
Abstract
Activities of daily living (ADLs) include feeding, dressing, toileting, and personal hygiene. Occupational therapy practitioners work with young children and their families to promote participation in meaningful occupations and ADLs and to establish daily habits and routines for their children for sleep and rest (American Occupational Therapy Association [AOTA], 2014). Interventions for ADLs and sleep routines occur in the context of early intervention (EI) coaching, the neonatal intensive care unit (NICU), educational preschool programs, inpatient hospital programs, and pediatric outpatient clinics. Sleep, eating, and toileting habits are often the primary areas of concern for families of young children with and without diagnosed disabilities, developmental delay, or challenges with behavioral regulation. Occupational therapy practitioners provide the team with a holistic outlook and can address motor, sensory, cognitive, and behavioral factors necessary for appropriate development and directly associated with participation in ADLs and rest and sleep. It is essential that occupational therapy practitioners incorporate current knowledge of effective interventions to improve ADLs and rest and sleep performance in young children.
This systematic review aims to provide up-to-date and expanded knowledge about evidence-based interventions for outcomes related to ADLs, rest, and sleep to be included in published occupational therapy practice guidelines related to early childhood practice. This review addresses the following question: What is the evidence for the effectiveness of interventions within the scope of occupational therapy practice to support ADLs, rest, and sleep for children ages 0–5 yr and their families?
Method
This systematic review followed Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for systematic reviews (Moher et al., 2009). Search terms (Table 1) were established by the review authors, medical librarian, research methodologist, and AOTA staff. These terms were reviewed by an advisory group before the search was conducted. An overall literature search was performed by the medical librarian. The search strategy included five databases (MEDLINE, PsycINFO, CINAHL, OTseeker, ERIC) and Evidence-Based Medicine Reviews, Cochrane Database of Systematic Reviews, Cochrane Controlled Trials Register, and Database of Abstracts of Reviews of Effectiveness. After the initial review, it was determined that the search did not return evidence related to toileting, dressing, or grooming ADLs for this age group. A secondary search with additional search terms was conducted, which then captured toileting but no dressing or grooming studies.
Search Terms for Systematic Review of Children and Youth
Note. DIR = Developmental, Individual differences, Relationship model; NIDCAP = Newborn Individualized Developmental Care and Assessment Program.
The systematic review included studies that were published in peer-reviewed journals in English between January 2010 and March 2017 (ADLs and feeding) or between January 2000 and March 2017 (sleep and toileting). Only Level I, II, and III studies were included, unless the evidence at these levels was not sufficient. For toileting, a topic for which there were not sufficient high-level studies available, Level IV studies were also included. Studies included in the review were required to be within the scope of occupational therapy practice (AOTA, 2014) and focused on children ages 0–5 yr.
Additional inclusion criteria required studies to use specific outcome measures relating to ADL performance or sleep. Studies were excluded if they were dissertations, theses, presentations, or proceedings; if they were published before the publication date range; and if outcomes were focused on children older than age 5 yr, 11 mo. Additional exclusion occurred when studies focused on interventions that are outside the scope of occupational therapy practice and when the age range of children in the studies reviewed in systematic and other review articles were not clearly delineated. The protocol for this review is not published separately; the process is presented in the Method section.
The initial results were reviewed by the AOTA Evidence-Based Practice Project research methodologist to eliminate articles not relevant to the project. The citations were then provided to the review authors for further appraisal. Data were collected on levels of evidence (design), quality (scientific rigor), and significance of findings. After duplicate titles were removed by a graduate student assistant, titles and abstracts were screened. Each study was given a rating of yes, no, or maybe. The “maybe”-rated articles were reviewed by the research team in a conference call to determine inclusion. An evidence table was developed and reviewed by the research methodologist (Table A.1 in the Appendix).
In addition, studies were analyzed for risk of bias using the Cochrane Collaboration’s tool (Table A.2; Higgins et al., 2011). Risk of bias was considered when determining overall strength of evidence for the generated themes as strong, moderate, or low. A rating of strong was applied if the outcome had 2 or more Level I studies and the available evidence usually included consistent results from well-designed, well-conducted studies. A rating of moderate was assigned if at least 1 Level I high-quality study or multiple moderate-quality studies were available and the available evidence was sufficient to determine the effects on health outcomes, but confidence in the estimate was constrained by size or quality of individual studies or inconsistency was found across individual studies. A rating of low was assigned if a small number of low-level studies were available or if studies had significant flaws, and the available evidence was determined to be insufficient to assess effects on health and other outcomes of relevance to occupational therapy (U.S. Preventive Services Task Force, 2018). No overall assessment of risk of bias was identified that affected the cumulative analysis.
Results
From the initial search, 5,310 results were returned; 17 articles were added by secondary search for additional toileting search terms not included in the original search process. The study team reviewed 109 full-text articles and summarized them in a master citation table. Figure 1 shows the flow diagram for inclusion and exclusion of studies. A total of 40 articles were included in the final evidence table (see Table A.1).
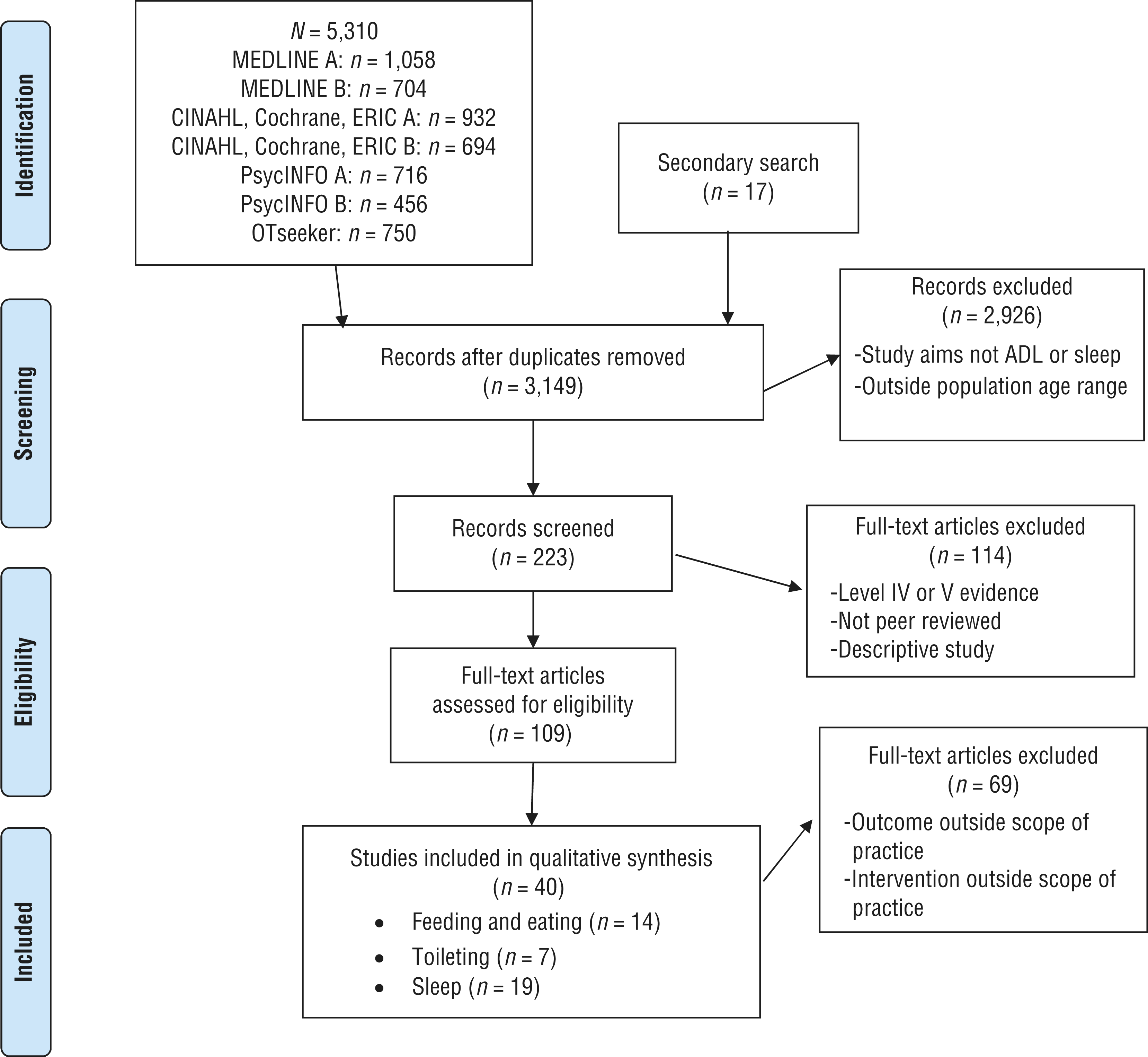
Flow diagram for inclusion and exclusion of peer-reviewed studies in the systematic review.
We evaluated the final 40 articles for risk of bias and intervention themes. Overall, the risk of bias for studies included in this review was acceptable, with weaknesses noted in blinding personnel and outcome assessments, which is likely a result of the types of outcome measures used (see Table A.2). After analysis of all the studies included in the review, we identified three main themes: interventions to address sleep and rest, interventions to address feeding and eating, and interventions to address toileting. Within each theme, articles were further categorized to capture distinct intervention approaches and subthemes related to behavioral approaches, parent–caregiver education, and contextual intervention. The results for each theme follow.
Sleep and Rest
Nineteen studies were included: Fourteen Level I randomized controlled trials (RCTs), 2 Level II nonrandomized studies, and 3 Level III one-group studies met the criteria for the review and provided evidence related to occupational therapy interventions addressing sleep performance in children ages 0–5 yr. These studies ranged from low to moderate risk of bias and showed significantly improved outcomes for sleep and rest.
Parent Training: Infants
Five Level I studies and 2 Level II studies examined interventions for parental training for behavioral sleep problems in infants and provide strong strength of evidence for its effectiveness. In-person parental education on behavioral strategies to improve infants’ sleep occurred 1:1 and in groups. Parents can learn the difference between types of infant cries and when to assist with soothing, as well as controlled comforting and anticipatory guidance to encourage self-soothing in infants (Hall et al., 2015; Hiscock et al., 2014; Kusanagi et al., 2011; Salisbury et al., 2012). In addition, techniques of bedtime fading and gradual extinction are beneficial (Gradisar et al., 2016). These interventions led to significantly improved self-soothing, decreased sleep latency (time to fall asleep), and decreased nighttime wakings (Hall et al., 2015). When a 5-yr follow-up was conducted, no long-term negative effects from behavioral infant sleep intervention were found (Price et al., 2012).
Parent Training: Toddlers
One Level I, 1 Level II, and 2 Level III studies examined interventions for parental training for behavioral sleep problems in toddlers. Typically developing children (Blunden, 2011) and children with autism spectrum disorder (ASD; Johnson et al., 2013; Malow et al., 2014) benefit from group and individual parent behavioral intervention training, including camping out, extinction, communication and sensory strategies, and setting bedtime routines based on sleep hygiene. These interventions produced significant improvements in sleep latency, bedtime resistance, sleep duration, and night wakings and have moderate for their effectiveness.
Internet-Delivered Training
One Level I study (2 articles, the initial findings and a long-term follow-up) and 1 Level II study examined interventions for internet-delivered interventions for parents of infants and toddlers and provide moderate strength of evidence. Distance interventions providing general information and interventions that were customized to families led to significantly improved outcomes in child and maternal sleep. These outcomes included sleep duration, sleep latency, and frequency and duration of night wakings (Mindell et al., 2011a, 2011b; Schlarb & Brandhorst, 2012).
Massage
Two Level I studies examined the use of massage for sleep in infants and provide low strength of evidence because of their conflicting results. Average sleep duration significantly increased in colicky infants whose parents completed massage at home after training; this intervention was more effective than rocking the infant (Sheidaei et al., 2016). In an earlier study conducted by Yates et al. (2014), massage was provided in the NICU environment but was found to cause wakefulness as opposed to sleep.
Positioning Devices
One Level I study examined the use of a positioning device for sleep in infants and provides moderate strength of evidence (Lacina et al., 2015). Infants on the conformational positioner spent significantly less time in alert, active awake, and crying states than control infants. Electroencephalography showed higher efficiency and time in deep and light sleep, with less time awake (Lacina et al., 2015).
Media Use
One Level I study examined the influence of visual media on sleep in toddlers and provides moderate strength of evidence (Garrison & Christakis, 2012). In this RCT, caregiver education on healthy media use in preschoolers led to a significant decrease in parent-reported sleep problems over 18 mo.
Kangaroo Care
One Level I study examined the impact of kangaroo care on infant sleep and provides moderate strength of evidence. Infants in the KC group had significantly greater mean deep sleep time and quiet awake and alert states (Kusanagi et al., 2011).
Toileting
Two Level I RCTs, 3 Level III studies, and 2 Level IV case-series study met the criteria for the review and provide evidence related to occupational therapy interventions addressing toileting in children ages 0–5 yr. These studies ranged from low to moderate risk of bias.
Caregiver Education
Four studies (3 Level III and 1 Level IV) used a toilet training approach that included caregiver education and coaching and caregiver-implemented interventions. Protocols that taught the use of positive reinforcement and rewards for in-toilet elimination, scheduled toileting sits, increased fluid intake during training, and the exclusion of punitive or negative language resulted in significant changes in achieving more frequent in-toilet eliminations, more frequent child-initiated toileting, and earlier achievement of complete dryness (Cicero & Pfadt, 2002; Keen et al., 2007; Law et al., 2016; Rinald & Mirenda, 2012). These studies provide a low strength of evidence as a result of predominantly low levels of available evidence.
Punitive Language
One Level I study (RCT) focused specifically on educating parents to avoid negative and punitive language around defecation. This study found that exclusion of negative language regarding defecation did not reduce the incidence of stool toileting refusal and hiding during defecation, but it significantly reduced the duration of stool toileting refusal and promoted complete toilet training sooner than without this specific parent education (Taubman et al., 2003). Because only 1 Level I study was found, the strength of evidence for the findings was moderate.
Wetting Alarm
One Level I (RCT) study found that significantly more children became fully toilet-trained (dry) by wearing a wetting alarm diaper during waking hours, compared with children who wore a placebo alarm (Vermandel et al., 2009). Due to only having 1 Level I study, this provides moderate strength of evidence for this finding.
Multidisciplinary Approach in Cerebral Palsy
One Level IV case series examined a multidisciplinary approach to toileting for children with cerebral palsy. Results indicated that mitigating all medical, coordination, and perceptual factors before engaging in occupational therapy adaptive and psychological behavioral interventions can assist in increasing independence in bowel and bladder management (Millard et al., 2013). This Level IV study provides low strength of evidence, resulting in insufficient evidence to draw conclusions about this approach.
Feeding and Eating
Ten Level I RCTs, 1 Level II nonrandomized study, and 3 Level III one-group studies met the criteria for the review and provided evidence related to occupational therapy interventions addressing feeding performance in children ages 0–5 yr. The risk of bias of these studies ranged from low to moderate.
Repeated Exposure
Five Level I studies addressed repeated exposure to nonpreferred foods with and without modeling and various types of rewards. The available studies provide strong evidence for repeated exposure approaches. Outcomes for target food acceptance are significant and most improved when exposure is paired with modeling and rewards. Using tangible rewards with exposure is significantly more effective than using social rewards. Repeated exposure alone is not as effective as exposure paired with reward. Preparation of the target food (e.g., raw or cooked) did not have a significant effect on outcomes. We should note that all studies were conducted with children with typical eating patterns (Corsini et al., 2013; de Wild et al., 2017; Holley et al., 2015; O’Connell et al., 2012; Remington et al., 2012).
Non-Nutritive Suck
One Level I and 1 Level II study addressed oral stimulation and non-nutritive sucking (NNS) before feeding sessions with preterm infants. The available studies provide moderate evidence for non-nutritive suck and oral stimulation approaches. Oral stimulation and NNS before a feeding session significantly increased feeding rate early in a feeding session but had no effect on overall volume consumed. NNS before oral feeding significantly improved arousal state for a feeding session. Mother’s voice paired with NNS significantly improved oral feeding outcomes (Chorna et al., 2014; Hwang et al., 2010).
Parent Training
Two Level I and 3 Level III studies addressed parent training programs for child feeding-related behaviors. The available studies provide strong evidence for parent training programs for decreasing stress and mealtime behaviors. They provide low evidence for dietary variety and nutritional status because of inconsistency in findings across individual studies for these outcomes. The studies primarily used behavioral approaches, such as escape extinction, positive reinforcement, response fading, and task chaining. Training focused on supporting a structured and routine mealtime. The interventions used a combination of didactic and guided interactive activities. Results indicated significantly decreased reports of parenting stress and mealtime behaviors, but no differences in dietary variety or nutritional status were achieved (Johnson et al., 2015; Maestro et al., 2016; Sharp et al., 2014; Sobko et al., 2017; Wen et al., 2011).
Tube Feeding Weaning
Two Level I studies addressed intensive tube feeding weaning programs and provided strong evidence for these interventions. A hunger provocation program (Hartdorff et al., 2015) and an outpatient behavioral program (Sharp et al., 2016) both reported significant improvements in the achievement of full oral feeds, increased volume consumed orally, and body mass index–height ratio and weight gain compared with a waitlist control group (Hartdorff et al., 2015) or a standard-of-care outpatient treatment comparison group (Sharp et al., 2016).
Discussion
The purpose of this review is to provide occupational therapy practitioners with evidence supporting the use of intervention strategies to enhance the ADL, rest, and sleep performance of children ages 0–5 yr. Since the previous systematic review (Howe & Wang, 2013), many studies have been published that add to the depth of knowledge in this practice area. This was especially notable for studies focused on toileting and sleep, themes that were not included in the previous review.
Sleep and Rest
Interruption of routines surrounding the occupation of sleep for infants and toddlers has a profound impact on the health and well-being of children and their caregivers. The 19 articles that met criteria provided moderate to high strength of evidence for interventions to improve infant and toddler sleep and rest. However, these articles were further subdivided into seven subthemes because the age range, method of delivery, and intervention methods varied. The strongest evidence emerged for educating parents to implement behavioral interventions to improve infant and toddler sleep factors, including reducing crying, decreasing the number and duration of night wakings and time to fall asleep (sleep latency), and increasing sleep duration. Although occupational therapy practitioners were not always the health professionals delivering these interventions, these types of interventions fall into the scope of occupational therapy in EI and NICU settings.
Toileting
Toilet training is often a challenging milestone in the daily life of families with young children. Articles reviewed indicated that toileting can be taught to typically developing children with behavioral approaches such as increasing fluid intake, scheduled toileting visits, and positive reinforcement for in-toilet elimination. Significant positive effects were found for reducing or refraining from negative or punitive language when toileting errors or defecation occur. Parent–caregiver education and coaching approaches are an effective intervention mechanism to supplement or replace in vivo training by a clinician or specialist. Occupational therapy practitioners should consider these practices to develop and support families in tailored toileting strategies to enhance ADL performance, health, and quality of life for toddlers and young children with and without developmental disabilities.
Feeding and Eating
Mealtimes are a critical routine in the life of families with infants and toddlers and incorporate nourishment, motor skills, and social relationship building. For young children with typically developing feeding mechanics, skills, and behaviors, there are significant positive effects for repeated exposure paired with reinforcement of a target food to increase consumption and preference for that food. Parent–caregiver education and coaching approaches are an effective intervention to reduce mealtime behaviors and parental stress. Behavioral strategies such as positive reinforcement, response shaping, and extinction are effective in parent training, particularly for feeding challenges that require more intensive intervention strategies. Education and behavioral strategies can be used to develop and support families in tailored mealtime strategies to enhance feeding performance, health, and quality of life for infants and young children.
The studies included in this review ranged from Level I to III evidence; Level IV studies were included for toileting, an outcome that did not have sufficiently high levels of evidence. All outcome measures were related to performance skill or behaviors during ADL routines; however, a meta-analysis of results is not possible because of the wide variety of measurement tools. Many studies focused on typically developing study participants; others recruited children with disabilities or developmental delays. Therefore, improvements reported across themes may not be generalizable to all children younger than age 5 yr.
Although the evidence to support behavioral interventions to improve sleep for children with ASD or developmental delays is strong, most other areas of intervention covered in this review did not have strong-enough evidence to make recommendations for intervention with specific populations such as children with cerebral palsy. This represents a gap in the literature for interventions tailored to improving ADL performance in prevalent diagnosis groups. However, many children ages 0–5 yr referred to an occupational therapy practitioner are done so without a formal diagnosis for an unspecified developmental delay in the areas of sleep, toileting, or feeding, and interventions can thus can be guided by this review.
Only a few studies included a long-term follow-up component in their design; therefore, whether many of the improvements discussed would be maintained beyond the study period is unclear. However, performance of occupations such as sleep and dressing skills follow a typical developmental trajectory and are likely to improve as a child ages. For example, sleep–wake difficulties look very different in an infant and in a 6-yr-old.
Limitations
This review had an extensive list of search terms. The inclusion criteria and broad search term list returned studies with wide-ranging outcomes. All outcome measures were related to performance skills or behaviors during ADL routines; however, a meta-analysis of results is not possible because of the wide variety of measurement tools and diagnostic populations. The review is potentially limited by studies missed during our searches, lack of Level I studies for some themes, and the risk of publication bias. In addition, we only looked at English language articles. The review did not find evidence related to dressing or grooming ADLs for this age group, even with a secondary search with additional search terms. It is possible that evidence for these skills may not have been captured and could be embedded in articles about general ADL participation.
Future Directions
Many valuable studies were included in this review to inform occupational therapy practice with young children ages 0–5 yr. However, many gaps remain and limit conclusions for certain outcomes. Additional well-designed studies that examine the impact of toddler media consumption, conformational positioning devices for infants, and infant massage are needed to increase the strength of evidence for these interventions. Only 1 or 2 articles were included for each of these interventions, which limits their generalizability across populations and practice settings. Moreover, more research is needed to understand the effects of alarm devices and video modeling approaches to toileting interventions. Finally, as studies of effective feeding and eating interventions are developed, more information and research are needed to understand how intervention strategies influence nutritional intake volume and variety, in addition to mealtime stress and behaviors.
Implications for Occupational Therapy Practice
The interventions examined in this review that showed moderate to high strength of evidence can be effectively incorporated into occupational therapy practice with young children ages 0–5 yr and their families. Occupational therapy practitioners often work closely with families on ADL performance and sleep routines in the natural context of EI practice. Parent coaching as a part of family-centered practice involves addressing the needs of the parents and the child to support the accomplishment of family goals (Graham et al., 2014).
Many studies in this review demonstrated strong evidence for parent education and coaching strategies to improve feeding, toileting, and sleep routines. Occupational therapy practitioners can also incorporate reinforcement, chaining, shaping, and exposure strategies to improve toileting independence and mealtime success in an early childhood or preschool setting. Integrated service delivery models support the incorporation of related services, such as occupational therapy, into the natural settings of early childhood education. Occupational therapy practitioners can build these strategies into classroom, snack time, and nap routines (Bazyk et al., 2009).
Finally, occupational therapy interventions play a unique and critical role in supporting the feeding and sleep routines of very young infants and children in the NICU and inpatient hospital programs. Occupational therapy practitioners can support providers and families by directly incorporating kangaroo care and positioning devices, caregiver education, NNS protocols, and hunger provocation programs as effective strategies.
Conclusion
This systematic review examined the effectiveness of occupational therapy interventions to address ADLs, sleep, and rest in children ages 0–5 yr. Benefits of these interventions include improved falling and staying asleep, more frequent child-initiated toileting, and fewer negative mealtime behaviors. Overall, in many studies, parenting stress was a common outcome that was reduced across all themes. We found moderate to high strength of evidence for sleep interventions, low to moderate strength of evidence for toileting interventions, and moderate to high strength of evidence for feeding interventions.
Footnotes
Acknowledgments
This systematic review project was supported by the American Occupational Therapy Association Evidence-Based Practice Program. We acknowledge Molly Grabill for her contributions to this project. The authors report no conflict of interest.
Evidence and Risk-of-Bias Tables
Risk-of-Bias Table
| Citation | Selection Bias | Performance Bias: Blinding of Participants and Personnel | Detection Bias | Attrition Bias: Incomplete Outcome Data | Reporting Bias: Selective Reporting | ||
|---|---|---|---|---|---|---|---|
| Random Sequence Generation | Allocation Concealment | Blinding of Outcome Assessment: Self-Reported Outcomes | Blinding of Outcome Assessment: Objective Outcomes | ||||
|
|
|||||||
| Chorna et al. (2014) | + | + | + | + | + | + | ? |
| Corsini et al. (2013) | + | + | − | ? | ? | − | + |
| de Wild et al. (2017) | + | + | + | + | + | + | + |
| Hartdorff et al. (2015) | + | + | + | + | + | + | + |
| Holley et al. (2015) | + | + | + | + | + | + | + |
| Hwang et al. (2010) | − | − | − | − | − | − | + |
| Johnson et al. (2015) | − | − | − | − | − | − | − |
| Maestro et al. (2016) | − | − | − | − | − | + | + |
| O’Connell et al. (2012) | + | − | − | − | − | + | + |
| Remington et al. (2012) | + | + | − | − | − | + | + |
| Sharp et al. (2014) | + | − | − | − | − | ? | + |
| Sharp et al. (2016) | + | − | + | + | + | + | + |
| Sobko et al. (2017) | − | − | − | − | − | + | + |
| Wen et al. (2011) | + | + | + | + | + | − | + |
|
|
|||||||
| Cicero & Pfadt (2002) | − | NA | − | − | − | + | + |
| Keen et al. (2007) | − | − | − | − | − | + | + |
| Law et al. (2016) | − | NA | − | − | − | + | + |
| Millard et al. (2013) | − | NA | NA | NA | NA | + | + |
| Rinald & Mirenda (2012) | − | − | − | − | − | + | + |
| Taubman et al. (2003) | + | + | + | NA | + | + | + |
| Vermandel et al. (2009) | + | − | − | NA | + | + | + |
|
|
|||||||
| Austin et al. (2013) | NA | NA | NA | NA | − | + | + |
| Bastani et al. (2017) | + | + | − | − | − | + | + |
| Blunden (2011) | NA | NA | NA | NA | NA | + | + |
| Garrison & Christakis (2012) | + | − | − | − | − | + | + |
| Gradisar et al. (2016) | + a | − | − | − | + | + | + |
| Hall et al. (2015) | + | - | + | + | + | + | + |
| Hauck et al. (2012) | NA | NA | + | + | − | − | + |
| Hiscock et al. (2014) | + | + | − | − | − | + | + |
| Johnson et al. (2013) | + | − | − | − | − | + | + |
| Kusanagi et al. (2011) | NA | − | − | − | − | + | + |
| Lacina et al. (2015) | + | − | − | − | + | + | + |
| Malow et al. (2014) | + | − | − | + | − | + | + |
| Mindell et al. (2011a) a | − | − | − | + | NA | + | + |
| Mindell et al. (2011b) b | − | − | − | + | NA | + | + |
| Price et al. (2012) c | + | + | − | − | − | + | + |
| Salisbury et al. (2012) | − | − | − | + | NA | + | + |
| Schlarb & Brandhorst (2012) | NA | NA | NA | NA | NA | + | + |
| Sheidaei et al. (2016) | − | + | − | − | NA | + | + |
| Yates et al. (2014) | NA | − | − | NA | − | + | + |
Note. Categories for risk of bias are as follows: + = low risk of bias; − = high risk of bias; ? = unclear risk of bias; NA = not applicable because of study design. Risk-of-bias table format adapted from “Assessing Risk of Bias in Included Studies,” by J. P. T. Higgins, D. G. Altman, and J. A. C. Sterne, in Cochrane Handbook for Systematic Reviews of Interventions (Version 5.1.0), by J. P. T. Higgins and S. Green (Eds.), 2011, London: Cochrane Collaboration. Retrieved from http://handbook-5-1.cochrane.org. Copyright © 2011 by The Cochrane Collaboration.
But allowed to request to swap conditions on request.
One-year follow-up of Mindell et al. (2011a).
Long-term follow-up of Hiscock et al. (2014).
This table is a product of the American Occupational Therapy Association's Evidence-Based Practice Project and the American Journal of Occupational Therapy. Copyright © 2020 by the American Occupational Therapy Association. It may be freely reproduced for personal use in clinical or educational settings as long as the source is cited. All other uses require written permission from the American Occupational Therapy Association. To apply, visit www.copyright.com.
Suggested citation: Gronski, M., & Doherty, M. (2020). Interventions within the scope of occupational therapy practice to improve activities of daily living, rest, and sleep for children ages 0–5 and their families: A systematic review (Table A.2). American Journal of Occupational Therapy, 74, 7402180010. https://doi.org/10.5014/ajot.2020.039545
*
Denotes article included in systematic review.