
Abstract
In 2010, the World Health Organization (WHO; 2013) estimated that 285 million people were living with visual impairment. In 2018, WHO estimated that 1.3 billion people were living with some type of visual impairment, the majority over age 50. WHO categorized this population as follows: for distance vision, 188.5 million people with mild visual impairment, 217 million with moderate to severe visual impairment, and 36 million with blindness, and for near vision, 826 million people with visual impairment (WHO, 2018). Low vision, a classification of visual impairment, affects near and distance vision, creating challenges for older adults’ engagement in leisure and social participation.
The American Occupational Therapy Association (AOTA; 2014) described leisure and social participation as intrinsically motivating activities that support engagement in the community with family and friends. Low vision affects the ability to see family, friends, and everyday items in the home and community, challenging the participation of older adults with low vision in leisure and social activities. Older adults with low vision who have not received rehabilitation have been found to limit their physical and social life spaces (Rudman et al., 2010).
Engagement in leisure and social participation in the home and community helps promote overall health and well-being (Nastasi, 2018; Smallfield & Lucas Molitor, 2018). Thus, interventions that support social and leisure occupations are recommended as routine care for older adults (Smallfield & Lucas Molitor, 2018).
In 2013, Berger and colleagues completed a systematic review examining the effectiveness of interventions to improve leisure and social participation for older adults with low vision. They found strong evidence for using a problem-solving approach and moderate evidence for delivering a combination of services to maintain, restore, and improve leisure and social participation. Mixed evidence was found for providing skills training and making home visits and environmental adaptations. Their findings and the findings of related systematic reviews are available in the Occupational Therapy Practice Guidelines for Older Adults With Low Vision (Kaldenberg & Smallfield, 2013). The purpose of the current systematic review was to update the evidence for the effectiveness of interventions within the scope of occupational therapy practice to maintain, restore, and improve performance and quality of life in leisure and social participation for older adults with low vision.
Method
This systematic review is one of three updated reviews of the literature on older adults with low vision undertaken as part of AOTA’s Evidence-Based Practice (EBP) Project (see also Liu & Chang, 2020, and Smallfield & Kaldenberg, 2020, in this issue). The author followed the protocol established by the EBP Project for the systematic reviews on this topic (Arbesman et al., 2013), as well as the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA–P; Moher et al., 2015). The research question, search terms, and methodology were developed by two research methodologists at AOTA, AOTA staff, an advisory group, and the review authors. A medical librarian searched the key words used in Berger et al.’s (2013) previous systematic review on this topic as well as additional words added for this review (Table 1). MEDLINE, PsycINFO, CINAHL, OTseeker, and the Cochrane Database of Systematic Reviews were searched, and hand searching of bibliographies and journals was also completed as needed. Citations were initially reviewed by the AOTA research methodologists and provided to the author, who then reviewed the articles with two other researchers, with support from the AOTA research methodologists, with respect to level of evidence, quality, risk of bias, and significance of findings.
Search Terms for Leisure and Social Participation for Older Adults With Low Vision
Suggested citation: Nastasi, J. A. (2020). Occupational therapy interventions supporting leisure and social participation for older adults with low vision: A systematic review (Table 1). American Journal of Occupational Therapy, 74, 7401185020. https://doi.org/10.5014/ajot.2019.038521
Inclusion and Exclusion Criteria
Inclusion criteria for this review were as follows: peer-reviewed articles providing Level I, II, and III evidence published in English between January 2010 and March 2017 that addressed intervention approaches within the scope of practice of occupational therapy specific to leisure and social participation for older adults with low vision (mean [M] age = ≥55). Level I studies include systematic reviews, meta-analyses, and randomized controlled trials; Level II studies include two-group, nonrandomized designs; and Level III studies include one-group, nonrandomized designs. Excluded were articles presenting Level IV (descriptive studies) and Level V (case reports and expert opinion) evidence, presentations, conference proceedings, non–peer-reviewed literature, dissertations, theses, interventions outside the occupational therapy scope of practice, research published outside the dates of inclusion, and studies with samples with a mean age of <55 yr.
Data Extraction and Risk of Bias
The author and two additional researchers evaluated all articles through all stages of the review, identifying the level of evidence and rationale for inclusion and exclusion of each. An evidence table was created for the three articles included in the review listing authors, year of study, level of evidence, study design, participant inclusion criteria, intervention and control conditions, outcome measures, and results (Table 2, at the end of this article). The AOTA research methodologists reviewed the master citation table and evidence table for quality control. Risk of bias was evaluated for the studies using the Cochrane risk-of-bias guidelines (Higgins et al., 2011; Table 3, at the end of this article). Risk of bias ranged from low to high, with an overall high risk of bias. Selection bias, performance bias, and detection bias were high for all three studies. Attrition bias and reporting bias were low except for the study by Renieri et al. (2013), which had high attrition bias.
Evidence Table for Leisure and Social Participation for Older Adults With Low Vision
Note. HADS = Hospital Anxiety and Depression Scale; M = mean; MMSE = Mini-Mental Status Examination; PFGP = Progression of the Functional Global Profile.
This table is a product of AOTA’s Evidence-Based Practice Project and the American Journal of Occupational Therapy. Copyright © 2020 by the American Occupational Therapy Association. It may be freely reproduced for personal use in clinical or educational settings as long as the source is cited. All other uses require written permission from the American Occupational Therapy Association. To apply, visit www.copyright.com.
Suggested citation: Nastasi, J. A. (2020). Occupational therapy interventions supporting leisure and social participation for older adults with low vision: A systematic review (Table 2). American Journal of Occupational Therapy, 74, 7401185020. https://doi.org/10.5014/ajot.2019.038521
Risk-of-Bias Table
Note. Categories for risk of bias are as follows: + = low risk of bias; – = high risk of bias. Risk-of-bias table format adapted from “Assessing Risk of Bias in Included Studies,” by J. P. T. Higgins, D. G. Altman, and J. A. C. Sterne, in Cochrane Handbook for Systematic Reviews of Interventions (Version 5.1.0), by J. P. T. Higgins and S. Green (Eds.), 2011, London: Cochrane Collaboration. Retrieved from http://handbook-5-1.cochrane.org. Copyright © 2011 by The Cochrane Collaboration.
Suggested citation: Nastasi, J. A. (2020). Occupational therapy interventions supporting leisure and social participation for older adults with low vision: A systematic review (Table 3). American Journal of Occupational Therapy, 74, 7401185020. https://doi.org/10.5014/ajot.2019.038521
Analysis and Synthesis
The U.S. Preventive Services Task Force (2013) definitions for level of certainty (i.e., strength of evidence) were used to classify the evidence as a whole as strong, moderate, or low. Strong evidence indicates two or more well-designed Level I studies. Moderate evidence indicates at least one high-quality Level I study or multiple moderate-quality studies. Low evidence indicates a small number of studies with inconsistent findings or flaws. Strength of evidence was determined for this systematic review using these definitions.
Results
The database search yielded 10,549 articles, of which 455 were screened after removal of inappropriate articles (e.g., did not describe research, low vision, or older adults). Five duplicate articles were removed, and 447 were excluded during screening because they were not relevant to the research question (Figure 1). Three studies were included in this systematic review, and all addressed social participation; no articles were found that addressed leisure.
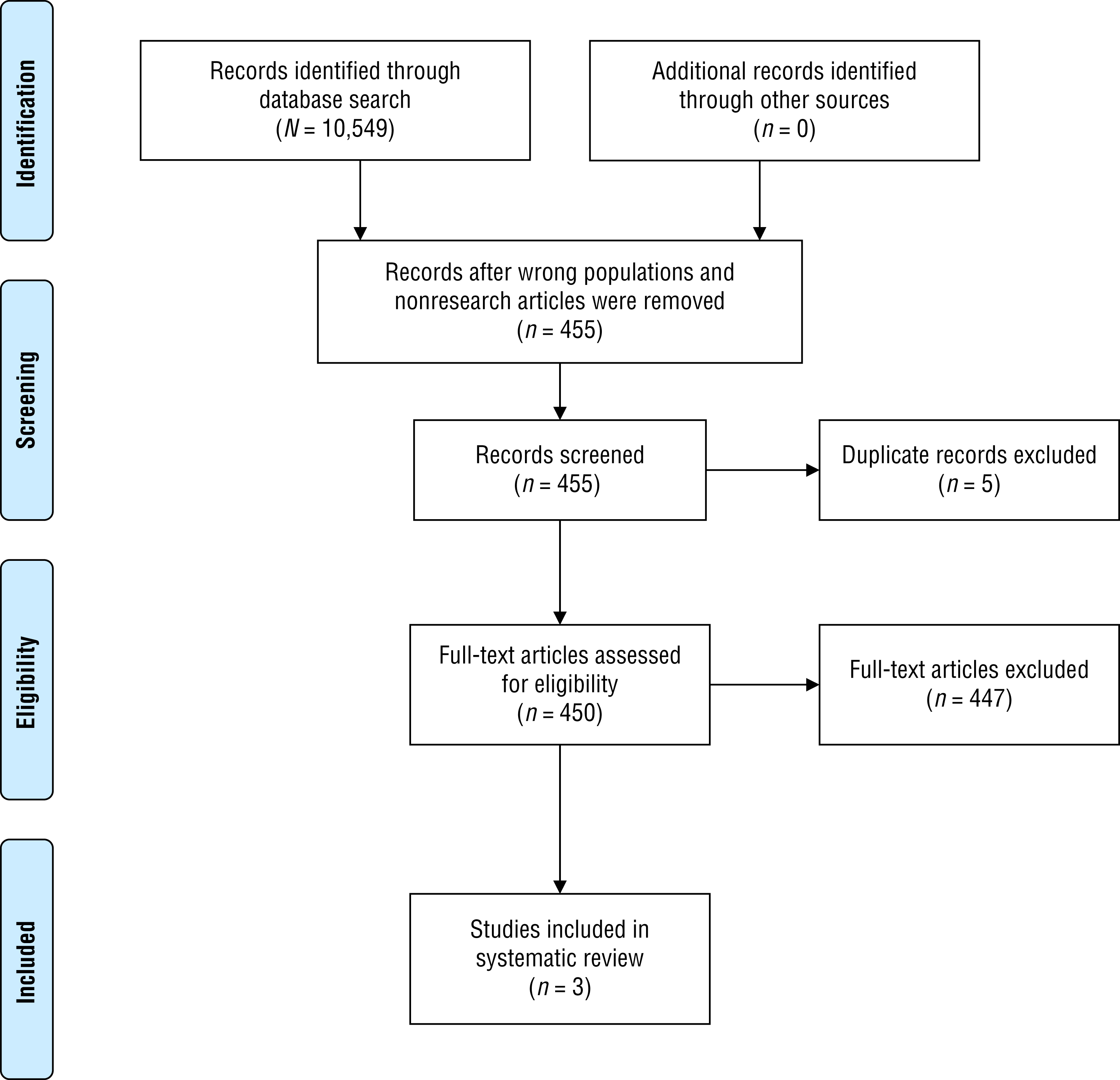
Flow of articles through the selection process.
The 3 articles provide Level III evidence (Alma et al., 2012; Coulmont et al., 2013; Renieri et al., 2013). The studies included 217 participants with a mean age of 77.89. All studies included both male and female participants, with 62.8% being female, and all participants were identified as having low vision. Together the studies provide low strength of evidence and high risk of bias but produced statistically significant findings that group therapy, more hours of direct service provided over a shorter duration, and fitting with low vision devices had positive effects on social participation.
Coulmont et al. (2013) recruited 100 participants with low vision enrolled in a rehabilitation program. The researchers studied hours of direct services provided, hours of indirect services provided, and hours of service related to both services and intervention plans. The Progression of the Functional Global Profile (PFGP) was used as an outcome measure at the beginning and end of the program. Regression analysis showed significant findings (in order of importance) for more hours of direct services provided (M = 13.23 hr, standard deviation [SD] = 9.82), younger age (M age = 81.76 yr, SD = 7.18), shorter duration of services, more hours of direct services over a shorter duration, and female gender. More hours of service provided in a shorter period of time contributed to higher scores on the PFGP, providing evidence that clinical intervention can improve the quality of social participation for older adults with low vision.
Renieri et al. (2013) interviewed 88 participants with low vision 3 mo after low vision rehabilitation that included being fitted for magnifying devices, provided vision aids, and given suggestions on managing daily care activities. The researchers used the Modified German National Eye Institute Visual Functioning Questionnaire 25-item version (National Eye Institute, 2000), Hospital Anxiety and Depression Scale (Zigmond & Snaith, 1983), Mini-Mental Status Examination Blind (Busse et al., 2002), and Indicators of Rehabilitation Status (Gerdes & Jäckel, 1995) as outcome measures. Renieri et al. found significant improvement in perceptions of social functioning, as well as near tasks and reading abilities, for participants fitted with low vision devices including magnifying devices and vision aids.
Alma et al. (2012) recruited 29 participants with visual impairment to participate in 2-hr weekly meetings over 20 wk consisting of four components: (1) practical training; (2) education, social interaction, counseling, and training in problem-solving skills; (3) individual and group goal setting; and (4) a home-based exercise program. A booster session was completed 12 wk after program completion. Outcomes were measured using the Utrecht Scale for Evaluation of Rehabilitation–Participation (van der Zee et al., 2010) and the Impact on Participation and Autonomy questionnaire (Cardol et al., 1999) at baseline, postintervention, and 6-mo follow-up. No significant changes were found over time at the instrument level; however, at the item level, significant findings were found in frequency of housekeeping and outdoor activities and in satisfaction with partner relationships.
Overall, low strength of evidence is available to support the effects of low vision rehabilitation on social participation. Providing fitted low vision devices and providing clients with opportunities to interact with others helped decrease isolation and increase confidence in social participation.
Discussion
Since the previous systematic review (Berger et al., 2013), few studies have been published on interventions addressing leisure and social participation for older adults with low vision. The previous review covered a longer period (1990–2010) than the current review (2010–2017) and included 13 articles compared with 3 in the current review. More research is needed on occupation-based interventions to promote leisure and social participation for older adults with low vision.
Evidence from this review provides additional support for problem-solving approaches (Alma et al., 2012), delivery of a combination of services (Coulmont et al., 2013), skills training (Alma et al., 2012; Renieri et al., 2013), and environmental adaptations (Alma et al., 2012; Renieri et al., 2013). No additional evidence was found to support making visits to the home, an intervention highlighted in the past review (Berger et al., 2013). More research needs to be conducted on interventions to maintain, restore, and improve performance and quality of life in leisure and social participation for older adults with low vision because these occupations support engagement in the community with family and friends and are recommended as routine care for older adults (AOTA, 2014; Smallfield & Lucas Molitor, 2018).
Implications for Occupational Therapy Practice, Research, and Education
The findings of this review have the following implications for occupational therapy practice, research, and education:
The evidence supports providing fitted low vision devices (magnifying devices and vision aids) to improve confidence and social participation for older adults with low vision.
Future well-designed studies addressing leisure and social participation for older adults with low vision are needed that focus on occupation-based interventions to improve functional outcomes and sensitive outcome measures.
Occupational therapy educational programs should include content on interventions and outcome measures addressing leisure and social participation for older adults with low vision. In addition, students need to be prepared to conduct research on leisure and social participation with this population.
Limitations
The findings of this systematic review are limited by the limitations of the individual studies. All studies provide Level III evidence with high risk of bias. The interventions varied across studies, and outcomes were measured with a variety of measures.
Conclusion
The evidence continues to provide limited support for interventions to improve leisure and social participation for older adults with low vision. Although this systematic review found additional evidence supporting such interventions, this evidence has low strength and high risk of bias. Further research in this area is critical to support interventions to improve leisure and social participation for older adults with low vision.
Footnotes
Acknowledgments
I thank Elizabeth Hunter and Deborah Lieberman for their support throughout the systematic review. I also thank Elizabeth Masci and Chelsea Blair, who completed the systematic review with me.
*
Indicates articles included in the systematic review.