required to complete weekly homework assignments that were based on session content. Group topics are listed in Appendix A. A supervisor met with the group leader after every session to confirm the accuracy of the information delivered.
Instruments
Stages of Recovery Scale
The Stages of Recovery Scale (SRS; Song & Hsu, 2011) was developed by Taiwanese scholars and is based on mental health recovery literature and three recovery scales. The SRS has 45 items and six subscales: Sense of Hope, Disability Management/Taking Responsibility, Regaining Autonomy, Social Functioning/Role Performance, Overall Well-Being, and Willingness to Help. It has good internal consistency (α = .80–.95 for subscales) and appropriate construct validity. SRS items are rated on a 4-point scale: never (0), seldom (1), sometimes (2), and often (3). Higher scores indicate better recovery. Song and Hsu (2011) also provided cutoff scores for four recovery stages: Stage 1 (overwhelmed by the disability), 0–57; Stage 2 (struggling with disability), 58–90; Stage 3 (living with disability), 91–119; and Stage 4 (living beyond disability), 120–135.
Course Assessment
The researchers (Chang and Su) designed the course assessment, including the course questionnaire (Cronbach’s α = .94) and course feedback. For the first- and second-phase course questionnaires, the first seven items were the same; other items were formulated according to the content of the two-phase curricula. A 5-point rating scale was used (1 = strongly disagree to 5 = strongly agree). Participants were also invited to express their opinions on the curriculum through responses to open-ended questions, as a reference for subsequent program improvement.
Data Collection
The study was approved by the institutional review board of National Cheng Kung University Hospital (No. A-ER-106–245). The recovery group was conducted at a community psychiatric rehabilitation center in southern Taiwan. The staff of the collaborating agency assisted in recruitment; participants attended the group after informed consent was obtained. The recovery group had two cohorts; the first cohort consisted of 10 participants, and the second cohort consisted of 14 participants. Participants filled out the SRS in the first class. At the end of each phase of the curriculum, participants filled out the SRS and course assessment and then participated in a 30-min discussion. The discussion included two parts: recovery stage change experiences and course suggestions. Discussions were recorded and transcribed.
Data Analysis
We collected both quantitative and qualitative data. IBM SPSS Statistics (Version 20; IBM Corp., Armonk, NY) was used for descriptive statistical analysis. We also calculated the effect size estimate, r, by dividing the z score by the square root of the number of total observations. We considered r = .10 a small effect; r = .30, a medium effect; and r = .50, a large effect (Cohen, 1988). The feasibility of the recovery group was evaluated by means of course questionnaires and qualitative data, including course feedback and course discussion transcripts. The corresponding author (Su) coded the qualitative data. The first author (Chang) reviewed the coding and discussed any disagreements with the corresponding author until consensus was reached.
Results
Participants
Of the 24 study participants, 75% were women; 54% had been diagnosed with schizophrenia, and 42% had been diagnosed with bipolar disorder; 71% were single; 75% had a college or higher education; and 83% engaged in supported employment. The majority were at Recovery Stage 3 (42%) or Recovery Stage 4 (29%), according to the pretest SRS. Participants’ mean age was 43.21 yr (standard deviation [SD] = 8.37; range = 27–59), and the average attendance rate was 93% (SD = 0.10; range = 63%–100%; Table 1). Three participants were excluded from analysis as a result of incomplete posttest data.
Participant Demographic Characteristics (N = 24)
Note. M = mean; SD = standard deviation; Stage 1 = overwhelmed by the disability; Stage 2 = struggling with disability; Stage 3 = living with disability; Stage 4 = living beyond disability.
Stages of Recovery Scale
We found that participants who were at Stage 4 at pretest had performance differences from participants at other stages, so we divided the participants into two subgroups (Stage 1–3 group and Stage 4 group) on the basis of their pretest recovery status scores. The two subgroups had no significant differences in gender, age, or diagnosis. They tended to perform differently on the SRS (Figure 1); the Stage 1–3 group scored higher at the end of the first-phase curriculum but had almost no change at posttest compared with the Stage 4 group, which tended to score slightly lower, with posttest scores still within the range of Stage 4 (>120). In addition, we found medium to large effect sizes (i.e., .30 ≤ r < .50) for Social Functioning/Role Performance scores for all participants and for SRS total scores, Disability Management scores, and Social Functioning/Role Performance scores for the Stage 1–3 group (Table 2).
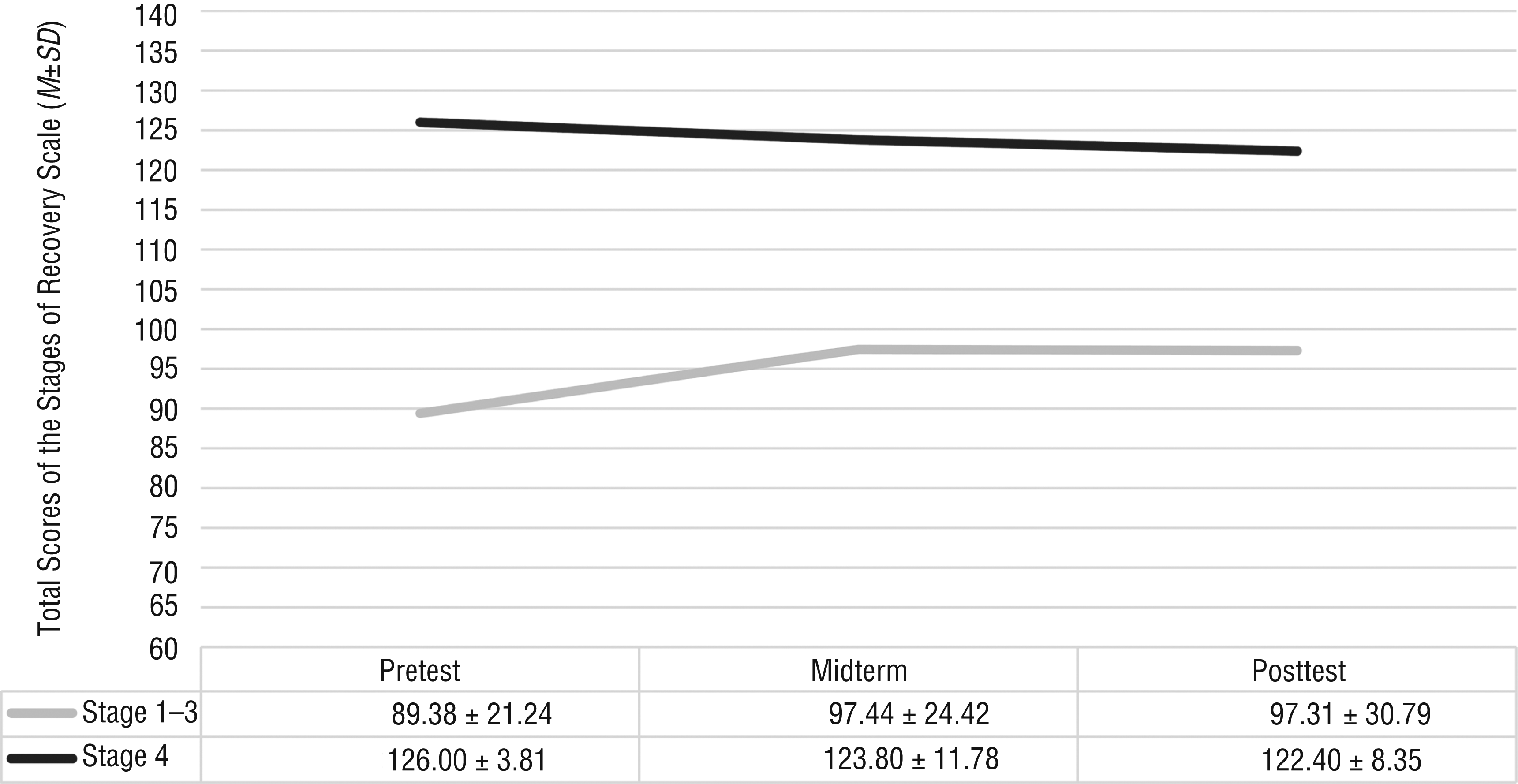
Total scores on the Stages of Recovery Scale at pretest, midterm, and posttest for the Stage 1–3 group and the Stage 4 group.
Stages of Recovery Scale Scores Among All Participants, Stage 1–3 Group, and Stage 4 Group
Note. M = mean; SD = standard deviation.
aThree participants were excluded from analysis as a result of incomplete posttest data.
Course Questionnaire
We merged disagree and strongly disagree responses into “disagree” and agree and strongly agree responses into “agree” to document overall agreement with each item (Table 3). Total mean scores for first- and second-phase course questionnaires were 4.37 (SD = 0.52) and 4.29 (SD = 0.59), respectively, showing participants’ high identification with the group. In general, more than 90% of the participants were satisfied with the group, with the majority of participants believing that the manual and homework were helpful to their learning, although the item “I can memorize key points of courses ” had lower agreement (69.6% for Phase 1; 72.7% for Phase 2). With respect to items specific to each phase, nearly all participants (87.5%–100%) in the first phase agreed that the group helped them understand recovery-related concepts. For the second phase, the majority reported that recovery stories and writing their own stories were positive and helped them to understand and accept themselves (87.0% and 95.0%, respectively).
Course Assessment Questionnaire Results
Note. n/a = not applicable.
Not all participants completed all items. For Phase 2, 1 participant did not fill out the posttest measures.
Qualitative Data
Three themes emerged from the qualitative data: recovery stage reflection, course suggestion, and recovery group impact. Regarding recovery stage reflection, participants reported different experiences. Some participants felt more positively about themselves, some had difficulty improving their recovery stages, and some described changes in their thoughts about recovery during the intervention:
I became more optimistic after the first-phase courses, which made me more accepting of my disease, but I felt it was not easy after the end of the second-phase curriculum. (Participant 19)
As regards course suggestion, participants had two main concerns. Some had difficulty understanding the concept of recovery. Some suggested adding content, such as recovery stories and the meaning of self-redefinition:
I would like more recovery stories that describe how those people who have had mental health issues went through their recovery process successfully. (Participant 4)
Recovery group impact was mainly positive. Participants stated that participation in the group helped them change their perception and increase their acceptance of the disease:
Learning from some cases [in the recovery stories] let me know that I am not alone, and some people are working hard for themselves. (Participant 2)
In the course, by setting my personal goals, I found my own advantages, so that I no longer feel inferior. Also, I no longer feel that I am just a patient. (Participant 4)
I have more confidence in myself and know how to plan the way to go in the future. (Participant 22)
Discussion
Our results confirm the feasibility of implementing a recovery group in Taiwan; course questionnaire scores showed that the majority of participants were satisfied with the group and agreed with the course content. During group development, we found that participants were unfamiliar with the Western concept of recovery. They requested more examples and exercises to help them better understand the concept. We therefore added recovery stories and role exploration exercises to the curriculum. Recovery stories received extensive, positive feedback from participants, as shown in group discussion and in their responses to the course questionnaire. Participants pointed out that such recovery stories helped them to understand that they are not alone and that recovery is possible. Moreover, role is one of four performance patterns identified in the Occupational Therapy Practice Framework: Domain and Process (3rd ed.; AOTA, 2014), and it has an impact on the selection of occupations. Role exploration helped participants learn about potential roles other than the patient role, thus raising their expectations for the future and allowing them to choose occupations corresponding to these potential roles as their recovery goals. After these adjustments, participants came to gradually understand mental health recovery and were able to more concretely imagine the recovery journey.
Previous recovery interventions conducted in Western countries have resulted in significant participant improvement on many related measures, such as those assessing empowerment, hopefulness, and symptoms (Barbic et al., 2009; Green et al., 2013; Thomas et al., 2018). Our participants showed similar improvement. The SRS was developed using indigenous samples in Taiwan, and scores on the SRS were used to assess participants’ recovery stage. As shown in Figure 1, the participants at Stage 4 showed a slight decline in scores but were still within the range of Stage 4. This phenomenon was consistent with the qualitative data. After intervention, participants realized that recovery could be a challenging process and that they might not be as successful in their recovery journey as they indicated at pretest. This realization might have been a factor in their decreased scores. Previous mental health recovery literature has rarely reported such feedback; participants are mostly requested to fill out measures without an opportunity to discuss any changes in their scores. Despite drops in scores, the intervention enhanced participants’ self-awareness and reflection, indicating that it had positive influence on their recovery process.
Green et al. (2013) suggested that groups that use PTR expand the curriculum to 17–18 wk, so that participants can have sufficient time to absorb and reflect on the contents. In our study, although the curriculum lasted 18 wk, it was actually 16 wk after the last session of each phase, which was used for testing and feedback, was removed. Given participants’ feedback and actual group performance, we advise lengthening both session time and the total number of weeks so that participants have more opportunity for practice and discussion. Because it takes time for recovery efforts to bear fruit (Chang et al., 2013; Spaniol et al., 2002), a longer course may be more beneficial to participants’ recovery, providing them with tools and ongoing support during their recovery journeys.
In addition, many studies have proved the feasibility and validity of joint professional–peer leadership for recovery groups (Barbic et al., 2009; Green et al., 2013; Thomas et al., 2018). However, because mental health recovery is still in the beginning stages in Taiwan, these programs need more time for professionals and peers to learn basic recovery concepts. As these leaders learn, more groups will emerge and thrive in Taiwan under joint leadership.
This study had several limitations. First, because of the small sample size and lack of a control group, the group’s effectiveness in improving participant outcomes cannot be determined. However, this was a feasibility study, and our goal was to understand whether Taiwanese people with mental illness would take part in such group and benefit from its curriculum. Therefore, program effectiveness was not the study’s focus (Tickle-Degnen, 2013). Second, our results are not generalizable to all Taiwanese people with mental illness. The majority of the participants were female, and they had a high level of education and were at a higher recovery stage. Thus, results may not be applicable to men and those with a lower level of education and at lower recovery stages. Third, the SRS was the only measure used. Additional measures should be used in future studies to assess self-esteem, social support, and hope to document the effect of such groups on people’s recovery.
Implications for Occupational Therapy Practice
The results of this study have the following implications for occupational therapy practice:
Indigenous recovery stories and role exploration may help people with mental illness in non-Western countries understand recovery more easily, boosting learning effects.
Recovery programs tailored to people with mental illness in non-Western countries may need more and longer sessions for participants to fully understand and implement the concepts of recovery.
Because recovery is an ongoing process, we suggest collecting not only quantitative data but also qualitative data to faithfully show the effects of a recovery group on participants.
Conclusion
This study affirmed the feasibility of recovery programs for Taiwanese people with mental illness. It showed that participants were satisfied with the recovery program and that the program might improve their recovery status. Randomized controlled trials with multiple evaluation tools and follow-up tracking should be carried out to verify the effectiveness of such recovery groups.
Footnotes
Acknowledgments
We thank the study participants for the time and effort they contributed to this study.
Weekly Group Topics
| Phase 1: Recovery Profile | Phase 2: Recovery Plan |
| 1. Introduction • Introducing the strengths approach • Pretest |
1. My Life, My Role • Identifying personal roles • Vision for personal recovery |
| 2. Gearing Up for the Journey: Hope • Instillation of hope • Strategies for creating hope |
2. Setting a Course for the Recovery Journey • Forming long-term goals • Setting successful short-term goals • Steps to reach these goals |
| 3. Gearing Up for the Journey: Courage • Definition of courage • Building courage |
3. Social Support for the Journey • Exploring and applying social support • Expanding supportive relationships |
| 4. Taking the First Step With Courage • Risk assessment • Changing negative self-talk |
4. Recovery Plan Check • Checking how the plan goes • Revising the personal recovery plan |
| 5. Setting Ourselves in Motion • Motivation • Self-responsibility for recovery • Turnaround toward recovery |
5. Making It Past Detours and Roadblocks • Identifying difficulties during the recovery journey • Working through the roadblocks |
| 6. Recovery Is Self-Discovery: Recognizing Our Strengths I • Changing orientation from negative to positive |
6. Rest Stops and Travel Tips • Stress management • Flexibility and adaptability • Supercharging the recovery journey |
| 7. Recovery Is Self-Discovery: Recognizing Our Strengths II • Strategies for identifying strengths • Completing my strength map |
7. Our Stories of Recovery I • The value in sharing • Writing the personal journey of recovery |
| 8. Recovery Profile • Program integration and review |
8. Our Stories of Recovery II • Sharing the personal journey of recovery |
| 9. Celebration • Feedback on the program • Midterm test |
9. Celebration • Feedback on the program • Posttest |