
Abstract
Occupational therapy practitioners work with children and families to promote participation in meaningful occupations and activities of daily living (ADLs) across many settings, including early intervention (EI), schools, hospitals, and the community (American Occupational Therapy Association [AOTA], 2014). Practitioners working in EI or school settings usually provide services under the Individuals With Disabilities Education Act of 1990 (Pub. L. 101-476), which ensures that children and youth receive special education and related services, including occupational therapy. Practitioners can also serve children ages 0–5 yr through other models, including outpatient therapy. As members of interdisciplinary teams, occupational therapy practitioners provide individualized interventions relevant to children’s daily routines (Hwang et al., 2013).
Many occupational therapy interventions address parent–infant interactions, developmental milestones, and sensory exploration. Practitioners can specifically address gross and fine motor skills to promote participation in occupations such as ADLs, education, play, self-care, and social participation (AOTA, 2014; Case-Smith et al., 2013). Motor interventions for children aim to remediate motor impairments, minimize developmental delays, and support family functioning by fostering the development of routines to encourage motor development (Blauw-Hospers et al., 2011; Case-Smith et al., 2013).
Young children who receive occupational therapy services may have a medical diagnosis or delays in motor development (Case-Smith et al., 2013). For example, premature infants and those with low birthweight (LBW) are at higher risk of developmental delays (Spittle et al., 2012) and cerebral palsy (CP). As members of interdisciplinary teams, occupational therapy practitioners can address motor outcomes for young children with motor delays. A systematic review (SR) on this topic (Case-Smith et al., 2013) was completed more than 5 yr ago, and a considerable amount of new research has come out since that time. Therefore, the rationale for conducting this review is to provide the profession with up-to-date information about evidence-based interventions to guide efforts in both practice and research. This review addresses the following question: What is the evidence for the effectiveness of interventions within the scope of occupational therapy practice to promote motor development and prevent further delay for children ages 0–5 yr?
Method
This review was completed as part of AOTA’s Evidence-Based Practice Project to update the practice guidelines for children and youth. The protocol for this review is not published separately, but the process is presented in this section. The search strategy was developed by a medical librarian, a research methodologist, and AOTA staff, and it was reviewed by an advisory group. A literature search was performed by a medical librarian using MEDLINE, PsycINFO, CINAHL, OTseeker, ERIC, and Cochrane databases (Evidence-Based Medicine Reviews, Database of SRs, Controlled Trials Register, and Database of Abstracts of Reviews of Effectiveness; Table 1).
Search Terms for Motor Performance in Children Ages 0–5 Years
Note. DIR = Developmental, Individual differences, Relationship model; NIDCAP = Newborn Individualized Developmental Care and Assessment Program.
Inclusion criteria for this study were as follows: Articles were published between January 2010 and March 2017; examined interventions within the scope of occupational therapy practice as defined in the Occupational Therapy Practice Framework: Domain and Process (3rd ed.; AOTA, 2014); addressed motor skills specifically; used a Level I, Level II, or Level III design (Sackett, 1989); and included participants with a mean age of <6 yr. Exclusion criteria were as follows: presentations, conference proceedings, non–peer-reviewed research literature, and dissertations and theses; studies with a primary outcome of amount of activity (e.g., number of steps, minutes spent exercising); interventions for entire hospital units; and primary intervention of lower extremity orthotics or gait training.
The AOTA research methodologist reviewed the search results and provided citations to the authors of this review. We collected data on level of evidence (design), quality (scientific rigor), and statistical significance of findings using standardized forms provided by AOTA (Table A.1 in Appendix A). Studies were assessed for risk of bias on the basis of the Cochrane Collaboration’s tool (Higgins et al., 2011; Table A.2) and the Assessment of Multiple Systematic Reviews (AMSTAR) tool (Shea et al., 2007; Table A.3); no risks were identified that would affect the cumulative evidence.
The initial search results were reviewed by the AOTA research methodologist (Figure 1). Each abstract was reviewed by a review author on the basis of the inclusion and exclusion criteria and given a “yes,” “no,” or “maybe” rating. The review authors met to clarify criteria, and abstracts with a yes or maybe rating were reviewed by a second rater. The authors then reviewed the remaining full-text articles and included them in the final evidence table (see Table A.1). The strength of the evidence for each intervention strategy was assessed as follows: Strong evidence indicates consistent results from 2 or more Level I studies, moderate evidence indicates at least 1 Level I high-quality study or multiple lower level studies that may have inconsistent findings, and low evidence indicates a small number of low-level or flawed studies (AOTA, 2017; U.S. Preventive Services Task Force, 2018).
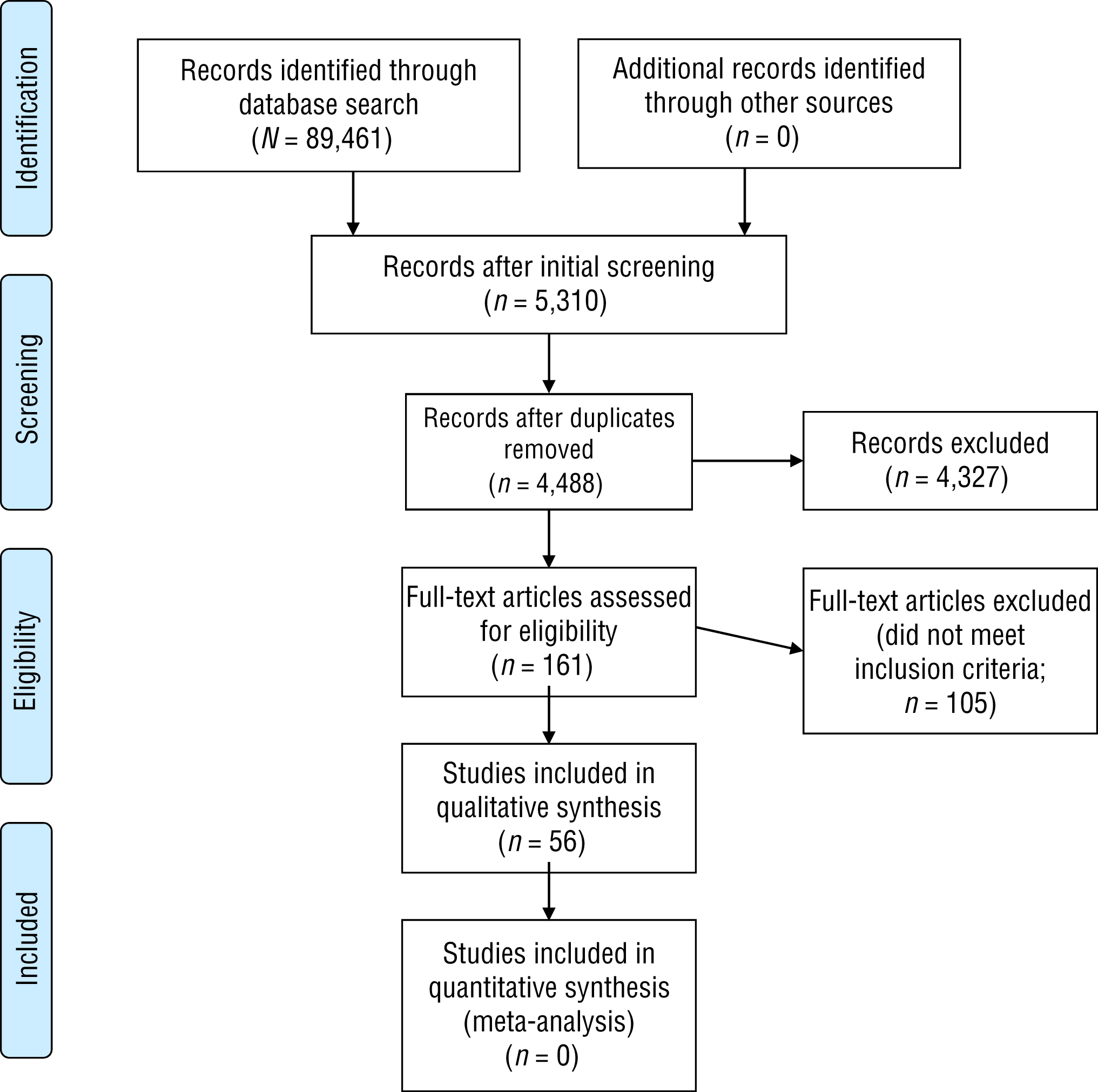
Flow diagram for inclusion and exclusion of peer-reviewed studies in the systematic review.
Results
The risk of bias for included studies was high because of weaknesses in allocation concealment, blinding of participants and personnel, and outcome assessments, largely because of the nature of the interventions studied (see Figure 1). Thus, results should be interpreted with caution. Three intervention themes were identified in the final evidence table: (1) EI for children younger than age 3 yr, (2) interventions for preschool children ages 3–5 yr, and (3) interventions for children with or at risk for CP ages 0–5 yr.
Early Intervention
Nineteen studies were related to interventions provided to children younger than age 3 yr, including 13 Level I studies (1 meta-analysis, 1 SR, and 11 randomized controlled trials [RCTs]), 5 Level II studies, and 1 Level III study. For the purpose of this study, “EI” includes any intervention for children younger than age 3 yr.
General Early Intervention
The results of an SR of EI delivered after hospital discharge to children born preterm indicated a small, significant short-term effect on motor skills compared with standard follow-up, which was not always specified but in some studies included physiotherapy in accordance with institutional policies (standardized mean difference = 0.10, p = .040; Spittle et al., 2012). The results of a meta-analysis showed a small (d = 0.12, p = .003), significant effect of EI on movement-related functions for children born preterm or with LBW (Park et al., 2014). Thus, strong evidence indicates that EI programs can have a small positive effect on motor development in the short term for preterm children.
Newborn Individualized Developmental Care and Assessment Program
An RCT investigated the impact of the Newborn Individualized Developmental Care and Assessment Program (NIDCAP) on preterm infants with severe intrauterine growth restriction in comparison with standard care. Results indicated improved motor function in the NIDCAP group on the behavior assessment at 2 wk corrected age but no significant differences at 9 mo on the Psychomotor Developmental Index of the Bayley Scales of Infant and Toddler Development, Second Edition (Bayley–II; Als et al., 2011). Moderate evidence thus indicates that NIDCAP can improve short-term motor skills.
Home-Based Parent Coaching
A feasibility RCT indicated a large effect size (d = 1.29) for Test of Infant Motor Performance scores of children who received a parent coaching program focused on teaching parents to interact with their infants using developmentally appropriate play activities that began in the neonatal intensive care unit (NICU) and continued to the home in comparison with those of a group who received standard care (Dusing et al., 2015). Another RCT indicated improvements (effect size = 0.40 standard deviation [SD]) in motor development over time for the intervention group (seen on the Bayley Scales of Infant and Toddler Motor Development, Third Edition [Bayley–III], and the Movement Assessment Battery for Children) in comparison with a standard care group, in particular for infants with bronchopulmonary dysplasia (effect size = 0.90 SD ; Van Hus et al., 2016).
Other studies showed mixed results. The results of an RCT comparing clinic- and home-based therapy with usual care for preterm infants indicated that the clinic-based therapy group showed a trend toward lower rates of motor delay, but no significant differences were found between groups (p = .05; Wu et al., 2014). In this study, the same types of activities (i.e., providing education about child development, encouraging interaction, supporting feeding skills, and providing parent support) were provided to both groups; only the location differed. Two RCTs examined routines-based EI for children with or at risk for developmental disabilities (Hwang et al., 2013) and the Mother–Infant Transaction Program for children with LBW (Nordhov et al., 2010) and found no significant differences between the intervention and control groups on primary motor outcomes. However, subscale analysis by Nordhov et al. (2010) revealed that intervention participants were significantly better than control participants at single leg stance (p = .03) and placing keys in a box with their nondominant hand (p = .03) at age 5 yr. Hwang et al. (2013) found a significant effect of intervention stage (p < .01) indicating decreasing progress in mobility functional and caregiver assistance skills over time for both groups.
Finally, two RCTs investigated the effectiveness of home-based EI in developing countries. One compared parent-implemented EI to a home-visiting program for children with birth asphyxia (Carlo et al., 2013). Significant differences were found between groups on the Bayley–II Psychomotor Developmental Index at 36 mo, with higher scores for the resuscitated group (p = .043), the nonresuscitated group (p = .016), and the combined groups (p = .002) compared with the corresponding control groups; no significant differences were found on the Ages and Stages Questionnaire. The other RCT found no significant differences in motor skills for children who received a home-based parent-coaching intervention in comparison with those who received home-based health education visits (Wallander et al., 2014).
Because of inconsistent findings, the strength of evidence is moderate that home-based parent-coaching EI can improve short-term motor development for children with or at risk for delays.
Massage
An RCT found significant improvements in gross motor skills for children with Down syndrome or CP who received parent-administered qigong massage compared with a wait-list control group (Silva et al., 2012). A Level II quasi-experimental study of parent-administered massage for preterm infants indicated no significant differences compared with standard care (Abdallah et al., 2013). Thus, moderate evidence shows that parent-administered qigong massage may improve gross motor skills but that parent-administered general massage may not.
Home Programming With Therapy
An RCT found significant improvements in gross and fine motor skills and most Pediatric Evaluation of Disability Inventory (PEDI) scores for children who received clinic-based therapy along with home programming in comparison with those who received clinic-based therapy alone (Tang et al., 2011). Home programming included task-specific or activity-focused interventions that addressed individualized treatment goals discussed with the parents and that were implemented by the parents at home (Tang et al., 2011). The strength of evidence therefore is moderate that home programming with clinic-based care can improve gross and fine motor skills.
CareToy
A Level II study comparing use of CareToy, a smart infant gym, to standard care resulted in significant improvements for the treatment group in Infant Motor Performance (IMP) scores (d = 1.10) and nonsignificant improvements in Alberta Infant Motor Scales (AIMS) scores (d = 0.73; Sgandurra et al., 2016). A subsequent Level I RCT found large (d = 0.69), significant improvements in IMP scores in the CareToy group in comparison with the standard care group, with a nonsignificant medium effect (d = 0.33) on AIMS scores (Sgandurra et al., 2017). The strength of evidence thus is moderate that CareToy can improve motor skills in infants born preterm.
Other Interventions
Several other interventions were identified as being potentially helpful for improving motor outcomes in children younger than age 3 yr; however, limited information was available on each of these interventions. A pilot RCT comparing power wheelchair use for children ages 14–30 mo to EI alone indicated a significant improvement in the treatment group on the PEDI Functional Skills Scale (median difference between groups = 6.15) and Caregiver Assistance Scale (median difference between groups = 11.80; Jones et al., 2012). This compensatory approach improved mobility skills and decreased the need for caregiver assistance, but it did not specifically improve motor skills. Results suggest that children as young as age 14 mo can learn to operate a power wheelchair (Jones et al., 2012).
A Level II nonrandomized trial studying the impact of initiating tummy time early (before vs. after 11 wk corrected age) for infants with Down syndrome found significant differences in Bayley–III Motor scores with a large effect size (d ≥ 0.80) and a slope that declined less rapidly (p < .001; Wentz, 2017). A Level II nonrandomized pilot study of weekly swimming lessons for typically developing full-term infants in comparison with no treatment found significant improvements from pre- to posttest in AIMS scores for both groups (p < .02, Cohen’s r = .90), with no difference between groups (Dias et al., 2013). A Level III pretest–posttest study revealed significant improvements from baseline after 3–9 mo of participation in a sensory-enriched, center-based EI program in both Bayley–III Fine Motor (p = .03) and Gross Motor (p < .001) scores (Blanche et al., 2016).
In summary, the strength of evidence is low that powered mobility, tummy time, or sensory-enhanced, center-based EI can improve motor outcomes for children ages 0–3 yr. Results thus far suggest that swimming programs may not improve motor outcomes.
Interventions for Children Ages 3–5 Years
Nine studies—4 Level I RCTs, 3 Level II studies, and 2 Level III studies—provide evidence for occupational therapy interventions to address motor development in children ages 3–5 yr.
Video Game Interventions
An RCT examining the impact of a commercial, prosocial video game plus traditional rehabilitation compared with traditional rehabilitation alone resulted in significant gains for the treatment group on the Pediatric Quality of Life Inventory (p = .130, d = 0.30) and the Pediatric Outcomes Data Collection Instrument (p = .008, d = 0.25; Hsieh et al., 2016). Another RCT that investigated the impact of a low-cost virtual reality game in comparison with traditional rehabilitation found significant improvements in the treatment group on the single leg stance test (p = .017) and grip strength (right, p = .024; left, p = .043; Salem et al., 2012). A Level III pretest–posttest study that used an adaptive joystick video game found significant improvements on the Beery–Buktenica Developmental Test of Visual–Motor Integration (Beery VMI; p = .001, η2 = .45) and the Peabody Developmental Motor Scales, Second Edition (PDMS–2) Total Motor Quotient (p = .012, η2 = .29), Gross Motor Quotient (GMQ; p = .013, η2 = .28), and Fine Motor Quotient (p = .003, η2 = .37; Hsieh et al., 2015). Therefore, the strength of evidence is strong that video games can improve gross motor outcomes for children ages 3–5 yr.
Preschool Programs Targeting Fine Motor and Visual–Motor Skills
In an RCT, children who received a fine motor intervention (including one-on-one and consultative occupational therapy services) had significant improvements in comparison with standard care control participants on the Beery VMI (p = .009, d = 0.34) and the Bruininks–Oseretsky Test of Motor Proficiency, Second Edition (BOT–2), Manual Coordination subscale (p = .023, d = 0.24; Ohl et al., 2013). In a Level II nonrandomized study, children who received the Handwriting Without Tears–Get Set for School (HWT–GSS) program improved on the HWT–GSS Check Readiness tool (p = .022, d = 0.86) and the BOT–2 Fine Motor Control (p = .170, d = 0.89), Precision (p = .045, d = 0.74), and Integration subtests (p = .21, d = 0.87) in comparison with a standard care group (Lust & Donica, 2011). Finally, a Level II nonrandomized study of a magnifier training program in comparison with basic fine motor sessions without a magnifier for children with visual impairment resulted in significant improvements on the ManuVis, a manual skills test for children with visual impairments (p = .120; Reimer et al., 2011). The strength of evidence thus is moderate that preschool programs targeting fine and visual–motor skills can improve fine motor outcomes, with mixed results for visual–motor outcomes.
Movement Breaks
An RCT comparing the Mighty Moves program to the Food Friends nutrition education program resulted in significant improvements in the Mighty Moves group on the PDMS–2 GMQ (p < .005; Bellows et al., 2013). A Level III pretest–posttest study revealed that multiple breaks for vigorous physical movement daily over 6 mo resulted in significant improvements on the 12-m run and standing long jump (Monsalves-Alvarez et al., 2015). The strength of evidence is therefore moderate that movement breaks can improve gross motor outcomes for children ages 3–5 yr.
Sensory-Based Therapy
In a Level II nonrandomized study, children with autism spectrum disorder received either a sensory-based therapy, described as sensory integration therapy, or group therapy (Iwanaga et al., 2014). The sensory-based therapy group demonstrated greater gains in the Japanese Miller Assessment for Preschoolers total (p = .005) and coordination (p = .008) scores (Iwanaga et al., 2014). Therefore, the strength of evidence is low that sensory-based therapy can improve gross motor skill outcomes for preschool-age children.
Interventions for Children With or at Risk for Cerebral Palsy
Twenty-eight studies (25 Level I [3 SRs and 22 RCTs] and 3 Level III studies) focused on motor interventions for children ages 0–5 yr with or at high risk for CP.
Early Intervention Programs
Two RCTs (Morgan et al., 2015; Morgan, Novak, et al., 2016) compared the GAME (Goals–Activity–Motor Enrichment) home-based program to standard care. Both studies found motor improvements, but only one found significant differences between the intervention and control groups on the PDMS–2 Total Motor Quotient (p = .05) and raw scores (p = .01) at 12 mo, with a large effect size over time (η2 = .20; Morgan, Novak, et al., 2016). Two RCTs examined the impact of Coping and Caring for Infants With Special Needs (COPCA), a family-centered coaching approach, compared with standard care; one found significant improvements in PEDI functional mobility scores for the COPCA group at 18 mo (p < .05; Dirks et al., 2016), whereas the other found minimal differences between groups (Blauw-Hospers et al., 2011).
An SR found that studies using child-initiated movement, task-specific training, and environmental modifications had the largest effect sizes and provided high-quality evidence (Morgan, Darrah, et al., 2016). Neurodevelopmental therapy (NDT) was the most commonly studied intervention; however, the two NDT studies that reported improvements were of low quality (Morgan, Darrah, et al., 2016).
Another SR concluded that the literature on EI for children at very high risk for CP lacked high-quality studies (Hadders-Algra et al., 2017). Limited information on sensory stimulation precluded conclusive recommendations. However, high-intensity NDT intervention was associated with significantly better outcomes than NDT intervention with a lesser frequency. One of four studies on developmental stimulation found significant improvements (Hadders-Algra et al., 2017).
In summary, there is strong evidence that early intervention programs can improve motor outcomes in young children with or at high risk for CP.
Constraint-Induced Movement Therapy and Bimanual Intensive Therapy
Constraint-induced movement therapy (CIMT) and bimanual intensive therapy (BIT) are intensive treatments that use motor learning principles to improve upper extremity function for children with unilateral CP (DeLuca et al., 2012). In an SR, Novak et al. (2013) rated CIMT and BIT as “green light” interventions. Two RCTs found that CIMT resulted in significant improvements in motor outcomes in comparison with usual care (de Brito Brandão et al., 2010; Taub et al., 2011). A multisite RCT found no differences in motor improvements between children who received 3 versus 6 hr per day of CIMT; however, both groups improved, with effect sizes ranging from η2 = .36 to .79 (DeLuca et al., 2012), and results were maintained 6 mo later (Case-Smith et al., 2012). A small Level III pretest–posttest study found that CIMT for infants resulted in significantly improved fine and gross motor scores on the Bayley–III and the Infant Motor Activity Log (Lowes et al., 2014).
Three Level I studies compared matched dosages of CIMT and BIT with a focus on motor learning principles. No significant differences in outcomes were found between these interventions (Facchin et al., 2011; Gelkop et al., 2015; Hoare et al., 2013).
In some studies, CIMT and BIT were modified for group and family-implemented models. An RCT examining CIMT in a camp setting found significant improvements in the treatment group’s motor outcomes in comparison with a usual care group (d = 0.43 on the Assisting Hand Assessment, d = 1.01 on the ABILIHAND-Kids; Aarts et al., 2010). Video observation–based analysis revealed greater improvements in capacity (d = 0.55) and performance (d = 0.65) in the intervention group that were maintained at follow-up (Aarts et al., 2011). Another RCT in which parents were trained to complete an in-home version of CIMT found significant improvements in use of the more impaired side for the treatment group compared with a wait-list control group (observed effect divided by the square root of twice the error mean square = 1.26; Eliasson et al., 2011).
An RCT found significantly improved hand function for children who received 1 hr of weekly CIMT provided by an occupational therapy practitioner plus 2 hr per day of home therapy compared with a group who received NDT (d = 1.50; Al-Oraibi & Eliasson, 2011); this finding is consistent with those of an SR by Novak et al. (2013). Another RCT found no significant difference between groups treated with intensive occupational therapy (without constraint) and with modified CIMT (Wallen et al., 2011). Finally, an RCT found no significant differences between groups treated with CIMT with and without electrical stimulation (Xu et al., 2012).
Overall, the strength of evidence is strong for traditional CIMT and BIT (administered 3–6 hr per day for 21 days using motor learning principles and encouraging use of the more affected side) to improve motor outcomes in children with unilateral CP.
Child-Focused and Context-Focused Therapies
An RCT comparing context-focused therapy (removing task and environmental barriers) to child-focused therapy (remediating impairments) over 6 mo found improvements in self-care, participation, and mobility (ds = 0.22–0.26) for both groups (Law et al., 2011). An RCT that compared child-focused, context-focused, and standard care found that self-care, mobility, and gross motor skills (p < .05) all improved significantly, with no differences between groups (Kruijsen-Terpstra et al., 2016). An RCT comparing a home program to a perceptual–motor program to address postural control in infants with CP found no interaction effect (p = .433; Harbourne et al., 2010).
These results are consistent with the findings of an SR that rated context-focused interventions as green light interventions (Novak et al., 2013). The strength of evidence for child- and context-focused therapies to improve motor skills in children with CP therefore is strong.
Hippotherapy
The results of an RCT examining the effect of hippotherapy plus conventional therapy in comparison with home-based aerobic activity for children with CP found significant increases for the hippotherapy group in scores on the 66-item and 88-item Gross Motor Function Measure (GMFM–66 and GMFM–88, respectively; Kwon et al., 2015). The strength of evidence for hippotherapy to improve gross motor function in children with CP thus is moderate.
Other Interventions
Several other interventions had only one article each supporting their use. An RCT examining the effect of wearing a TheraSuit compared with a sham suit found improved PEDI and GMFM–66 scores for both groups, with no significant differences between groups (Bailes et al., 2011). A Level III pretest–posttest study of a visual–perceptual training program found significant improvements on the Beery VMI and Pediatric Functional Independence Measure (WeeFIM) self-care, mobility, communication, and social cognition scores (all ps < .05; Milim et al., 2015).
A Level III pretest–posttest study investigating the effects of goal-directed functional therapy found significant improvements on the GMFM–66 that were maintained at follow-up (p < .001); effect sizes ranged from 1.27 to 3.36 depending on Gross Motor Function Classification System (GMFCS) level, but participants with GMFCS Level III or IV demonstrated a nonsignificant decrease at the final assessment (Löwing et al., 2010).
The strength of evidence that suit wear, visual–perceptual training, or goal-directed therapy can improve motor outcomes for children with CP thus is low. For suit wear, results thus far suggest that this intervention does not improve motor outcomes.
Discussion
The purpose of this review was to update the previous SR (Case-Smith et al., 2013) on occupational therapy interventions that address motor delays for children ages 0–5 yr and their families. The overall themes identified in both reviews were similar (i.e., interventions for children younger than age 3 yr, children ages 3–5 yr, and children with or at risk for CP ages 0–5); however, additional interventions were included in this updated review. In particular, several new intervention types emerged in the literature that address the needs of preschool-age children (e.g., video games, movement breaks, sensory-based therapy). This review did not include conductive education for children with CP and found fewer articles investigating neurodevelopmental treatment than Case-Smith et al.’s (2013) review.
The studies included in this review were mostly Level I; however, most studies had high risk of bias because of lack of blinding and selective reporting. Therefore, the results should be interpreted with caution. In addition, small sample sizes in the majority of the studies limit the ability to make confident statements about the effectiveness of the interventions across the broader population. The studies also used a variety of motor assessments; therefore, a meta-analysis was not possible. The majority of outcome measures used in the studies addressed the body functions and structures domains of the International Classification of Functioning, Disability and Health: Children and Youth Version (ICF–CY; World Health Organization, 2007).
Although some interventions in this review addressed the environment or participation in activities, few outcome measures are available to address these domains; therefore, the outcome measures used typically focused on body structures and functions. A notable exception was that several studies used the PEDI as an outcome measure. The available literature is insufficient to enable a full understanding of the link between improvements in body functions and structures and performance of and participation in activities. In addition, few studies reported long-term outcomes, so it is uncertain whether motor improvements were maintained. Thus, the ability to generalize results across outcomes and time is limited for the majority of interventions included in this review.
Note that the strength of evidence for interventions is based on evidence only for motor outcomes and only among children ages 0–5 yr and not for other potential outcomes or age groups. In the literature on interventions for children in this age range with or at high risk for CP in particular, strong evidence continues to emerge as early diagnosis becomes more accurate (Novak et al., 2017). Several articles included in this review, in particular the SRs and meta-analysis, reported outcomes across several age groups and areas of development; however, we have reported only those findings relevant to our focused research question.
Limitations
Limitations of this review include the inclusion of articles only in English and the exclusion of gray literature. In addition, this review targeted children ages 0–5 yr, but some studies included participants older than 5 yr. Finally, although clinical significance is important to consider, given the nature and breadth of this review, the focus was on the statistical significance of the interventions.
Future Directions
Future research is needed that analyzes the impact of powered mobility, tummy time, swimming programs, and sensory-enhanced, center-based EI for children ages 0–3 yr; sensory-based interventions for children ages 3–5 yr; and hippotherapy, suit wear, visual–perceptual training, and goal-directed therapy for children with CP. Studies of modified CIMT and BIT are needed to determine intervention effects, optimal dosage, and maintenance of outcomes over time. Future research should analyze components of dosing (i.e., frequency, timing, and intensity) for interventions and the impact of contextual factors such as family engagement. Outcome measures that address other domains of the ICF–CY aside from body functions and structures (i.e., activities and participation and environmental factors) should be further developed and used in future research exploring the links among these domains. Populations not well represented in this review, such as children with low-incidence diagnoses, those from low- and middle-income countries, and those historically underrepresented in research studies, should also be included in future research.
Implications for Occupational Therapy Practice
Findings from this review have the following implications for occupational therapy practice:
Occupational therapy practitioners may consider using NIDCAP, home-based parent coaching, massage, home programming, and CareToy for children younger than age 3 yr; video games, preschool programs, and movement breaks for children ages 3–5 yr; and EI, CIMT, and BIT or child- and context-focused interventions for children with CP ages 3–5 yr.
Interventions for children younger than age 3 yr should actively include parents during interventions and in home program development.
For children with CP, interventions should use components of motor learning, specifically emphasizing goal-oriented, activity-based therapy and frequent task practice.
Conclusion
Multiple interventions within the occupational therapy scope of practice have been shown to foster the development of motor skills in young children. However, the intervention types investigated in the literature vary widely, resulting in limited evidence for many of the interventions. Additional high-quality research is needed to improve the strength of evidence.
Footnotes
Acknowledgment
This systematic review was completed as part of the American Occupational Therapy Association’s Evidence-Based Practice Program.
Appendix A
*
Indicates studies that were systematically reviewed for this article.