
Abstract
Cannabinoids, which are compounds derived from the cannabis plant, have become an international topic of much interest and controversy. Although cannabis is classified as a Schedule I drug, which is a designation for substances at high risk for abuse and lack of medical use, the plant has been recognized for its therapeutic potential and legalized for medicinal purposes in 33 states, the District of Columbia, Guam, and Puerto Rico. It has also been legalized for recreational purposes in nine states (National Conference of State Legislatures [NCSL], 2019, 2020; U.S. Drug Enforcement Agency, n.d.). Along with legalization of recreational and medicinal cannabis, researchers have started to consider how cannabinoids effect quality of life (QoL). Despite limited research and federal restrictions, it has been suggested that the therapeutic properties of cannabinoids influence QoL and alleviate symptoms associated with a range of conditions and diseases (Davison & Davison, 2011; Fiz et al., 2011; Goldenberg et al., 2017; NCSL, 2019).
Cannabis research is limited, however, because of a multitude of factors, such as the lack of suitable medicinal cannabinoid products and availability of potent cannabis sold illegally or by dispensaries; lack of large randomized controlled trials; federal restrictions; lack of alternative delivery methods and understanding of current delivery systems; lack of knowledge and basic understanding of the endocannabinoid system (ECS) and therapeutic potential of cannabinoids within the health care profession, politics, and media; and the high costs of medicinal cannabinoids versus the low cost of recreational cannabis (Braun et al., 2017; NCSL, 2020; Notcutt, 2015). In fact, only two cannabinoid medications are approved in the United States: nabilone and dronabinol (which are pills classified as synthetic cannabinoids). Nabiximol, a nonsynthetic cannabinoid medication comprising both δ-9 tetrahydrocannabinol (THC) and cannabidiol (CBD) in a 1:1 ratio currently undergoing further research, is an oromucosal spray with a quicker onset of action than nabilone and dronabinol (Notcutt, 2015).
Evidence suggests that nonsynthetic cannabinoids may have more therapeutic potential than currently approved synthetic cannabinoid medications and opioids because of a faster onset of action and less severe side effects (Braun et al., 2017; Notcutt, 2015). In addition, the therapeutic effects of cannabis vary depending on the strain of cannabis and cannabinoid concentration (Lusk & Rutherford Owen, 2017). Subsequently, people may experience adverse effects associated with cannabinoids because of lack of knowledge and understanding regarding the purity, concentration, and cannabis strain from which the nonsynthetic cannabinoid is derived. Moreover, little to no research specifically has investigated the influence of cannabinoids on occupational engagement, although a dynamic relationship between occupation and QoL has been shown.
Therefore, a scoping review was conducted to investigate the impact of cannabinoids on QoL and occupation of recreational and medicinal users. The aforementioned terms are defined according to the Occupational Therapy Practice Framework: Domain and Process (3rd ed.; OTPF–3; American Occupational Therapy Association [AOTA], 2014), which encapsulates the interrelated constructs of the occupational therapy profession. QoL is defined as the “dynamic appraisal of life satisfaction (perception of progress toward identified goals), self-concept (beliefs and feelings about oneself), health and functioning (e.g., health status, self-care capabilities), and socioeconomic factors” (AOTA, 2014, p. S45). Occupation is described as purposeful engagement in day-to-day activities that occur within a particular context across the following eight domains: activities of daily living (ADLs), instrumental activities of daily living (IADLs), work, education, rest and sleep, leisure, play, and social participation (AOTA, 2014).
Method
A scoping review was selected for this topic because of the limited research regarding the influence of cannabinoid use on QoL and occupation. Therefore, the scoping review was conducted in accordance with the five stages developed by Arksey and O’Malley (2005). Stage 1 entails identification of the research question. Stage 2 involves the identification of relevant studies, which answers the research question. Stage 3 is the selection of relevant studies, including review of full articles. Stage 4 consists of extracting and charting the key data derived from the selected research articles. Stage 5 entails collating, summarizing, and reporting the results of the review. The purpose of this scoping review is to answer the following two research questions:
What is the short- and long-term impact of nonsynthetic recreational and medicinal cannabinoids on QoL in adults?
What is the short- and long-term impact of nonsynthetic recreational and medicinal cannabinoids on occupation in adults?
The search strategy involved a literature search conducted by both authors of this scoping review. Databases searched included Ovid and CINAHL; sources derived from a manual search of reference lists were also used. We identified a total of 691 articles using the following two key terms: (1) cannabis AND quality of life and (2) cannabinoids AND quality of life. The database search yielded a total of 22 articles that met the inclusion and exclusion criteria for this scoping review (Figure 1). The included studies are summarized in Appendix A. The inclusion criteria were English language, clear focus or description of the impact of nonsynthetic cannabinoids on QoL and aspects of occupation, and published between January 2011 and May 2019. Exclusion criteria were articles that included studies that discussed the impact of cannabinoids on people younger than age 18 yr, single case studies, and animal studies; antineoplastic articles and articles that only discussed or investigated effects of synthetic cannabinoids were also excluded.
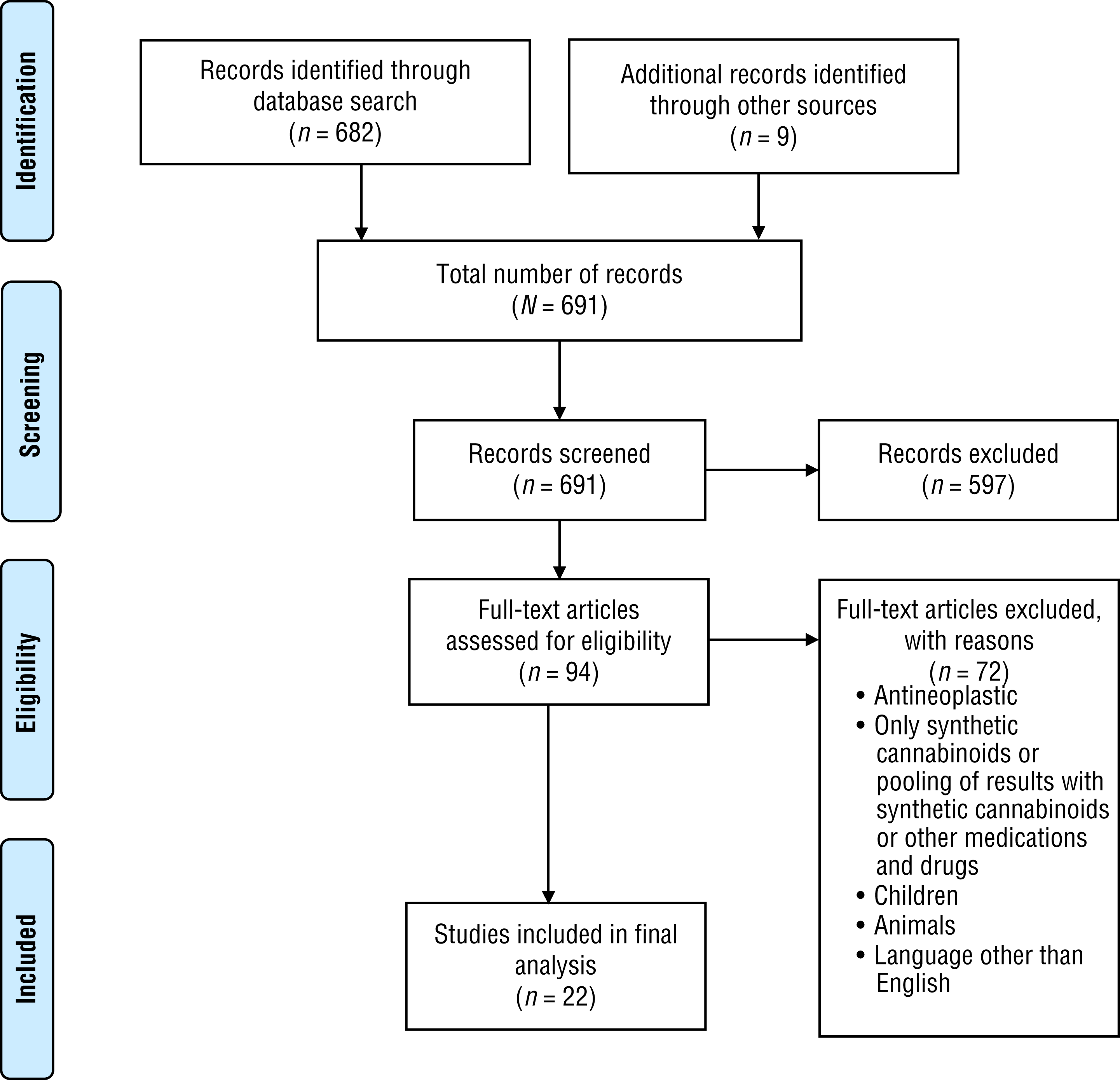
Flow diagram for inclusion and exclusion of peer-reviewed studies in the scoping review.
Results
Quality of Life
Multiple studies have investigated the impact of cannabinoid use on QoL with a specific focus on symptom and pain management (Fiz et al., 2011; Haroutounian et al., 2016; Johnson et al., 2013; Lynch et al., 2014; McKenzie et al., 2018; Portenoy et al., 2012; Russo et al., 2016; Vigil et al., 2017). However, the research regarding the impact of nonsynthetic cannabinoids on QoL is rather limited. In addition, because QoL is multifaceted, it is influenced by variables such as pain management. Therefore, cannabinoid research often associates QoL with efficacy of pain control. Thus, 6 out of the 22 identified studies indicated an increase in QoL for people with a medical diagnosis in which nonsynthetic cannabinoids were associated with effective pain management (Fiz et al., 2011; Haroutounian et al., 2016; Johnson et al., 2013; McKenzie et al., 2018; Russo et al., 2016; Vigil et al., 2017).
The following medical diagnoses were associated with cannabinoids alleviating pain and improving QoL: fibromyalgia and other pain disorders, various forms of cancer, musculoskeletal disorders, irritable bowel disease, and multiple sclerosis (MS; Fiz et al., 2011; Haroutounian et al., 2016; Johnson et al., 2013; McKenzie et al., 2018; Russo et al., 2016; Vigil et al., 2017). However, 2 studies indicated no significant difference in QoL as a result of pain management between treatment and placebo groups (Lynch et al., 2014; Portenoy et al., 2012). Last, as previously mentioned, QoL is multifaceted and therefore associated with occupation in areas other than pain management. For instance, 1 study reported that cannabis helped the majority of the study participants maintain function and QoL by improving their ability to work, increasing life satisfaction and productivity, reducing anxiety, and increasing appetite (Aggarwal et al., 2013). In another study, significant reductions in spasticity, which is a client factor that influences occupational engagement, were associated with significant improvements in QoL (Russo et al., 2016).
Currently, research regarding recreational use of cannabinoids is also limited, even more so than medicinal cannabinoid research. In fact, only 1 article (Morgan et al., 2012) addressed the impact of nonsynthetic cannabinoids on psychological well-being, an aspect of QoL. Morgan et al. (2012) found that high concentrations of THC negatively influenced psychological well-being and instead increased feelings of depression and anxiety. Conversely, the results of the same study indicated that CBD helped reduce psychosis-like symptoms associated with the use of THC, ultimately reducing instances of anxiety and depression. The increased instances of psychosis-like symptoms in recreational users may be attributed to the fact that recreational cannabis generally contains a higher THC concentration than medicinal cannabis (Davison & Davison, 2011; Morgan et al., 2012). Moreover, recreational cannabis is likely to be illicit, and therefore the quality and composition of the product are unknown (Braun et al., 2017; Notcutt, 2015).
Cannabinoids and Occupation
As previously mentioned, occupation consists of eight domains, and occupational engagement is influenced by multiple factors, which include contextual and environmental factors, client factors, performance skills, and performance patterns (AOTA, 2014). Moreover, medicinal cannabinoids are generally used to manage symptoms associated with various diseases and illnesses that affect occupational engagement. Therefore, multiple studies have assessed the impact of cannabinoids on occupations such as sleep, ADLs, and IADLs.
Activities of Daily Living and Instrumental Activities of Daily Living
Pain was discussed in the previous section in association with QoL. However, pain is specifically associated with the IADL occupational domain as a form of health management and maintenance. Health management and maintenance encompass multiple aspects of health and wellness promotion, which also include pain control and medication routines (AOTA, 2014). Thus, more than half of the articles included in this review address the influence of nonsynthetic cannabinoids on pain management. Eight studies found that cannabinoid use resulted in either statistically or clinically significant pain reduction in study participants (Fiz et al., 2011; Haroutounian et al., 2016; Johnson et al., 2013; Lynch et al., 2014; McKenzie et al., 2018; Portenoy et al., 2012; Russo et al., 2016; Vigil et al., 2017).
Similarly, 4 studies explored the perceptions of people who are medically ill and health professionals on medicinal cannabinoid use (Braun et al., 2017; Heng et al., 2018; Khelemsky et al., 2017; Lal et al., 2011). Overall, these 4 studies indicated that participants perceived that cannabinoids may be used to alleviate pain in people with a range of medical conditions and illnesses. Conversely, when the efficacy of pain management in the cannabinoid treatment group was compared with placebo groups, 2 studies reported no notable difference between the two groups (Lynch et al., 2014; Portenoy et al., 2012). In addition, only 1 of the 22 articles suggested that cannabinoids insufficiently alleviated pain and therefore did not recommend cannabinoids as a pain management technique (Martellucci et al., 2015).
Another topic in cannabinoid research is appetite, which is associated with the client factor of energy and drive. Appetite influences both the ADL and IADL domains of occupation because it is an aspect of both feeding (ADL) and meal preparation (IADL; AOTA, 2014). Thus, research has indicated an association between nonsynthetic cannabinoid use and increased appetite in people with a medical diagnosis or illness (Aggarwal et al., 2013; Braun et al., 2017; Lal et al., 2011; Martellucci et al., 2015; McKenzie et al., 2018).
In addition, bladder function is another client factor addressed in cannabinoid research. According to the OTPF–3, bladder functions are associated with the ADLs of toileting and toilet hygiene (AOTA, 2014). Thus, the mini review by Sevilla Guerra (2012) suggested that cannabinoids were effective in treating bladder dysfunction, urge incontinence, nocturia, void urgency, and void frequency in people with MS.
Sleep
Cannabinoid research has also been associated with the occupational domain of rest and sleep, with a specific focus on sleep. Rest and sleep entail sleep preparation and sleep participation (AOTA, 2014). These areas of sleep may be negatively affected by symptoms associated with certain medical conditions. Thus, the research has suggested that nonsynthetic cannabinoids may be used to effectively treat sleep disorders and improve sleep participation (Babson et al., 2017; Braun et al., 2017; Haroutounian et al., 2016; Lichtman et al., 2018; Martellucci et al., 2015). Conversely, 3 studies associated no improvements in sleep and impaired sleep with long-term use of THC and high doses of nabiximol (Babson et al., 2017; Lichtman et al., 2018; McKenzie et al., 2018).
Recreational Cannabinoids and Occupation
The research regarding recreational cannabinoids and their impact on occupation is rather limited. Only 3 articles addressed the influence of recreational cannabinoids on aspects of occupation (driving, health management and maintenance, and rest and sleep; Asbridge et al., 2012; Lacey et al., 2016; Pedersen & Sandberg, 2013). Pedersen and Sandberg (2013) reported that 25% of participants used cannabis explicitly for medicinal purposes, although none of the participants were approved for legal use of cannabinoids. Therefore, the distinction between recreational and medicinal is unclear in that study. However, participants reported using cannabis for relaxation; treating insomnia, stress, and pain; and mitigating symptoms associated with MS, Tourette’s syndrome, and severe rheumatism.
The effects of cannabinoid use on driving is within the scope of occupational therapy practice as an IADL. Specifically, practitioners address the underlying cognitive, physical, and psychosocial skills necessary to promote safe driving and participation across the lifespan (AOTA, 2017). In addition, occupational therapy practitioners are nationally recognized as driving rehabilitation specialists (Carr et al., 2010). However, research regarding the impact of cannabinoids on driving to date has been elusive. In fact, only a few countries have a variation in laws regarding cannabis use and driving for medicinal and recreational users. Much of the research has been inconclusive and conducted across Europe in controlled settings incongruous with real-world scenarios.
Nonetheless, studies have suggested a relationship between illicit cannabis use and increased motor vehicle collisions, although other studies have found no connection between the two variables (Asbridge et al., 2012; Notcutt, 2015). For instance, the systematic review completed by Asbridge et al. (2012) suggested that acute use of THC was significantly associated with an increased risk of a motor vehicle collision, which almost doubled in comparison with unimpaired driving. However, the National Highway Traffic Safety Administration, a consumer agency, conducted a case control study that suggested that no significant increase in crash risk was associated with the use of THC (Lacey et al., 2016).
Discussion
More research and evidence are available on the medicinal use of cannabis than on recreational use. However, on the basis of the inconclusive and limited research, it is evident that further exploration into the therapeutic potential of cannabinoids, their influence on QoL and occupation, and the long-term effects of cannabis use on QoL and occupation is necessary. In the studies included in this review, QoL, in most instances, was described in addition to pain management. In addition, although areas of occupation were addressed, no literature directly addressed the impact of cannabis on occupational engagement from an occupational therapy perspective. Primary aspects of occupation identified in the literature other than pain management were sleep, appetite, and bladder function. Work was also mentioned in 1 study (Aggarwal et al., 2013).
Note that the distinction between recreational and medicinal cannabis was obscured. Therefore, the following questions arise: What defines medicinal cannabis use? Does it constitute a diagnosis and prescription from a physician? What about the people who use cannabis to treat condition-associated symptoms but lack the funds to forgo an evaluation for medicinal cannabis? Sagar and Gruber (2018) suggested that recreational users primarily seek out THC (psychoactive), whereas medicinal users seek out other cannabinoid products that often contain high levels of CBD (nonpsychoactive). However, Pedersen and Sandberg (2013) suggested that recreational cannabis users also use cannabis for medicinal purposes. Therefore, clearer definitions of recreational cannabis and medicinal cannabis are necessary: Recreational consumers may be self-treating certain conditions because of lack of access to health care or for financial reasons instead of using cannabis for a psychoactive effect.
Moreover, society has historically associated cannabinoids with crime, criminal sanctions, harm, vulnerability, and illicit drug abuse (Bottorff et al., 2013; Cousijn et al., 2018; Szaflarski & Sirven, 2017). It is clear that the social stigma associated with cannabinoids continues, despite an increase in legalities and accessibility. Therefore, people who use cannabinoids also run the risk of experiencing self-stigma, which has recently been associated with the substance abuse of opioids and heroin (Chang et al., 2019; Cheng et al., 2019). In addition, the terminology used to describe cannabinoid use should be evaluated. To integrate cannabinoids into the health profession, researchers and practitioners must start using scientific and medical language instead of terms that diminish the potential therapeutic properties of cannabis.
Research comparing the use of nonsynthetic cannabinoids with traditional pain management and medication practice is warranted. Currently, the leading cause of preventable deaths in the United States is opioid drug overdose (Vigil et al., 2017). Therefore, alternative pain management options, such as cannabinoids, may help combat the U.S. opioid crisis. In addition, health professionals must establish contraindications and guidelines for medicinal use of cannabinoids. The numerous types of cannabinoids vary in effectiveness and tolerability, and often the composition of illicit cannabinoids is unknown; these factors make identifying the impact of cannabinoids on QoL and occupation difficult (Braun et al., 2017; Karst & Passie, 2018). Although the effects of cannabinoid use on cognitive function in healthy people has been studied historically, further research is warranted because of increased knowledge regarding the various types of cannabinoids and the ECS. The ECS consists of cannabinoid Type 1 and cannabinoid Type 2 receptors that aid in the process of inflammation, neural development, and pain throughout the immune, central, and peripheral nervous systems (Khaiser et al., 2016).
Moderate evidence suggests a statistical association between cannabis use and impairment in learning, memory, and attention. However, limited evidence exists regarding impaired academic achievement and educational outcomes, work as it relates to unemployment and low income, and impaired social engagement (National Academies of Sciences, Engineering, and Medicine, 2017). Moreover, adverse effects can potentially be prevented if consumers and health professionals have more knowledge about the physiological effects of cannabinoids and how they interact with the ECS.
In addition, adverse effects can be minimized by evaluating the quality of the product, specifically, cannabinoid type, cannabinoid concentration, cannabis plant strain, and most appropriate method of intake. Subsequently, Notcutt (2015) suggested that the following parameters should be implemented to evaluate cannabinoid usage: “pattern of dosing, target symptoms evaluation, side effect assessment, patient’s activities of daily living, caregiver’s activities of daily living, and changes to other medications” (p. 775). Finally, future research should explore the use and appropriateness of cannabinoids in acute care and inpatient settings, because none of the articles in this scoping review addressed cannabinoid use in these environments.
Implications for Occupational Therapy Practice
The results of this scoping review have the following implications for occupational therapy practice:
Because of increased interest in cannabis and cannabinoids, occupational therapy practitioners may encounter people who either use cannabis medicinally or recreationally. Although occupational therapy practitioners do not prescribe medications, they have the knowledge and skills to promote occupational engagement as well as effective pain and medication management.
According to Maida and Daeninck (2016), optimal client outcomes in cannabinoid therapy may be accomplished through interprofessional collaboration that includes the prescribing physician, nurses, social workers, rehabilitation therapists, and pharmacists.
As part of the rehabilitation team, occupational therapy practitioners have the potential to provide education regarding cannabis use and monitor how it affects occupational engagement and QoL for both recreational and medicinal users.
Occupational therapy practitioners may play a vital role in both medication and pain management for clients who use cannabinoids by assessing how their current pain management techniques and medications affect occupational engagement and QoL.
Conclusion
Cannabinoids have the potential to influence QoL and occupational engagement; however, further research is warranted. Unfortunately, cannabinoid research is limited in scientific, clinical, and economic development because of decades of misrepresentation as solely a psychoactive agent and related restrictions on cannabinoid use (Karst & Passie, 2018). Although cannabinoid use restrictions remain in place, occupational therapy practitioners may encounter clients who use cannabinoids for recreational or medicinal purposes. Thus, practitioners should be mindful of the impact of cannabinoids on QoL and occupation. Last, because of practitioners’ expertise in occupational engagement, they have the opportunity to be at the forefront of research to address the gap in the literature regarding the influence of cannabinoids on occupation.
Footnotes
Acknowledgments
This scoping review was done in partial completion for the residency experiential component of the entry-level Doctor of Occupational Therapy Program at Nova Southeastern University (Tampa, FL).
Articles on the Impact of Recreational and Medicinal Cannabinoids on QoL and Occupation Included in the Scoping Review
| Author/Year | Study Design and Participants | Study Setting | Recreational or Medicinal | QoL or Occupation | Results |
|---|---|---|---|---|---|
| Aggarwal et al. (2013) |
Prospective longitudinal observational study Various diagnosed illnesses and diseases, N = 37 |
Washington State dispensary | Medicinal | Both | 80% reported medicinal marijuana helped maintain functional status and QoL improvements in ability to work, increased life satisfaction and productivity, decreased anxiety, and increased appetite. |
| Asbridge et al. (2012) |
Systematic review N = 9 |
N/A | Recreational | Occupation |
Most studies found acute use of THC was significantly associated with an increased risk of a motor vehicle collision. The risk of a motor vehicle collision resulting in severe injuries or fatalities was almost doubled in comparison with unimpaired driving. The influence of acute cannabis use on minor motor vehicle collisions was vague. |
| Babson et al. (2017) |
Systematic review Patients with sleep disorders, N = 23 |
N/A | Medicinal | Occupation |
CBD may be a potential therapeutic treatment option for insomnia, REM sleep behavior disorder, and excessive daytime sleepiness. THC was found to potentially decrease sleep latency. Long-term use of THC may impair the quality of sleep. |
| Braun et al. (2017) |
Qualitative study Medicinal marijuana and oncology experts, N = 15 |
Nationwide (United States) | Both | Occupation |
Experts in the medicinal marijuana and oncology arena found that medicinal marijuana can alleviate nausea, pain, seizures, and anxiety; help with coping; increase appetite and decrease risk of weight loss; minimize sleep disturbances; and manage symptoms associated with MS and neurodegenerative disorders. Recreational marijuana was perceived to be a means to “get high” for pleasure, used for medicinal or preventative purposes in certain situations, or a safer alternative to alcohol or tobacco use. Some experts expressed reservations regarding marijuana use because of lack of quality research and a necessity for stricter production standards. |
| Davison & Davison (2011) |
Overview CKD population |
N/A | Medicinal | Both |
Suggested HRQoL is negatively affected by traditional treatments in people with advanced CKD. Traditional treatments include opioids and dialysis that typically worsen the following symptoms associated with CKD: nausea, anorexia, pruritus, and insomnia. Therapeutic alternatives such as cannabinoids should be explored for the pain and symptom management of CKD. Cannabinoids have the potential to treat the aforementioned symptoms and pain experienced by people with CKD. Use of cannabinoids is limited by the psychotropic effects of THC; however, the antipsychotic effects of CBD may mitigate the psychotropic effects associated with THC. |
| Fiz et al. (2011) |
Cross-sectional study Patients with FM, N = 56 Users of cannabis, n = 28 Nonusers, n = 28 (comparison group) |
Community (Spain) | Medicinal | Both |
A statistically significant decrease of pain and stiffness, increased relaxation, and increased feelings of well-being were found in cannabis users compared with nonusers. The mental health component score of the SF–36 was slightly significantly higher in participants who used cannabis. No significant differences were found in the remaining domains of the SF–36, FIQ, and PSQI. |
| Haroutounian et al. (2016) |
Prospective open-label study N = 206 (follow-up data for 176 participants) |
Pain clinic (Jerusalem) | Medicinal | Both |
Overall, results indicated significant improvement in pain, sleep, and QoL and reduction in opioid use. Only 11 participants discontinued the treatment because of adverse events. |
| Heng et al. (2018) |
Prospective study Postoperative patients with musculoskeletal trauma, N = 500 |
Orthopedic outpatient clinic | Medicinal | Occupation |
81% of the 500 participants indicated that marijuana can be used for medicinal purposes. 78% of participants also indicated that marijuana can be used to treat pain and anxiety. 90% of the 302 participants who reported using marijuana during recovery indicated that it helped alleviate pain. 81% of that same group indicated that marijuana use helped reduce the use of opioids for pain management. |
| Johnson et al. (2013) |
Long-term, open-label, follow-up study Patients with cancer, N = 43 |
Study centers (Belgium and United Kingdom) | Medicinal | Both |
Participant scores on the BPI Short Form decreased over time, indicating an improvement in pain relief. In addition, improvements in the areas of insomnia, pain, and fatigue on the EORTC–QLQ–C30 were reported over time. |
| Khelemsky et al. (2017) |
Prospective population survey Preoperative patients, N = 501 |
Mount Sinai Hospital (New York) | Medicinal | Occupation |
81% of the 501 participants believed cannabinoids could at least be beneficial in the treatment of postoperative pain. 83% of the participants reported at least somewhat of a belief in the efficacy of cannabinoids in the treatment of chronic pain. 89% supported legalization of cannabinoids for medicinal use, whereas 60% supported legalization of cannabinoids for recreational purposes. |
| Lacey et al. (2016) |
Case-control study Drivers, N = 10,131; THC group, n = 725 Crash-involved drivers, n = 267 Non–crash-involved drivers, n = 458 |
Community (Virginia Beach) | Recreational | Occupation |
On the basis of unadjusted odds ratios, drivers who tested positive for THC were more likely to crash compared with drivers who tested negative for drugs. However, after demographic variables were considered, no statistical significance was found between groups. |
| Lal et al. (2011) |
Cross-sectional study Patients with IBD, N = 291 Patients with UC, n = 100 Patients with CD, n = 191 |
Outpatient clinic (Canada) | Medicinal | Both |
33% of lifetime users with UC and 50% of users with CD used cannabis to treat abdominal pain and diarrhea and to reduce appetite. Lifetime users who reported a low QoL and history of abdominal surgery were more likely to use cannabis to alleviate symptoms. |
| Lichtman et al. (2018) |
RCT, double-blinded, placebo-controlled study Patients with cancer, N = 291 Intervention group, n = 141 Control group, n = 150 |
International study centers | Medicinal | Occupation |
Participants receiving low and medium doses reported improvement in sleep, whereas participants in the high-dose and placebo groups had no treatment difference. Overall, the nabiximols groups reported greater analgesia than the placebo group; however, the high-dose groups reported greater adverse events. The results indicated a positive treatment effect in the low- and medium-dose groups when the two were combined. The study concluded that nabiximols are effective and safe at low to medium doses in patients with advanced cancer who respond poorly to opioids. |
| Lynch et al. (2014) |
RCT, placebo-controlled, crossover pilot study Patients with cancer, N = 16 Intervention group, n = 9 Control group, n = 7 |
Community (Canada) | Medicinal | Both |
Overall, no adverse side effects resulting from treatment were reported. In addition, no statistically significant difference in neuropathic pain HRQoL was found between the treatment and placebo groups. However, 5 of the 9 treatment participants reported a 2-point or greater reduction of pain, which is indicative of clinical significance. |
| Martellucci et al. (2015) |
Prospective study Patients with cancer, N = 18 |
Community (Italy) | Medicinal | Both |
Control of emesis was found in all participants; however, no significant control of pain was reported. Cannabinoids were found to insufficiently alleviate pain. Participants who were experiencing loss of appetite, sleep disturbances, anxiety, or depression reported clinical improvements in alleviating symptoms. QoL index scores for all participants rose. |
| McKenzie et al. (2018) |
Literature review N = 4 |
Israeli studies | Medicinal | Occupation |
Suggested cannabinoids were associated with increased QoL, decrease in pain severity, and decrease in IBD-related symptoms. Side effects associated with cannabinoid use, specifically THC, were sleepiness, drowsiness, nausea, and impaired cognitive function in 2 out of 4 studies. No significant differences in side effects were found between treatment and placebo groups. Further research that is more rigorous is required regarding the use of cannabinoids to treat people with IBD. |
| Morgan et al. (2012) |
Independent groups design study N = 120 Recreational users, n = 66 Daily users, n = 54 |
Community (United Kingdom) | Recreational | QoL |
CBD helped reduce the psychotic-like symptoms associated with THC use. In addition, the study suggested that a higher concentration of THC negatively affects psychological well-being because of increased depression and anxiety. THC was also shown to negatively affect memory, although memory was reported to be better in participants with a presence of CBD found in their hair sample. |
| Pedersen & Sandberg (2013) |
Qualitative study People with and without a medical condition N = 100 |
Community (Norway) | Recreational | Occupation |
None of the participants were approved legally for cannabis use; however, 25% reported using cannabis explicitly for medicinal purposes. Overall, participants reported using cannabis for relaxation; insomnia, stress, and pain; and symptoms associated with MS, Tourette’s syndrome, and severe rheumatism. Participants reported a preference for cannabis over prescription medication, which they identified as chemicals with the negative side effects of dependence and tolerance. |
| Portenoy et al. (2012) |
RCT, double-blinded, placebo-controlled, parallel-group study Patients with cancer, N = 263 Intervention group, n = 197 Control group, n = 66 |
International study centers | Medicinal | Both |
Overall, no significant differences were found between the treatment and placebo groups on the following measures: BPI Short Form, PGIC, MADRS, and PAC–QOL. However, EORTC–QLQ–C30 scores showed small improvements for the treatment group. In addition, the results indicated that nabiximol was more effective in lower doses, and participants in the nabiximol group reported greater analgesia than the placebo group. Participants in the high-dose nabiximol group demonstrated low tolerance and no analgesic effects. |
| Russo et al. (2016) |
Cross-sectional study Patients with MS, N = 20 Patients with pain, n = 10 Patients with no pain, n = 10 |
Research institute (Italy) | Medicinal | Both |
A significant decrease in pain was reported for the patients in the pain group as evidenced by the visual analog scale. The results of the MAS indicated a significant reduction in spasticity in addition to significant improvements in QoL as evidenced by the MSQOL for both groups. |
| Sevilla Guerra (2012) |
Mini review Patients with MS, N = 2 |
N/A | Medicinal | Occupation | Suggested cannabinoids were beneficial in treating bladder dysfunction, urge incontinence, nocturia, void urgency, and void frequency. |
| Vigil et al. (2017) |
Cohort research design study Habitual opioid users with various diagnosed diseases and illnesses, N = 66 Users of cannabis, n = 37 Nonusers, n = 29 (comparison group) |
Medicinal cannabis program (New Mexico) |
Medicinal | Both | Overall, clinically and statistically significant improvements were found in pain reduction, social life, activity levels, and QoL as well as reduction in opioid use. |
Note. BPI = Brief Pain Inventory; CBD = cannabidiol; CD = Crohn’s disease; CKD = chronic kidney disease; EORTC–QLQ–C30 = European Organization for Research and Treatment of Cancer–Quality of Life Questionnaire–Core 30; FIQ = Fibromyalgia Impact Questionnaire; FM = fibromyalgia; HRQoL = health-related quality of life; IBD = irritable bowel disease; MADRS = Montgomery–Åsberg Depression Rating Scale; MAS = Modified Ashworth Scale; MS = multiple sclerosis; MSQOL = Multiple Sclerosis Quality of Life assessment; N/A = not applicable; PAC–QOL = Patient Assessment of Constipation Quality of Life; PGIC = Patient Global Impression of Change; PSQI = Pittsburgh Sleep Quality Inventory; QoL = quality of life; RCT = randomized controlled trial; REM = rapid eye movement; SF–36 = 36-item Short Form Health Survey; THC = δ-9 tetrahydrocannabinol;; UC = ulcerative colitis.
*
Indicates studies included in the scoping review.