
Abstract
Cerebral palsy (CP), defined as nonprogressive motor impairment occurring in the developing brain, is the most common pediatric physical disability, with an incidence of 2–2.5 per 1,000 live births (Rosenbaum et al., 2007; Stanley et al., 2000). Children with hemiplegic CP, who present with hemiparesis or a substantially greater deficit on one side of the body, make up a large proportion of this population (Odding et al., 2006). Children with hemiplegic CP tend to use their less affected side more than their more affected side, especially the upper extremity. The neglect-like phenomenon of the affected upper limb, despite some preserved skills, in children with hemiplegic CP is referred to as developmental disregard (DD; Houwink et al., 2011, 2013; Taub et al., 2006). Insufficient use of the affected upper limb has a negative effect on motor improvement and skill development and subsequently brings about functional deficits that further interfere with development in multiple life domains, including play, self-care, and daily activities (Sakzewski et al., 2010).
Although different hypotheses have been proposed to explain the phenomenon of DD, there is currently no consensus in the field of CP research. Understanding the underlying mechanism of DD has high clinical value in that it dictates the direction of therapeutic approach. Some authors have viewed DD as a process in which a child gradually learns not to use the more affected limb as a result of negative reinforcement from unsuccessful experiences with that limb (Crocker et al., 1997; Hoare et al., 2007; Taub et al., 1999, 2004; Zielinski, Jongsma, et al., 2014). Others have posited that DD is a neurologically based phenomenon, similar to poststroke neglect syndrome, that is caused by brain injury to the neural networks involved in spatial attention processes (Sutcliffe et al., 2009; Zielinski, Steenbergen, et al., 2014). Clinical characteristics of typical people with stroke support that lesions in these networks cause deficits of both spatial attention and motor performance on the more affected side (Sutcliffe et al., 2009; Zielinski, Steenbergen, et al., 2014). However, despite the strong similarity between neglect syndrome in people with stroke and DD in children with hemiplegic CP (Sutcliffe et al., 2009), the neural mechanisms underlying the correlation between motor performance and spatial attention in children with DD are not clear. Specifically, one cannot ignore developmental factors and the influence of motor learning.
Neurodevelopmental researchers have argued that as a result of the lack of use of the more affected upper limb during the developmental period, neural substrates serving entire classes of motor behaviors may not be established, refined, or coordinated (Zielinski, Jongsma, et al., 2014). This delay in neural refinement is believed to affect not only the actual motor performance of children with hemiplegic CP but, most likely, also the higher order cognitive aspects involved in motor behavior (Houwink et al., 2011; Hugdahl & Carlsson, 1994; Rizzolatti & Camarda, 1987; Zielinski, Jongsma, et al., 2014; Zielinski, Steenbergen, et al., 2014). Although some evidence demonstrates performance asymmetry in auditory attention (Hugdahl & Carlsson, 1994), the current literature is largely limited in studies addressing the neurocognitive profile of children with CP that include spatial attention. In particular, whether the observed disregard in motor domains can also be extended to the spatial attention domain remains undetermined.
In this study, we aimed to investigate asymmetrical performance in the motor and visual–spatial attention domains of children with hemiplegic CP. Moreover, we investigated whether asymmetrical performance in both visual–spatial attention and motor domains, if any, was associated with use of the more affected hand in daily activities. We hypothesized that (1) children with hemiplegic CP would demonstrate performance asymmetry not only in motor performance but also in tasks related to visual–spatial attention and that (2) this performance asymmetry would be associated with the frequency of use of the more affected hand during daily activities.
Method
Participants
A convenience sample of 25 children with hemiplegic CP (ages 5–12 yr) was recruited from local community agencies, schools, and hospitals. Children were excluded if they were unable to understand instructions or complete the required task. Twenty-five age-matched typically developing (TD) children participated to serve as a reference group. All participants had normal or corrected-to-normal vision. We obtained informed consent from the children’s guardians and assent from the participating children before data collection. This study was approved by the review board of National Taiwan University Hospital (No. 201605102RIN).
Instruments
We used three measures. The computerized Random Visual Stimuli Detection Task (RVSDT), developed by our research team, was used to assess visual–spatial attention. The Melbourne Assessment 2 (MA2; Randall et al., 2014) was used to assess the quality of motor performance in each hand. Finally, the Observatory Test of Capacity, Performance, and Developmental Disregard (OTCPDD; Liu et al., 2016) was used to assess use of the hand of the more affected upper limb in daily activities. Children with hemiplegic CP were evaluated with all three measures (RVSDT, MA2, and OTCPDD); TD children were evaluated with only the RVSDT.
Random Visual Stimuli Detection Task
The RVSDT is a computer-based paradigm that aims to probe the distribution of spatial attention across the visual field. It was programmed using the MATLAB-based Psychtoolbox (Pelli, 1997). A typical RVSDT trial begins with a red fixation cross in the center of the computer screen that aims to reset the participant’s spatial attention to the screen center and prepares the participant for the trial.
Trials were presented under two conditions: a target-present condition and a target-absent condition. In the target-present condition, after a variable delay (1,000–2,500 ms) from the trial onset, a white dot (size = 0.5°) was presented for 50 ms at a random location within a circular area that extended 22° of visual angle (Figure 1). Children were asked to press a designated button with their dominant hand (unaffected hand for children with CP) as soon as they saw the white dot appear on the screen. A “miss” response was recorded for trials in the target-present condition if the child did not press the button or the corresponding reaction time (RT) was longer than 2.5 s. The target of a given trial could randomly appear in 1 of 12 subregions (4 subregions in the central visual field and 8 subregions in the peripheral visual field, as shown in Figure 1). In the target-absent condition, no target was presented on the screen, and therefore no motor response was required. The target-absent condition was included to prevent blind motor responses by participants. A false alarm was recorded if a response was made for a trial in the target-absent condition.
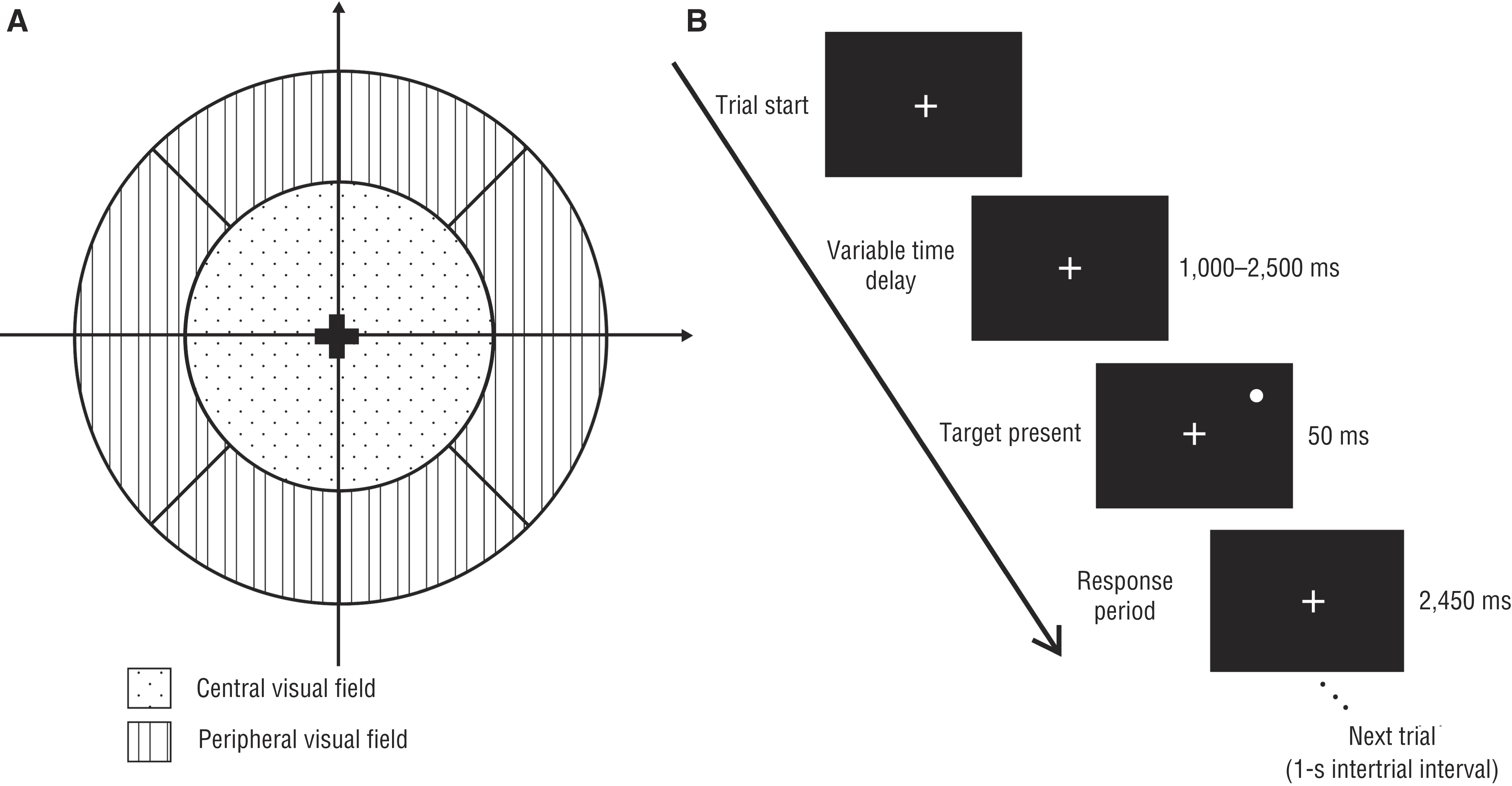
Random Visual Stimuli Detection Task: (A) the 12 subregions in which the target could be presented across a visual field that extended 22° of visual angle and (B) the typical display sequence for a trial of the target-present condition.
All potential participants performed a practice session to assess whether they were able to understand the instructions and visually detect the stimulus over the full range of the screen (especially when testing the visual field). Only participants who passed the practice session continued to complete the RVSDT. The complete RVSDT consisted of 180 trials divided into three sessions. Each session consisted of 60 trials, with 48 target-present trials (4 trials for each subregion) and 12 target-absent trials. The randomization of condition order and varied trial onset time prevented prediction of an upcoming trial.
To perform the RVSDT, children were instructed to sit at a table with their head positioned on a chinrest. The eye-to-screen distance was approximately 60 cm. Children could take short breaks between sessions.
Melbourne Assessment 2
The MA2 is a valid and reliable tool designed to evaluate the quality of unilateral upper limb motor performance in children with CP ages 2.5–15 yr (Randall et al., 2014). The MA2 measures four elements of upper limb movement quality: (1) active movement range for each upper limb joint; (2) accuracy of reach for, or in place of, a task; (3) dexterity of finger movements when grasping, releasing, and manipulating objects; and (4) fluency or smoothness of movements. Each child was asked to complete 14 test items. Each test was video recorded for subsequent scoring. Items were scored for each element of movement measured and categorized into four corresponding subscales.
Observatory Test of Capacity, Performance, and Developmental Disregard
The OTCPDD is an observation-based assessment designed to evaluate a child’s general hand function for the more affected upper limb in bimanual daily living activities (Liu et al., 2016). Ten functional motor components (reach, grasp, hold and carry, release, stabilize, adjust, catch and throw, manipulate, press, and pinch) were observed and scored while children performed 18 bimanual tasks. During the assessment, the child was asked first to perform each task spontaneously without instruction (to simulate real-world performance), and then the child was encouraged to use both hands (forced-use capacity). The frequency of more affected hand use for each motor component was counted and summed to obtain the final score for each condition (i.e., real-world performance and forced-use capacity). The difference in score between the two conditions (i.e., the DD score) was defined as the level of severity of DD. The OTCPDD demonstrated excellent reliability (intrarater and interrater) and good validity (Liu et al., 2016).
Statistical Analysis
On the basis of previous findings (Zielinski, Jongsma, et al., 2014), we estimated the sample size requirement to be 21 children for each group in a two-group study design, given a large effect size (d = 0.80), a power of .80, and a one-sided Type 1 error of .05. Therefore, we planned to recruit at least 25 children to each group.
Performance asymmetry in both visual–spatial attention and motor performance was quantified by the Asymmetry Index (AI). We used the AI to estimate the performance discrepancy between dominant and nondominant sides for the TD group and between more affected and less affected sides for the group with CP. We calculated two attention AIs using the median RT (Equation 1) and the average miss rate (MR; Equation 2) for each subregion in the target-present condition in the RVSDT and four motor AIs using the four subscales of the MA2: Range of Motion, Accuracy, Dexterity, and Fluency (Equation 3)



The magnitudes of AIs ranged from 0 to 1. A positive value represents poorer performance on the nondominant side than on the dominant side, and a zero value represents comparable performance between the dominant or less affected and nondominant or more affected side.
We used IBM SPSS Statistics (Version 22.0; IBM Corporation, Armonk, NY) for all data analyses. Independent t tests and χ2 tests were used for group comparison of demographic data, RTs, MRs, and all AIs generated from the RVSDT and MA2 scores. To explore the relationship between motor and visual–spatial attention performance asymmetry, we further calculated the correlation between the severity of DD (DD scores) and more affected hand function (MA2 scores) and the RVSDT.
Results
The demographic characteristics of the study participants are shown in Table 1. We found no statistically significant differences in age and gender between the two groups. Significant differences were found for hand dominance. A majority of TD children were right-hand dominant, but the number of children with CP with right- and left-dominant hands was comparable.
Demographic Characteristics and Visual–Spatial Attention Performance Results Among Children With CP and TD and MA2 and OTCPDD Results Among Children With CP
Note. AI motor = Asymmetry Index in the motor domain; CP = cerebral palsy; M = mean; MA2 = Melbourne Assessment 2; OTCPDD = Observatory Test of Capacity, Performance, and Developmental Disregard; ROM = range of motion; RVSDT = Random Visual Stimuli Detection Task; SD = standard deviation; TD = typical development.
p < .05. ** p < .01.
Visual–Spatial Attention
Visual–spatial attention was measured by the RVSDT, and the corresponding results are summarized in Table 1. Significant differences between the two groups were found for RT and MR in the dominant, nondominant, central, and peripheral visual fields (p < .01). Children with hemiplegic CP demonstrated overall slower RT and higher MR when performing spatial attention tasks across the whole visual field.
Further comparison was conducted using the AIs for RT (AI attRT ) and MR (AI attMR ; Table 2). The results showed no significant group differences for AI attRT for both the central and peripheral visual fields, but significant group differences for AI attMR were found in the overall (p = .02) and peripheral (p = .01) visual fields.
AI for the Attention Domain Based on RVSDT Between Children With CP and TD Children
Note. AI attMR = attention Asymmetry Index for miss rate; AI attRT = attention Asymmetry Index for reaction time; CP = cerebral palsy; M = mean; RVSDT = Random Visual Stimuli Detection Task; SD = standard deviation; TD = typically developing.
p < .05.
Upper Limb Movement Quality
The MA2 was used to assess the unilateral upper limb movement quality of children with hemiplegic CP. The mean scores for the more affected hand and maximum scores were 20.8/27, 21.5/25, 10.3/16 and 14.5/21 for the Range of Motion, Accuracy, Dexterity, and Fluency subscales, respectively.
We also conducted further analysis of AIs for the four subscales. The motor AI (AI motor) for children with hemiplegic CP on the Range of Motion, Accuracy, Dexterity, and Fluency subscales were 0.23, 0.14, 0.45, and 0.30, respectively, indicating a discrepancy in movement quality between hands ranging from 14% to 45%. The largest motor discrepancy was on the Dexterity subscale (0.45) and the smallest was on the Accuracy subscale (0.14; Table 1). That is, the quality of motor performance on the more affected side was 14%–45% poorer than that on the unaffected side.
Affected Hand Use in Daily Activities
The OTCPDD was used to assess the use of the more affected hand in daily activities. The OTCPDD DD score represents the extent of underuse of the more affected hand. The DD score was 8.25, indicating that children with hemiplegic CP performed on average 8.25 more motor units in a forced-use context than in the spontaneous-use context (Table 1).
Interrelationship Between Motor and Visual–Spatial Attention Performance
We explored the interrelationship of affected-hand use in daily activities, motor capacity, and performance of visual–spatial attention in children with CP using DD scores, AIs for the four MA2 subscales (AI ROM, AI Accuracy, AI Dexterity, AI Fluency), RT (AI attRT ), and MR (AI attMR ; Table 3). Our results demonstrated that a significant correlation exists between DD score and discrepancy in motor quality for all four subscales of the MA2 (rs = .71–.80, p < .01). That is, the severity of DD was significantly associated with performance asymmetry in motor quality. We also found a significant correlation between DD scores and AI attMR (visual–spatial attention performance) in both overall and peripheral visual fields (rs = .50 and .53, respectively). In other words, the severity of DD is significantly associated with performance asymmetry in visual–spatial attention.
Correlations Between DD Scores and Level of Performance Asymmetry in Motor and Visual–Spatial Attention Domains in Children With Hemiplegic CP
Note. AI = Asymmetry Index; AI attMR = miss rate Asymmetry Index in the attention domain; AI attRT = reaction time Asymmetry Index in the attention domain; CP = cerebral palsy; DD = developmental disregard; OTCPDD = Observatory Test of Capacity, Performance, and Developmental Disregard; ROM = range of motion.
p < .05. **p < .01.
Discussion
The findings of this study support both of our hypotheses. First, our results showed that children with hemiplegic CP demonstrated performance asymmetry not only in motor performance but also in visual–spatial attention–related tasks. In terms of visual–spatial attention performance, we found that children with hemiplegic CP demonstrated performance asymmetry in MR only, not in RT. This finding implies that children with hemiplegic CP may have weaker attentional readiness or vigilance in the visual field of the more affected side. Anderson et al. (2000) had similar findings for adults with spatial neglect: They reported that patients with spatial neglect responded with comparable RT for successful trials in both neglected and nonneglected space, whereas their success rates were lower when stimuli were presented only in neglected space.
To our knowledge, this is the first study investigating the characteristics of visual–spatial attention in children with hemiplegic CP. We found that children with hemiplegic CP showed generally less optimal performance on visual–spatial attention tasks compared with TD children, as evidenced by slower RT and higher MR. These results further support that children with hemiplegic CP may also have cognitive dysfunction. Spatial attention is considered a fundamental cognitive functionality for developing and facilitating performance in other functional domains, including motor function. The overall poor performance of children with hemiplegic CP in spatial attention tasks across the whole visual field indicates that their dysfunction in the cognitive domain may not be limited to higher order cognition, as previously reported (e.g., executive function; Zielinski, Steenbergen, et al., 2014). These findings highlight the importance of including cognitive profiles in routine evaluations of children with CP. Moreover, the findings also prompt a reexamination of the need for cognitive intervention with children with hemiplegic CP.
The results support our second hypothesis that underuse of more affected limbs in daily activities (DD scores in the OTCPDD) not only correlates with asymmetric performance in the motor domain (Houwink et al., 2013; Liu et al., 2016; Taub et al., 2006) but is also associated with performance asymmetry in the attention domain. Our findings support the description of development-related disregard phenomena. As a result of asymmetrical development between the more affected and less affected limbs, the neural development of various functions, including cognitive domains, is not well established. Therefore, development-based disregard phenomena are likely to be observed in multiple functional domains (Houwink et al., 2011; Sutcliffe et al., 2009; Zielinski, Jongsma, et al., 2014).
In addition, a positive correlation between DD and spatial attention disregard is in line with premotor theory (Punt & Riddoch, 2006; Rizzolatti & Camarda, 1987), which claims that attention and motor circuits are closely linked. This theory posits that people normally shift their attention purposefully to prepare for future actions in an attended space. The underuse of the more affected limb might dim the neural networks subserving space representations and thus influence the perception of stimuli in the ipsilesional hemispace. However, it is important to note that the current results are not sufficient to identify the potential causal links between outcome measures. Future studies are needed to further disentangle the relationship between DD and the spatial attention and motor domains.
The results of asymmetric performance in motor domains were expected. Children with hemiplegic CP demonstrated poorer motor quality in the more affected hand than in the less affected hand, which aligns with findings of other studies (Houwink et al., 2013; Taub et al., 2006). We used a motor AI to represent the discrepancy in motor quality between both hands in range of motion, accuracy, dexterity, and fluency. We expected to observe greater motor discrepancy in dexterity, because it is a higher level motor skill (Randall et al., 2014). Moreover, the magnitude of a child’s motor AI might provide clinical meaning and guide treatment priorities. For example, the motor AI for the Dexterity subscale was 0.45. One could interpret this to mean that the motor quality of the more affected hand among children with hemiplegic CP was only half that of the less affected hand. This finding highlights the need to target dexterity in the more affected hand during bimanual activities.
Two limitations of this study warrant consideration. First, our results are based on a convenience sample and may have limited generalizability. Second, although the results reveal that children with hemiplegic CP have spatial attention disregard in the visual domain, whether such attention disregard extends to other sensory modalities, such as the auditory or tactile system, is still unclear and could also result in functional limitations in daily activities. Future studies with a design that allows testing of attentional performance in a multisensory context will be needed to answer this question.
Implications for Occupational Therapy Practice
The results of this study demonstrate that children with hemiplegic CP exhibit spatial attention disregard and that this phenomenon is correlated with motor quality and underuse of the more affected hand. Therefore, we strongly recommend that the evaluation of and intervention for visual–spatial attention be included in the traditionally motor-oriented rehabilitation approach.
Conclusion
The motor performance of children with CP has always been a predominant focus of researchers and clinicians. Our results provide behavioral evidence to support the growing clinical belief that cognitive aspects play an important role in the daily performance of children with hemiplegic CP. Specifically, children with hemiplegic CP demonstrated DD in both the motor and the visual–spatial attention domains. Spatial attention disregard also significantly correlated with use of the hand on the more affected side in daily activities. The evaluation of visual–spatial attention in children with hemiplegic CP is necessary to establish a comprehensive developmental profile as well as to design effective intervention protocols. We suggest including cognitive profiles in routine evaluations and adding spatial attention interventions to traditionally motor-oriented treatment.
Footnotes
Acknowledgments
This project was supported in part by Ministry of Science and Technology grants to Tien-Ni Wang (MOST 103-2314-B-002-008-MY3, MOST 107-2314-B-002-049-MY3) and Chien-Te Wu (MOST 102-2923-H-002-002-MY3, MOST 104-2314-B-002-094).