
Abstract
Children and youth participate in occupations that change over time as they age, mature in skills, and have new interests and responsibilities. Such occupations include instrumental activities of daily living (IADLs), which are complex and diverse and support the routines of daily life. The occupations of rest and sleep are also considered foundational and support optimal performance of meaningful daily life tasks (American Occupational Therapy Association [AOTA], 2014). As youth prepare for greater independence and progress toward adulthood, participation in and performance of IADLs become increasingly relevant, and interventions tailored to this age group’s unique characteristics reflect client-centered practice.
Occupational therapy is an integral part of health service delivery for children and youth with special health care needs as well as for children in school and community programs (Case-Smith & O’Brien, 2015). One of the four major goals of Healthy People 2020 is to “promote quality of life, healthy development, and healthy behaviors across all life stages” (U.S. Department of Health and Human Services, 2010, p. 5). Children and adolescents stand to benefit as health initiatives and therapy services addressing concerns such as obesity, sedentary lifestyle, safety, and poor nutrition become more prevalent.
Sleep, fitness, safety, nutrition, and overall health management, although relevant to all youth, may be especially important for children with chronic conditions and those who experience environmental or developmental barriers to participation. Supporting self-management for pediatric patients is recommended and is more critical for children with conditions that have a medical or social impact (Lozano & Houtrow, 2018). Sleep issues are more prevalent among children with autism spectrum disorder (ASD; Cavalieri, 2016) and developmental coordination disorder (Barnett & Wiggs, 2012) than among typically developing children. In addition, although inadequate rest and sleep are considered a public health problem (Centers for Disease Control and Prevention [CDC], 2015), occupational therapy practitioners often overlook sleep as an occupation of interest (Green, 2008).
Interventions within the scope of occupational therapy are diverse; thus, they require that practitioners seek guidance from intervention effectiveness studies to make quality decisions regarding therapy strategies. In keeping with AOTA’s recommendations from the Choosing Wisely® initiative, practitioners should seek purposeful and occupation-based interventions to enhance motivation and outcomes (Gillen et al., 2019). Armed with targeted interventions, the profession makes a unique contribution to the promotion of health and wellness and is equipped to address IADL and rest and sleep outcomes among children who experience barriers to achieving optimal participation and performance.
The objective of this review was to use a systematic process to search for, appraise, and synthesize the evidence for the effectiveness of occupation- and activity-based interventions for children and youth and contribute to the development of AOTA practice guidelines. The review was guided by the PICO (Problem/Patient/Population, Intervention/Indicator, Comparison, and Outcome) question “What is the evidence for the effectiveness of activity- and occupation-based interventions within the scope of occupational therapy practice to improve activities of daily living (ADLs), IADLs, play and leisure, and rest and sleep for children and youth ages 5–21 yr”? In this article, we specifically address the findings for IADLs and rest and sleep; the remaining categories are the focus of a second article (Laverdure & Beisbier, in press).
Method
This systematic review was supported by AOTA as part of the Evidence-Based Practice (EBP) Project. Using Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) methodology (Moher et al., 2009). The categories of IADLs and rest and sleep were critically appraised and analyzed separately and then combined for this article.
Search and Screening Strategy
Search terms for the systematic review were developed by the AOTA research methodologist with input from AOTA staff; the review authors; and an advisory group of occupational therapy pediatric practitioners, scholars, and leaders.
The AOTA medical research librarian searched MEDLINE, PsycINFO, CINAHL, ERIC, and OTseeker for articles published between 2000 and 2017. The Cochrane Database of Systematic Reviews was also used as an additional information source. Search terms are listed in Table 1. The results of the literature search were collected by the medical librarian in citation manager software, and duplicates were removed by the AOTA research methodologist. The research methodologist conducted the first review of the search results, eliminating articles that did not meet the study criteria.
Key Search Terms for the Systematic Review
Note. DIR = Developmental, Individual differences, Relationship model; NIDCAP = Newborn Individualized Developmental Care and Assessment Program.
The results were exported to the two reviewers (the authors), who completed the subsequent stages of final review. Articles were included if they were peer-reviewed Levels I, II, or III evidence; were published in English; were within the scope of occupational therapy practice (AOTA, 2014); were with populations of children and youth ages 5–21 yr; included occupation- or activity-based interventions; and had IADL or sleep and rest outcomes. Articles were excluded if they were dissertations, theses, presentations, or proceedings published before reviews; outside the scope of occupational therapy practice; lacking occupation- or activity-based interventions; Level IV and V studies; or with populations younger than age 5 yr or older than age 21 yr. We independently screened the articles for eligibility and then compared our choices to determine which articles to include in the review (Figure 1). We reached consensus on all articles in question. An evidence table was completed after a detailed reading of the articles (Table A.1). This table was reviewed by AOTA staff and the EBP Project consultant.
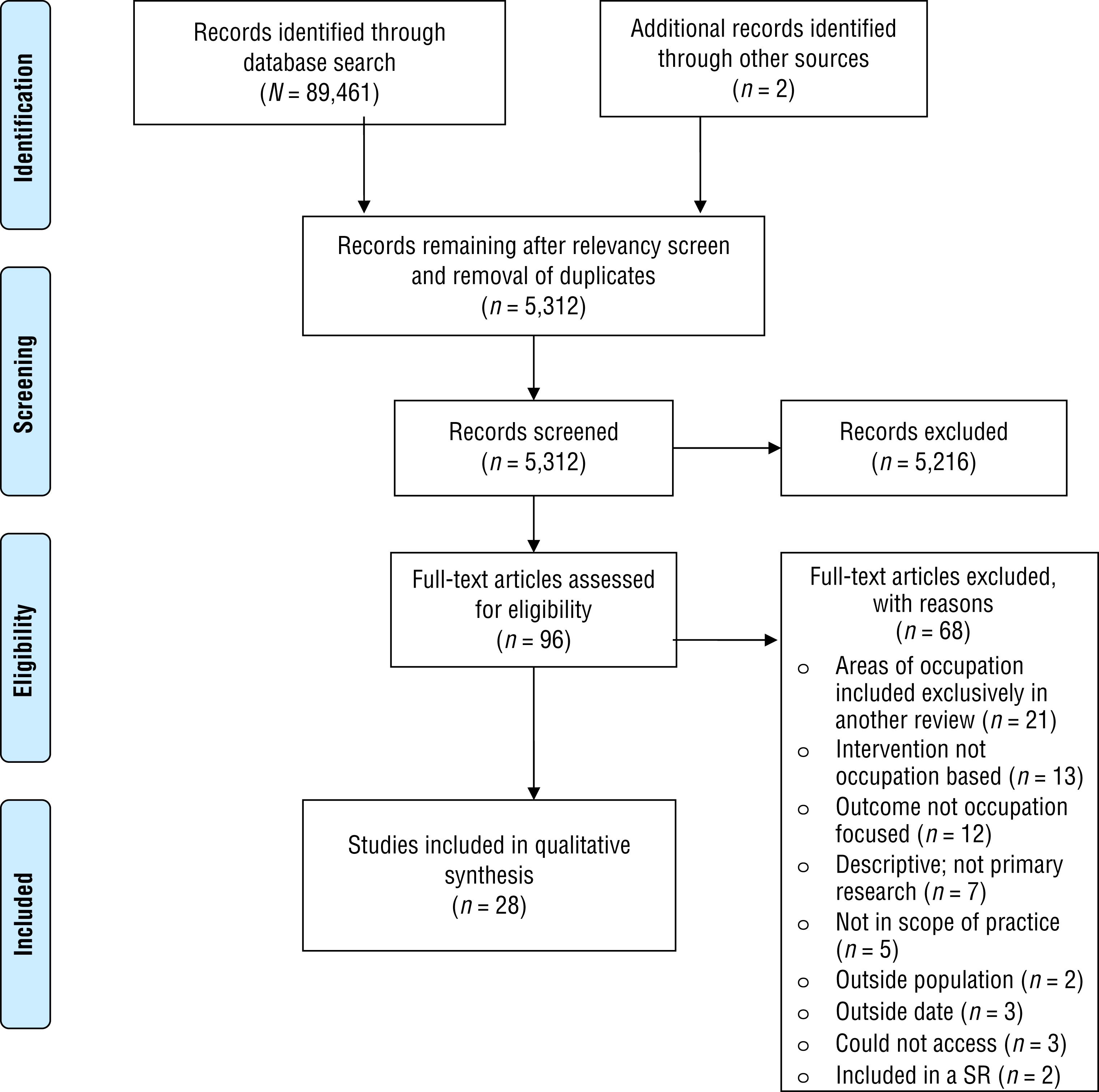
Flow diagram for reviewed studies.
Risk of Bias and Strength of Evidence
We individually assessed each article for risk of bias as described in the Cochrane risk-of-bias guidelines (Higgins et al., 2011) and reached consensus on the risk of bias of all studies. Tables A.2 and A.3 display the specific risk-of-bias information for the included studies. Articles were grouped into themes, and each theme was analyzed for strength of evidence, which informed the final recommendations for practice, education, and research. Study design, findings, and risk of bias all influenced the strength-of-evidence designations (Table 2; U.S. Preventive Services Task Force, 2018).
Strength of Evidence Criteria
Note. From U.S. Preventive Services Task Force (2018).
Results
We identified 28 articles for inclusion in the final synthesis for IADLs and rest and sleep (see Figure 1). The IADL category was organized into outcome themes of health maintenance and management and one broader category that included safety, driving, and communication management. Most studies that met the inclusion criteria for IADLs measured health maintenance and management outcomes, and those studies were grouped into three categories: physical activity and fitness, dietary and nutrition, and health routines and wellness. The outcomes related to rest and sleep were also analyzed and are discussed separately.
Health Maintenance and Management
Physical Activity and Fitness
Six Level I randomized controlled trials (RCTs) with low to moderate risk of bias and 1 Level II (Wong et al., 2016) and 2 Level III studies with moderate to high risk of bias measured physical activity outcomes. Of the 9 studies, 6 were conducted in schools; the remaining 3 studies were conducted outside of the school day or location. Most participants were not identified as having a disability or specific condition; however, 1 study’s participants were children with cerebral palsy (Maher et al., 2010).
Four Level I studies and 1 Level III study with statistically significant findings provide strong evidence that occupation- and activity-based interventions provided in a school setting increase health outcomes of physical activity and fitness. Beyler et al. (2014) measured the effect of a Playworks program that provided organized recess activities, after-school activities, class game time, and coach training and found a significant impact on teacher-reported student participation in physical activity during recess as well as a significant improvement in vigorous physical activity during recess. A Level III study conducted by Huberty et al. (2011) focused on elementary-school-aged children in Grades 3–5. The children participated in the Ready for Recess program, which included activity zones and access to equipment. Participation in physical activity was significantly higher at posttest for both recess and school-day outcomes. Another intervention that included interactive lessons, use of pedometers, and facilitation of creative strategies to increase physical activity was implemented with eighth-grade students (Suchert et al., 2015). The results of this Level I study included significant positive change in days of moderate to vigorous physical activity and an increase in sports in the intervention group with no or nonsignificant changes in the control group.
Sutherland et al. (2016) conducted a 24-mo school-based intervention for adolescents with a focus on physical activity promotion via student physical activity plans, fitness activities and lessons, provision of equipment, and promotion of community activities and parent engagement. The evidence indicates that this intervention was effective in increasing daily minutes of moderate to vigorous physical activity. A second study with adolescent participants (Whittemore et al., 2013) used an online program focused on obesity prevention. The authors found that both in-class and homework versions of the HEALTH[e]TEEN program resulted in significant findings for physical activity as measured by the Youth Risk Behavior Survey (CDC, 2009). In a Level I study of seventh- to ninth-grade girls, Casey et al. (2014) investigated the impact of a 12-mo school–community linked program that incorporated a sport and recreational unit that included self-management strategy building in physical education class. There were no statistically significant changes in self-reported physical activity levels.
For occupation- and activity-based interventions provided in a nonschool setting to increase health outcomes of physical activity and fitness, the strength of evidence was low. One Level I study with low risk of bias and 1 Level II study and 1 Level III study with high risk of bias all had nonsignificant findings. In a Level III cohort study, Hogg et al. (2012) evaluated the use of a lifestyle and activity curriculum paired with dance. The participants used diaries to track behaviors following the after-school intervention. Findings revealed an increase in physical activity but did not reach statistical significance. Maher et al. (2010) conducted an RCT using eight self-directed, interactive web-based modules focused on lifestyle physical activity. Outcome measures showed nonsignificant positive trends for activity behavior and exercise knowledge for children with cerebral palsy. Wong et al. (2016) conducted three 6-wk sessions of an after-school program that provided structured physical activity and lessons on nutrition and healthy habits. Monitors indicated no improvement in physical activity.
Dietary and Nutrition
Moderate-strength evidence supports occupation- and activity-based interventions to effect positive change in dietary outcomes for children ages 5–21 yr. Six studies (3 RCTs, 2 nonrandomized Level II studies, and 1 Level III study), all with moderate to high risk of bias, met the inclusion criteria. Five of the six studies resulted in statistically significant changes in nutrition behaviors resulting from the implementation of previously established programs and skills training.
Anand et al. (2015) used a self-administered questionnaire to measure the effects of a skills-based training approach of interactive role-play and homework. The intervention focused on making healthy choices and positive dietary behavior of teens. The intervention group showed significant improvement in knowledge, attitude, and practices, including eating fruits and vegetables. A Level I RCT with third- to fifth-grade participants was conducted as part of an after-school program, LA Sprouts (Davis et al., 2016). The intervention included interactive and activity-based instruction in cooking and nutrition and gardening. The intervention group improved its identification of vegetables and nutrition and gardening knowledge and increased gardening at home. A third study by Whittemore et al. (2013) implemented a web-based HEALTH[e]TEEN program in which the participants engaged in self-directed lessons supported by interaction with a coach and peers that resulted in statistically significant improvements in healthful eating behaviors.
Evidence from 1 Level II and 2 Level I studies supports pairing a skills-based interactive curriculum with structured physical activity. Hogg et al. (2012) used an intervention consisting of a lifestyle and nutrition curriculum paired with a dance activity. Findings revealed positive changes in eating behaviors and food selection, but statistical significance was not reported. Wright et al. (2012) used a 6-wk family-centered program (Kids Nutrition and Fitness) that targeted nutrition education and physical activity. Conducted with 8- to 12-yr-old children from low-income schools, this low-risk-of-bias RCT resulted in statistically significant improved dietary behaviors among participants compared with the control group. Although Wong et al. (2016) found no improvements in actual dietary habits after a 6-wk after-school healthy living program featuring structured physical activity paired with lessons on nutrition and interactive healthy habits, participants did gain an understanding of the impact of eating habits.
Health Routines and Wellness
Four Level I studies (1 systematic review and 3 RCTs) met criteria for health routines or wellness. The health management outcomes included health-related decision making, medication adherence, and management of pain and activity. Of the 3 studies with significant positive findings, 2 had a family or parent component (Letourneau et al., 2013; Palermo et al., 2009). Moderate-strength evidence supports education and skills training interventions using small-group activities and activity-based cognitive–behavioral strategies for 9- to 18-yr-old youth with a health concern.
Evidence from 2 Level I studies (moderate and high risk of bias) supports inclusion of family and parents throughout the therapy process. Letourneau et al. (2013) used an RCT to study the effects of a family-centered, home-based interactive cognitive–behavioral approach to address medication adherence for youth with HIV. Statistically significant changes in medication adherence were found in the intervention group. Palermo et al. (2009) measured the impact of a web-based self-guided interactive module with a sample of 11- to 17-yr-old youth. Children and parents completed weekly health-focused activities with accompanying homework and feedback provided by a professional. Findings for the treatment group reached statistical significance for a reduction in activity limitations and pain intensity.
A systematic review of 5 studies measured interventions for health-related decision making by youth. Of the 5 studies, 4 measured the impact of interactive coaching practices and had nonsignificant findings. One study showed that an intervention in the form of an activity-based workshop resulted in significantly increased quality of overall decision making. Although the review had low risk of bias, the overall quality of the studies included was mixed, and they lacked detail (Feenstra et al., 2014). Srof et al. (2012) evaluated an interactive small-group coping skills training intervention with 14- to 18-yr-old youth that focused on making health-related decisions for asthma self-management. Although the primary outcomes were quality-of-life measures and the overall scale failed to reach significance, the Activity subscale of the Pediatric Asthma Quality of Life Survey demonstrated significance in both between-group and within-treatment-group comparisons.
Driving and Community Mobility, Safety, and Communication Management
Because of the scoping nature of the IADL category, another, more diverse grouping of outcomes emerged (driving and community mobility, safety, and communication management). The interventions in the studies meeting the criteria fell into two main categories: technology-based interventions and activity-based coaching or skills training. There were 5 studies (3 Level I [2 RCTs and 1 meta-analysis] and 2 Level III studies) in which the intervention was primarily or partially technology based. All interventions resulted in positive outcomes, but the results reached statistical significance in the meta-analysis and 1 Level III study.
Two studies were categorized into activity-based coaching or skills training interventions (1 Level I RCT with moderate risk of bias and 1 Level III study with high risk of bias). Both studies in this intervention category resulted in statistically significant findings for IADL outcomes for teenagers. Overall, the strength of evidence for occupation- and activity-based interventions involving interactive training and coaching is moderate and that for technology-based interventions is low. Small sample sizes and moderate to high risk of bias were limiting factors in most of the studies and should be considered when interpreting the true intervention effect and application to practice.
Technology-Based Interventions
A four-group Level I RCT with a large sample of 7- and 8-yr-old children was conducted to measure safety during street crossing. The interventions included individualized training in an interactive virtual pedestrian environment, individual training at street-side locations, and training using widely available video and internet programs on pedestrian safety. Both street-side safety training and virtual reality show promise to train children to cross streets safely; however, most findings did not reach statistical significance for within- and between-groups measures, and the study was assessed as having a high risk of bias (Schwebel et al., 2014).
Two studies measured communication management outcomes after a technology-based intervention. Grynszpan et al. (2014) conducted a low-risk-of-bias meta-analysis of technology-based interventions used specifically with children with ASD. Length of session and presence of a trainer appeared to be factors resulting in greater gains in performance. The studies included in Grynszpan et al.’s analysis produced a moderate effect on outcomes of facial affect recognition and communicative behavior (IADL of communication management). Using a Level III design with high risk of bias, Ke and Im (2013) implemented a virtual reality intervention using role-play and situation-specific communication between participants and facilitators. Observation and the Social Skills Questionnaire (Spence, 1995) provided outcome data showing increased performance, but statistical significance was not reported.
Two studies measuring driving outcomes met criteria. Ekeh et al. (2013) measured the effect of a 12-module interactive web program as a driving intervention for new teen drivers. Safe driving outcomes measured via driving records were not statistically significant. A Level III study with a small sample of teens with attention deficit hyperactivity disorder (ADHD; n = 7) was conducted using an 8-wk parent–teen program (Supporting a Teen’s Effective Entry to the Roadway). The activity-based program included driving simulation, behavioral strategies, and teaching and discussion components. Outcomes were measured via CarChip monitors and a driving behavior questionnaire. Braking, speed, and overall driving skill measures improved, but the effect size was small (Fabiano et al., 2011).
Activity-Based Education and Training and Coaching
A single RCT (moderate risk of bias) measuring driving outcomes with two intervention groups and one control group met the criteria for inclusion. One intervention group received activity-based training with a focus on higher order skills. The intervention included on-the-road self-evaluation exercises, video-based hazard perception training, and coaching practices. The second intervention group received more traditional behind-the-wheel training in vehicle handling. Statistically significant findings for Group 1 included improvements in car handling and composite driving and hazard perception. Group 2 had statistically significant improvement only in car handling and composite driving skills (Isler et al., 2011).
Keenan et al. (2014) implemented a Level III study (with a high risk of bias) using activity-based training and coaching via a community-based life skills program. The coaches supported clients in selecting their own goals using the Canadian Occupational Performance Measure and then practiced skills in a natural setting. The most frequently identified goals were in the IADL content areas of cooking, money management, and community mobility. For all outcomes, posttest means were greater than pretest means and ratings and had large effect sizes.
Rest and Sleep
Five studies met criteria for inclusion in this theme: three Level I studies with low risk of bias and 2 Level III studies with high risk of bias. There is strong evidence that engagement in sleep preparation activities, including sleep education, coaching, and cognitive strategies for skills in relaxation and sleep hygiene, improves overall sleep outcomes.
Two RCTs were conducted with adolescent participants. De Bruin et al. (2015) measured the effectiveness of face-to-face group therapy or guided internet therapy with adolescents with insomnia. Both intervention groups received sleep education, sleep hygiene, and relaxation activities. De Bruin et al. reported that both groups showed significant improvements in sleep outcomes compared with the control group. Another study using guided imagery interventions was found to significantly decrease sleep interference from postsurgical pain among youth who underwent orthopedic surgery for adolescent idiopathic scoliosis (Charette et al., 2015).
One Level III study that used an aquatic activity program reported significant findings. The results included significant decreases in sleep onset latency and significant increases in sleep duration for children with ASD (Oriel et al., 2016). Sciberras et al. (2011) evaluated a brief and follow-up behavioral sleep coaching program for parents of children with ADHD and behavioral sleep disorders. Results of this RCT indicated significant improvement in healthy sleep routines and sleep hygiene practices, habits and routines, quality of sleep, and daily functioning among children and their caregivers with a medium effect size. Hooke et al. (2016) found that participating in 6 wk of yoga involving poses, relaxation, gentle stretching, and breathing along with a home program did not change sleep-related symptoms in a small sample of children with a cancer history, but participants did have a significant decrease in anxiety.
Discussion
This systematic review examined the effectiveness of activity- and occupation-based interventions to promote IADLs and rest and sleep outcomes in children ages 5–21 yr. The 28 studies included varied intervention strategies, including web-based and activity-based education and interactive skills training. Although much of the literature that met the inclusion criteria was centered on IADLs of health maintenance and management and rest and sleep, a small number of studies also evaluated the impact of interventions on safety, communication management, and driving.
Occupational therapists often provide services to children in natural settings of school, home, and community. Strong evidence supports activity- and occupation-based interventions in the school setting. This was especially true of structured programs and guided activities embedded into recess and physical education classes with resultant fitness and physical activity outcomes (Beyler et al., 2014; Huberty et al., 2011; Suchert et al., 2015; Sutherland et al., 2016; Whittemore et al., 2013). Evidence also supports interventions that promote parent or caregiver involvement (Fabiano et al., 2011; Letourneau et al., 2013; Palermo et al., 2009; Sciberras et al., 2011; Sutherland et al., 2016; Wright et al., 2012). These findings highlight the benefits of family-centered practice, which is a central tenet of occupational therapy service delivery with children and youth (Case-Smith & O’Brien, 2015).
Quality rest is essential to overall health, well-being, and occupational participation (Green, 2008). Strong evidence supports occupation- and activity-based interventions, including sleep education coaching and structured physical activity to improve sleep routines and sleep quality (de Bruin et al., 2015; Oriel et al., 2016). Interventions that incorporate caregivers are likely to have greater impact and are recommended.
The results of this review also support continued exploration of web-based interventions. Evidence indicates that the use of technology is most effective when highly individualized and coupled with personal interaction with a professional (Grynszpan et al., 2014; Ke & Im, 2013). Because of the diverse applications of technology, practitioners should seek evidence specific to the intervention of choice and adhere to best-practice methods.
Limitations
Only articles in English were considered for inclusion in the systematic review process. An additional limitation was the scope of the guiding question, because the variety of interventions that fall under the umbrella of occupation- and activity-based strategies created a challenge with review and synthesis. Limitations were also noted in the body of literature; many of the studies included multicomponent interventions, some of which were not occupation or activity based. Several studies had primary outcomes that were not IADL or occupation focused but instead focused on a performance component or client factors, with the IADL outcomes considered secondary. Many studies did not include occupational therapists as the interventionists. Additional limitations include small sample size, high risk of bias in individual studies and moderate risk of bias in overall theme groups, and nonstandardized outcome measures as reported in individual studies.
Implications for Occupational Therapy Practice
The results of this review have the following implications for occupational therapy practice:
Evidence supports parent and school and community involvement throughout the course of intervention as well as provision of pediatric services in the natural context of the child’s or teenager’s routine and environments.
Practitioners should consider skills-based training strategies that include peer, family member, and therapist interaction and the use of a small-group format for service delivery with children and adolescents.
Practitioners should explore interactive technology interventions for clients, including those with ADHD and ASD, and consider pairing such interventions with skills training.
Addressing rest and sleep occupations can improve health and well-being and increase performance and participation in meaningful occupations.
Implications for Occupational Therapy Education
The results of this review have the following implications for occupational therapy education:
Academic programs need to emphasize family-centered care and provision of services in natural environments so that students are well equipped to use evidence-based service delivery models.
Knowledge of rest and sleep should be an integral part of educational curricula for occupational therapists and occupational therapy assistants.
Educators should provide opportunities for students to discover the value of occupation as both intervention and outcome while planning for service with children and youth.
Implications for Occupational Therapy Research
The results of this review have the following implications for occupational therapy research:
There is a need for more research studies with robust methodology and design that use evidence-based, reliable, and sensitive outcome measures.
Researchers should consider a focus on studies that include both occupation-based interventions and occupation as a primary outcome.
Conclusion
Participation in IADLs and sleep occupations are part of a typical routine for children and youth. Those with special health care needs or barriers to participation may require supports and professional services to meet their developmental and occupational needs. This review supports the use of occupation- and activity-based interventions as a means of facilitating occupational performance and participation for children and youth ages 5–21 yr. Occupational therapy services with this age group should be family centered and delivered in the natural context when possible. The systematic review shows that individualized and structured skills-based training within the routine of the child is effective. Although the existing evidence for technology-based interventions was low, continued advances in technology support ongoing exploration.
Footnotes
Acknowledgments
This systematic review was supported by the American Occupational Therapy Association (AOTA) and completed as part of AOTA’s Evidence-Based Practice Project. We thank Deborah Lieberman, Elizabeth Hunter, Marian Arbesman, Hillary Richardson, and Elaine Sullo for their contributions to this project in conjunction with AOTA’s Evidence-Based Practice Project. The authors report no conflicts of interest.
Appendix
*
Indicates studies that were systematically reviewed for this article.