
Abstract
Nearly 16.5 million children and youth meet Diagnostic and Statistical Manual of Mental Disorders (5th ed.; American Psychiatric Association, 2013) criteria for a mental health condition (National Alliance on Mental Illness, 2019), and many more are at risk for developing mental health conditions over their lifetime (Polanczyk et al., 2015). Children with poor mental health often experience negative outcomes related to academic success and occupational performance (Maurizi et al., 2013; Watling & Nielsen, 2010). Occupational therapy practitioners understand that a lack of meaningful participation in occupations signals poor mental health or mental illness and that active engagement is associated with positive mental health. Activity- and occupation-based interventions are increasingly recognized as supportive of mental health in children and youth (Bazyk & Bazyk, 2009; Petrenchik & King, 2011; Shea & Jackson, 2015; Tokolahi et al., 2016).
In this review, we sought to identify evidence for activity- and occupation-based interventions within the scope of occupational therapy practice for children and youth with and at risk for mental health concerns. Occupation-based interventions are defined as interventions in which engagement in a recognizable occupational form (e.g., yoga, karate) is the main ingredient (Fisher, 2014, p. 98) or primary focus. Activity-based interventions are defined as interventions in which an occupational form (e.g., journaling, playing a game) is embedded but is not the fundamental component. The review question was developed in collaboration with American Occupational Therapy Association (AOTA) staff and reviewed by an expert panel. This review was supported by the AOTA Evidence-Based Practice (EBP) Project.
Method
We used the methodology recommended in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines (Moher et al., 2009). This review builds on a previous review by Arbesman and colleagues (2013), which included articles published from 2003 through 2012. Key search terms were developed by the EBP Project methodology consultant and reviewed by an expert panel that included the first author (Cahill). A medical research librarian with prior systematic review experience conducted searches in MEDLINE, PsycINFO, CINAHL, ERIC, OTseeker, and the Cochrane databases for peer-reviewed research studies published in scientific journals.
After the methodology consultant completed a first review of the search results, the first two authors (Cahill and Egan) independently reviewed the titles for inclusion on the basis of specified criteria, discussing any discrepancies until they reached agreement. The review was limited to articles published in English in peer-reviewed scientific journals between January 2010 and March 2017 that described activity- or occupation-based interventions. Conference proceedings, non–peer reviewed publications, dissertations, theses, and presentations were excluded from this review. Moreover, studies that involved participants younger or older than ages 5–21 were excluded.
Full-text articles were evaluated for inclusion independently by all three authors. Included articles were summarized in an evidence table that included brief descriptions of the interventions, outcomes, and results (Table A.1 in Appendix A). A risk-of-bias analysis was completed for each article to determine whether the study presented a low, moderate, or high risk of selection, performance, detection, attrition, and reporting bias (Table A.2). The evidence table and risk-of-bias analyses were reviewed by EBP Project staff.
Evidence levels for the articles were determined on the basis of the ranking system by Sackett (1989), as follows:
Level I—Systematic reviews, meta-analyses, randomized controlled trials (RCTs)
Level II—Two groups, nonrandomized studies (e.g., cohort, case control)
Level III—One group, nonrandomized studies (e.g., before and after, pretest–posttest)
Level IV—Descriptive studies that include analysis of outcomes (e.g., single-subject design, case series)
Level V—Case reports and expert opinion that include narrative literature reviews and consensus statements.
Only articles rated Level I, II, or III were included in this review.
Ratings related to the strength of evidence were based on the guidelines of the U.S. Preventive Services Task Force (2018), as follows:
Strong evidence—Consistent results from rigorous studies, usually at least two RCTs
Moderate-strength evidence—1 RCT, 2 or more studies with lower levels of evidence, or some inconsistency in findings across otherwise rigorous studies
Low-strength evidence—Few studies, a group of studies that do not include an RCT, or studies with methodological flaws.
Results
The initial search yielded 89,461 results (Figure 1). In the first review, the EBP Project methodology consultant removed all articles not relevant to the research question and exported 5,310 citations to the authors for review. The initial review of the titles by the first two authors resulted in the exclusion of 4,913 articles and the removal of 40 duplicate articles. The authors reviewed abstracts and full text of the remaining 357 articles using the inclusion and exclusion criteria. A total of 62 articles describing 20 (32%) Level I studies, 22 (36%) Level II studies, and 20 (32%) Level III studies were included in the review.
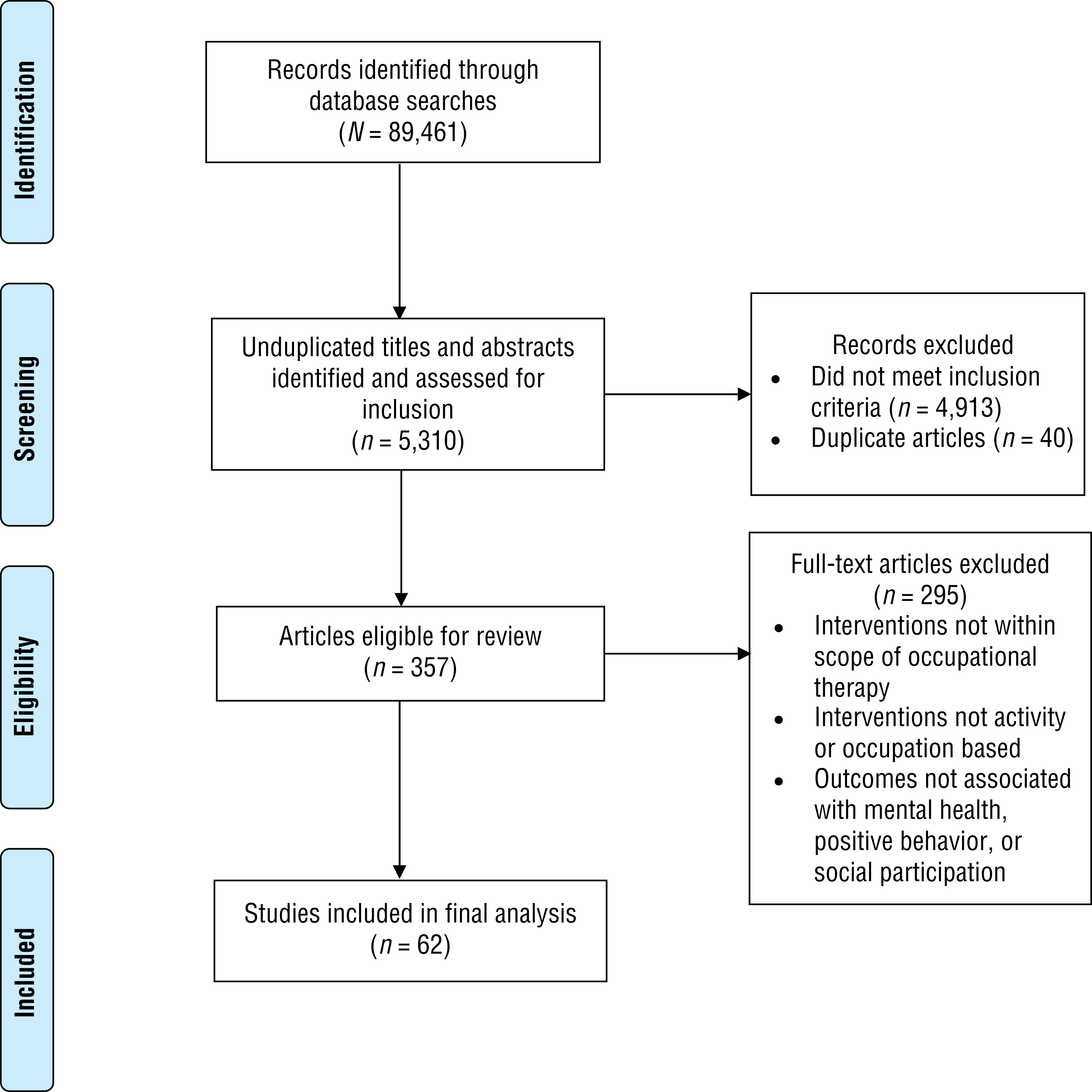
Flow diagram for reviewed studies.
We grouped the articles on the basis of type of intervention and found nine categories related to activity- and occupation-based interventions: (1) outdoor groups and camps, (2) video and computer games, (3) productive occupations and life skills, (4) meditation, (5) animal-assisted interventions, (6) creative arts, (7) play, (8) sports, and (9) yoga. Table 1 summarizes the strength of evidence for each intervention on the basis of the three outcomes of interest: mental health, positive behavior, and social participation. Studies in six of the nine intervention categories addressed only two of these outcomes; studies in the other three intervention categories—productive occupations and life skills, sports, and yoga—yielded evidence for all three outcomes. In this article, we focus on only these three categories because of space limitations.
Summary of the Strength of Evidence for Each Intervention Type and Outcome Category
Note. — = outcome not addressed.
Mental Health
Moderate-strength evidence from 8 studies supports yoga to improve mental health (Beets & Mitchell, 2010, Level I; Carei et al., 2010, Level I; Hall et al., 2016, Level III; Khalsa et al., 2012, Level I; Khalsa et al., 2013, Level II; Richter et al., 2016, Level II; Thygeson et al., 2010, Level III; Velásquez et al., 2015, Level I). Significant improvements were found in all of the studies except an RCT by Carei et al. (2010). Intervention content varied across studies, but all provided yoga in a group format. Some studies used a specific yoga program; for example, an RCT by Khalsa et al. (2012) used Yoga Ed, which emphasizes mindfulness in addition to yoga postures and games, breathing exercises, and visualization.
Moderate-strength evidence from 3 studies supports productive occupations and life skills training to address psychosocial and mental health outcomes (Kaboski et al., 2015, Level II; Pfiffner et al., 2014, Level I; Tokolahi et al., 2013, Level III). Interventions included life skills modules (e.g., organization, self-care, daily living skills; Pfiffner et al., 2014), vocational skills groups (Kaboski et al., 2015), and graded occupational engagement (Tokolahi et al., 2013). Kaboski et al. (2015) focused on outcomes associated with a vocational skills group for adolescent boys with autism spectrum disorder (ASD) and found significant decreases in social anxiety compared with typically developing peers. Tokolahi et al. (2013) examined an occupation-based group informed by cognitive–behavioral principles for children with anxiety and found significant changes in parent ratings of anxiety symptoms and internalizing behaviors.
Low-strength evidence from 3 Level II studies with mixed results addressed the use of sports interventions, including martial arts (Haydicky et al., 2012), boxing (Terry et al., 2014), and basketball (D’Andrea et al., 2013), to improve mental health outcomes. Two of the studies found nonsignificant results, but D’Andrea et al. (2013) found that a trauma-informed basketball program for adolescent girls with severe behavioral issues resulted in significantly reduced internalizing and externalizing behaviors.
Positive Behavior
Moderate-strength evidence from 2 studies was found for using yoga to improve behavior (Koenig et al., 2012, Level II; Telles et al., 2013, Level I). Both studies found significant improvements, but in the RCT by Telles et al. (2013), yoga was no more effective than group physical exercise.
Moderate-strength evidence from 3 studies supports the use of sports interventions to increase positive behaviors (D’Andrea et al., 2013, Level II; Kang et al., 2011, Level I; Pan, 2010, Level II). Kang et al. (2011) found significant reductions in inattention for children with attention deficit hyperactivity disorder who participated in 3 hr of weekly athletic activities. Pan (2010) investigated a water exercise swimming program and found significant decreases in antisocial behaviors. D’Andrea et al. (2013) found that adolescent girls who participated in a basketball intervention demonstrated increased perseverance, on-task, and conflict resolution behaviors, but these changes did not reach statistical significance.
Low-strength evidence from 1 Level I study was found for using productive occupations and life skills training to address positive behavioral outcomes (Pfiffner et al., 2014). Pfiffner et al. (2014) explored the impact of Child Life and Attention Skills (CLAS) groups on positive behaviors, particularly organizational behaviors that support performance at home and school. A significant increase in parent-reported organizational skills was found, but teacher reports at 1 yr follow-up indicated that these improvements were not maintained.
Social Participation
Strong evidence from 3 studies was found for sports interventions to support social participation (Bahrami et al., 2016, Level I; Haydicky et al., 2012, Level II; Kang et al., 2011, Level I). An RCT by Bahrami et al. (2016) examined the impact of a 14-wk karate intervention for boys with ASD and found significant reductions in social skill deficits and communication deficits at postintervention and follow-up. In another RCT, Kang et al. (2011) found significant improvements in cooperativeness after a 6-wk sports intervention. Haydicky et al. (2012) found improvements, though not significant, in parent-reported social problems for adolescent boys who participated in a manualized mindfulness martial arts intervention.
Low-strength evidence from 4 studies was found for yoga to improve social participation in children and youth. Improvements were significant in 2 of the studies (Beltran et al., 2016, Level III; Telles et al., 2013, Level I) and not significant in 2 studies (Koenig et al., 2012, Level II; Velásquez et al., 2015, Level I).
Low-strength evidence from 2 studies was found for the use of productive occupations and life skills interventions to improve social participation. Block et al. (2012, Level II) found that a manualized garden-to-table life skills group had a significant impact on cooperative behaviors. Pfiffner et al. (2014, Level I) examined the impact of CLAS groups on social participation and found significant parent-reported improvements in social skills; however, no significant improvements in teacher-reported outcomes were found.
Discussion
The studies included in this review provide evidence for activity- and occupation-based interventions to promote mental health, positive behavior, and social participation of children and youth with and at risk for mental health concerns and support previous studies highlighting the connection between engagement in occupation and positive mental health outcomes for children and youth (Tokolahi et al., 2016). The interventions included in this review are not unique to the practice of occupational therapy, but occupational therapy practitioners can use these interventions with children and youth and help them incorporate the activities and occupations into their daily and weekly performance patterns.
Evidence supports the use of productive occupations and life skills, sports, and yoga interventions to address all three outcomes of interest—mental health, positive behavior, and social participation. Yoga was the only intervention type that addressed all three outcomes with moderate strength of evidence; the evidence supporting yoga and sports interventions is stronger than that for productive and life skills interventions. These findings suggest that engagement in physical activities, particularly those that enhance the mind–body connection, enhances mental health and that such interventions should be introduced in childhood, when people are learning behavioral and emotional regulation skills (Hall et al., 2016).
Implications for Occupational Therapy Practice and Research
This systematic review has the following implications for occupational therapy practice and research:
Moderate-strength evidence suggests that yoga can be used to address mental health, positive behavior, and social participation of children and youth.
Low- to moderate-strength evidence suggests that productive occupations and life skills training can be used to address mental health, positive behavior, and social participation.
Limitations
This systematic review focused on three distinct outcomes, a broad focus that resulted in the inclusion of many studies that addressed only one or two outcomes. Future systematic reviews should focus on single, discrete outcomes, which would allow occupational therapy practitioners to more easily translate findings into practice.
Many studies were excluded from this review because they lacked sufficient intervention descriptions, making it difficult to determine whether the interventions could be classified as activity or occupation based. Additionally, many studies used self-report and subjective measures of mental health, positive behavior, and social participation; the use of more objective measures may increase rigor and strengthen study outcomes.
Many included studies reported outcomes immediately after the intervention or after a relatively short follow-up period, which prevents an understanding of the longer-term impacts on these outcomes. In addition, although all the interventions in this review are within the scope of occupational therapy practice, most of the studies were conducted by professionals in other disciplines. More research is needed to better understand this gap and to strengthen the evidence supporting the use and effectiveness of these interventions in occupational therapy practice.
Conclusion
Nine categories of activity- and occupation-based interventions were identified in this review. However, only three types of interventions—productive occupations and life skills, sports, and yoga—addressed mental health, positive behavior, and social participation. Occupational therapy practitioners should match the desired outcome to the most effective intervention type when incorporating activity- and occupation-based interventions into occupational therapy services for children and youth with and at risk for mental health concerns.
Footnotes
Acknowledgments
We thank Deborah Lieberman and Beth Hunter for their guidance and support; we also thank Ashley Buksa and Kierra Peak (MSOT students) for retrieving full-text articles and organizing data.
Appendix
*
Indicates studies that were systematically reviewed for this article.