
Abstract
Experiences during infancy and early childhood can affect social, emotional, behavioral, and psychological development. Trauma, developmental disorders, and disruptions in attachment that occur in early childhood can predispose a child for later difficulties in forming relationships, self-regulation, and managing behavior. Approximately 9.85% of babies born in the United States in 2016 were preterm (Martin et al., 2018). Preterm birth is associated with infant mortality; developmental delays; and physical, social, and mental health issues (Kiechl-Kohlendorfer et al., 2009; Martin et al., 2018). In addition, preterm infants may exhibit reduced attention and responsivity that may affect a caregiver’s ability to read and respond to their needs or to engage in typical infant–child social interactions (Ravn et al., 2011).
An estimated 45% of children experience or are exposed to at least one adverse childhood event (ACE), such as maltreatment, separation from family, violence, or substance use (Sacks & Murphey, 2018). ACE exposures are associated with cognitive and behavioral problems, maladaptive coping skills, and health risk behaviors during the developmental periods as well as into adulthood (Choi et al., 2017; Forster et al., 2017; Monnat & Chandler, 2015). In addition to preterm births and trauma exposure, approximately 7% of children in the United States live with a developmental disability (Zablotsky et al., 2017). Children with developmental disabilities are more likely to be diagnosed with a severe behavior disorder or mental health diagnosis than their typically developing peers (McIntyre, 2008). Preterm birth, early trauma exposure, and developmental disabilities can greatly influence children’s psychological, emotional, and social trajectories, often placing them at risk for mental and physical health problems throughout childhood. In addition, research has shown that caregivers’ psychological and physical health is strongly influenced by child behavior and caregiving demands (Raina et al., 2005), and a cyclical relationship exists between parental stress and attachment behavior and abuse and neglect of children (Stronach et al., 2013).
Taken together, the many early childhood mental health risk factors make it imperative to understand interventions that might support the social, emotional, and behavioral health of children and their caregivers. Infant and early childhood mental health interventions that facilitate skills for both parent and child include helping an infant or child form attachments with adults and peers, encouraging positive experiences and emotional regulation, and creating environments and supports for development and learning (Zero to Three, 2017). To maximize outcomes, parents are essential partners in supporting their child’s social–emotional development and behavioral patterns. The objective of this systematic review was to answer the following question: What is the evidence for the effectiveness of interventions within the scope of occupational therapy practice to improve mental health and positive behavior for children ages 0–5 yr and their families?
Method
The search terms and strategy were developed by an AOTA research methodologist, a medical librarian, and an advisory group. A literature search captured various interventions (e.g., motor, social, cognitive, behavioral) for children ages 0–5. Databases searched were PsycINFO, Cochrane, ERIC, MEDLINE, and OTseeker; publication dates ranged from January 2010 to March 2017. The initial search returned 89,461 results. After initial screening by the AOTA methodologist, 5,310 results were eligible for inclusion in the systematic review (Figure 1). After removal of duplicates, all three authors of this review screened the article titles and abstracts according to the inclusion and exclusion criteria; at this stage, we provided a yes, no, or maybe rating to articles screened. We then engaged in iterative discussions to review ratings, resolved discrepancies, and agreed on final yes or no ratings for articles eligible for full-text review. In-depth review of full texts was completed at this stage, and articles that did not meet the inclusion criteria were eliminated.
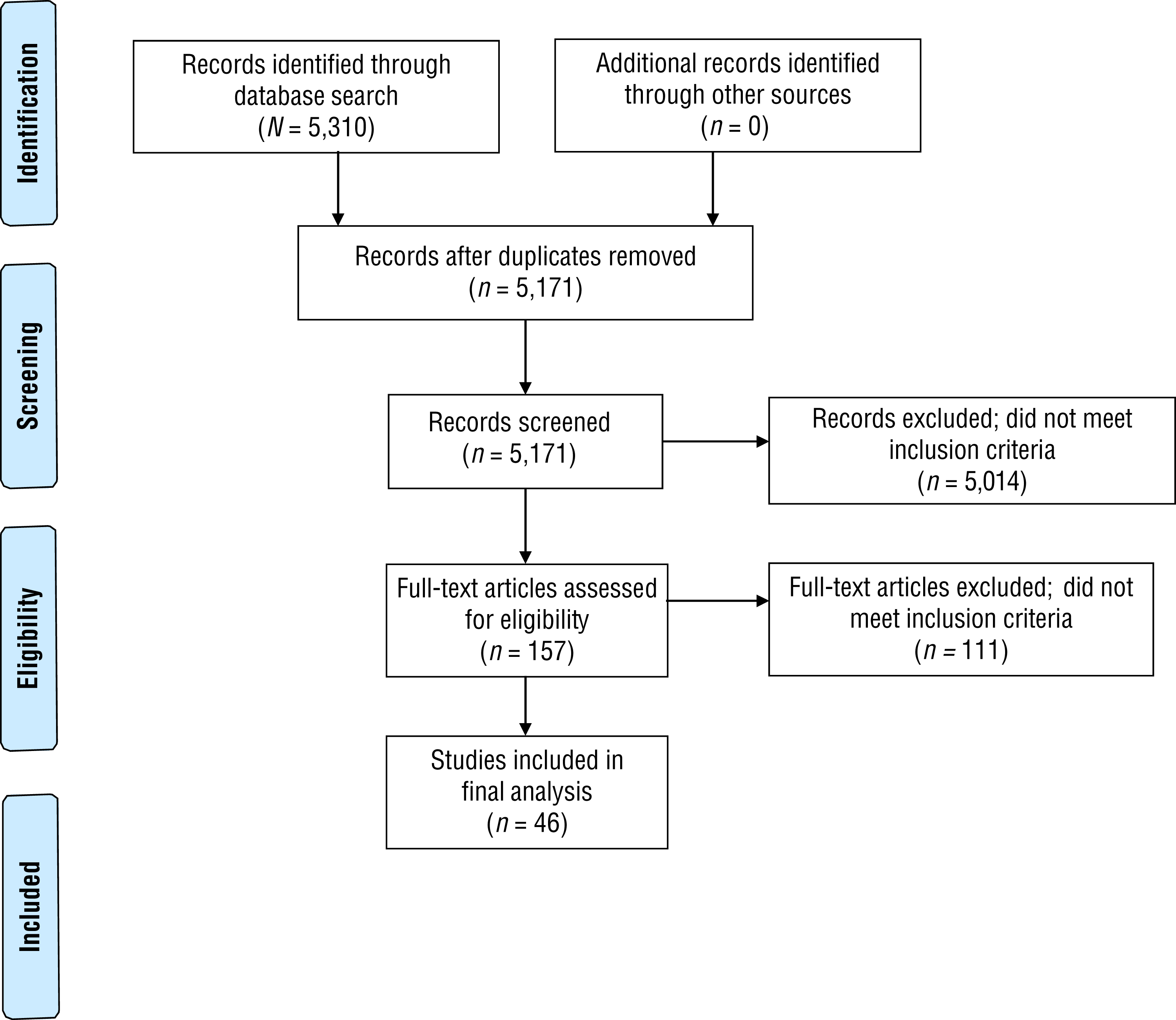
Flow diagram for inclusion and exclusion of peer-reviewed studies in the systematic review.
Study Evaluation
We critically appraised each included article by extracting study design, participants, intervention and control groups, outcome measures, and results. We assigned level-of-evidence ratings to each study using the adapted ratings from Sackett (1989), and we assessed risk of bias across studies using A Measurement Tool to Assess Systematic Reviews (AMSTAR) and Cochrane methodologies. Finally, we conducted and wrote this systematic review according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) and AOTA evidence-based practice and research guidelines for strength of evidence assignment when discussing intervention themes. The strength of evidence is rated as high (2 or more Level I studies; consistent results from well-designed and conducted studies), moderate (at least 1 Level I high-quality study or multiple moderate-quality studies; evidence is sufficient but constrained by moderate methodological limitations and inconsistency of findings), or low (small number of low-level studies; significant methodological limitations and inconsistency in findings).
Inclusion and Exclusion Criteria
To be included, articles were required to published in English in a peer-reviewed journal between January 2010 and March 2017, to include participants ages 0–5 yr, to examine interventions within the scope of occupational therapy, to include a mental health (e.g., anxiety, stress) or positive behavior (e.g., decreased aggression, social skills) outcome, and to provide Level I, II, or III evidence. We excluded articles that were dissertations, theses, presentations, or proceedings; that were published before 2010; that provided Level IV or V evidence; that focused only on adults (e.g., parental stress without any child outcome); that examined interventions that occupational therapy practitioners are not able to deliver; that included participants whose average age was >5 yr; that described interventions delivered in a kindergarten or primary school setting; and that were review articles in which participant age ranges were unclear.
Results
Forty-six studies were included in this systematic review (31 Level I, 8 Level II, and 7 Level III; Tables A.1–A.3 in Appendix A). Thematic analysis resulted in the following themes: touch-based interventions, parent–child interaction therapy (PCIT), and instruction-based interventions.
Touch-Based Interventions
Nine studies examined skin-to-skin contact, kangaroo care (KC), or massage: 5 Level I studies with low to high risk of bias and 2 Level II and 2 Level III studies with high risk of bias. Five studies examined skin-to-skin contact or KC, and 4 studies explored the effectiveness of infant massage.
Skin-to-skin contact and KC provide direct contact between the infant’s and caregiver’s skin. Included studies measured a variety of outcomes, including indicators of physiological stability and parent and infant mental and behavioral health. Overall, moderate strength of evidence supports the use of skin-to-skin contact and KC to address maternal stress, anxiety, and attachment. Low strength of evidence addresses skin-to-skin contact and KC to address maternal depression.
The use of lullaby music during KC sessions had a significant and large effect on decreasing maternal anxiety in a randomized controlled trial (RCT) conducted by Lai et al. (2006). Level II studies supported the use of skin-to-skin contact and KC interventions to increase maternal–infant attachment and to decrease maternal anxiety but had few or no significant effects on maternal depression (Ahn et al., 2010; Feldman et al., 2014). In addition, a Level III study found a significant increase in maternal–infant attachment and reduction in maternal stress after three 30-min sessions of KC per week (Cho et al., 2016). Although the majority of studies focused on KC delivered by the mother, a study of KC from fathers found no significant difference in physiology or stress in the infants (Srinath et al., 2016).
Regarding massage, strong evidence supports its use to increase infant self-regulation, moderate-strength evidence supports its use in reducing parental stress and improving social behavior, and low-strength evidence supports its use to decrease maternal depression. Four Level I studies (2 systematic reviews with low risk of bias and 2 RCTs with moderate risk of bias) examined specific massage techniques including manualized protocols designed by study authors, Baby’s First Massage, and qigong massage. Three studies found both statistically and clinically significant improvements on measures of infant self-regulation (Bennett et al., 2013; Juneau et al., 2015; Silva et al., 2011). The 2 systematic reviews also found improvements in social behavior and engagement in preterm and term infants (Bennett et al., 2013; Juneau et al., 2015). In addition, the 2 RCTs found that caregivers providing massage to their infants reduced parental stress with significant effect sizes (Oswalt & Biasini, 2011; Silva et al., 2011). Last, among mothers with HIV infection, providing Baby’s First Massage to their infants reduced depression level with a large effect size (Oswalt & Biasini, 2011).
Parent–Child Interaction Therapy
PCIT is a manualized intervention that provides specific training to parents in how to interact with their child to support positive behaviors. The intervention includes two phases: child-directed interaction and parent-directed interaction. Four studies (2 Level I, 1 Level II, 1 Level III) examined the effectiveness of PCIT. All studies had high risk of bias because of lack of randomization, use of convenience samples, and high attrition rates. Outcomes of the studies included child behavior, parenting behaviors, and parental stress.
Moderate evidence supports the use of PCIT to improve child behavior. Several studies found that PCIT had a significant effect with large effect sizes on child behavior, including reducing externalized and challenging behaviors (Bagner et al., 2016; Fung et al., 2014; Rodríguez et al., 2014; Ros et al., 2016). Low-strength evidence addresses PCIT targeting parenting behavior; 1 Level II study (Bagner et al., 2016) and 1 Level III study (Fung et al., 2014) found significant improvements in positive parenting behaviors, reductions in negative parenting behaviors, and improvements in parental discipline behavior.
Low-strength evidence with mixed results addresses PCIT’s effects on parental stress. Bagner et al. (2016) found no significant effects on parental stress, but Ros et al. (2016) found that parents who completed more homework assignments from their PCIT program experienced decreased stress.
Instruction-Based Interventions
A total of 33 studies examined instruction-based interventions including parent training, group-based parent training, teacher (prekindergarten) training, and parent training for child sleep. The 33 studies included 26 Level I studies (5 systematic reviews, 21 RCTs), 4 Level II studies, and 3 Level III studies with low to high risk of bias.
Parent Training
Twenty studies (16 Level I, 2 Level II, 2 Level III) with low to moderate risk of bias examined parent coaching, consultative counseling, and structured parent training administered in the home, clinic, and hospital. These studies addressed the outcomes of parenting behavior, child behavior, parent mental health, child mental health, and maternal–infant attachment.
Parenting Behavior.
Strong evidence from 9 studies supports parent training interventions to improve parenting behavior. Six Level I studies, 1 Level II study, and 2 Level III studies with moderate risk of bias found significant changes in parenting skills with large effect sizes.
A parent training program, Incredible Years (IY), educates and guides parents in developing parenting skills to address their child’s social, emotional, academic, and behavioral needs. Two studies of IY found significant improvements in parenting skills, including positive parenting strategies and discipline consistency, and improved compliance after 10 weekly sessions (McMenamy et al., 2011, Level III; Perrin et al., 2014, Level I).
Two RCTs examined parent training groups. Solomon et al. (2014) used home consultation and training, 3 hr/mo for 12 mo, for parents of children with autism spectrum disorder, and Wu et al. (2014) evaluated clinic- and home-based training for parents of preterm infants that focused on parent–child interactions and infant behavior. Both studies demonstrated significant improvements in parent responsiveness and didactic interactive behavior.
An RCT by Kierfeld et al. (2013) found significant improvements in managing internalizing and externalizing behaviors after an 11-wk parent training program using a self-help book and weekly phone meetings. In a Level II study, Kusanagi et al. (2011) used a parent coaching program for two groups of mother–infant dyads and found that the mild intervention group made more significant and overall improvements than the intensive intervention group.
Child Behavior.
Low-strength evidence from 12 studies (9 Level I, 3 Level III) with mixed findings and moderate risk of bias addresses the effect of parent training on child behavior. Five studies found significant effects on child behavior outcomes after parent-training interventions ranging from a self-help book to more structured training programs. In 2 RCTs, providing parents with a self-help book and weekly consultative meetings resulted in significant improvement in their children’s internalizing and externalizing behaviors with large effect sizes (Ise et al., 2015; Kierfeld et al., 2013). Six studies found that parent training programs, such as individual Early Social Interaction, modified Mother–Infant Transaction Program (MITP), and IY, demonstrated significant improvements in child behavior outcomes, including fewer behavior problems, decreased child aggression, improved compliance, and improved social communication and socialization (Lakes et al., 2011; McMenamy et al., 2011; Michelson et al., 2013; Nordhov et al., 2012; Smith et al., 2015; Wetherby et al., 2014).
Four Level I studies found no significant difference between intervention and control groups or inconsistent results for child behavior (Homem et al., 2014; Oono et al., 2013; Spieker et al., 2012; Wu et al., 2014). A Cochrane systematic review from 2013 found no significant evidence of gains for child behavior from parent-mediated approaches because of inconclusive evidence and inconsistencies across studies (Oono et al., 2013). An RCT examining the IY program found no significant differences in children’s social skills or aggressive and oppositional behavior after 14 120-min hospital-based parent training sessions (Homem et al., 2014). Another RCT evaluating the Promoting First Relationships program found significant group differences with medium effect sizes for child competence behavior (Spieker et al., 2012). Finally, an RCT of a clinic-based program for child–parent dyads resulted in no significant effects at 12 mo; however, lower rates of child internalizing behavior were found after 24 mo (Wu et al., 2014).
Parent Mental Health.
Moderate evidence from 3 studies (2 Level I, 1 Level II) with moderate risk of bias supports parent training to improve parent mental health (Akbarzadeh et al., 2016, Level I; Komoto et al., 2015, Level II; Solomon et al., 2014, Level I). In an RCT, Akbarzadeh et al. (2016) provided 60- to 90-min education sessions on attachment behaviors to expectant mothers, which resulted in significantly decreased anxiety compared with a control group. Solomon et al. (2014) conducted an RCT of a home-based parent training program and found that parents who received the intervention were significantly less likely to be depressed. A Level II study with a high risk of bias found that a clinic-based, mother–infant training session resulted in decreased parent-related stress with a moderate effect size (Komoto et al., 2015).
Child Mental Health.
Low-strength evidence from 2 studies with a moderate risk of bias addresses the use of parent training to improve child mental health (Komoto et al., 2015, Level II; Ravn et al., 2011, Level I). Ravn et al. (2011) found significant improvements in child mental health outcomes, including improved mood and decreased child-related stress and anxiety, after 11 1-hr parenting training sessions using an MITP model. In contrast, a clinic-based mother–child attachment training intervention resulted in no significant differences for child-related stress (Komoto et al., 2015).
Maternal–Infant Attachment.
Strong evidence from 6 studies (5 Level I, 1 Level II) with low risk of bias supports parent training to promote maternal–infant attachment. A systematic review found that parenting education focused on cue-based, responsive care with an average dosage of 7.5–10.0 hr over 8 wk improved the quality of the relationship with large effect sizes (Evans et al., 2014). A clinic-based mother–infant training intervention resulted in significant improvements in sensitivity to cues, response to child distress, and social–emotional growth (Komoto et al., 2015, Level II). An RCT examining the home-based Infant Behavioral Assessment and Intervention Program, which is focused on improving preterm infants’ self-regulation and development, found improved maternal sensitivity in interaction with preterm infants and no effect on the infants (Meijssen et al., 2010).
An RCT by Ravn et al. (2011) examined an MITP focused on facilitating first-time mothers’ understanding of their preterm baby’s characteristics and development and on fostering improved awareness and responsiveness to infant cues to establish positive interactions and enjoyment in 11 8-hr sessions. Significant improvements were found in maternal sensitivity and responsiveness and infant positive mood, which contributed to improved mother–infant interactions. Another RCT examined a parent training intervention that included 60-min in-home weekly sessions over 10 wk; the only significant caregiver outcome was improved sensitivity, with a medium effect size (Spieker et al., 2012). Finally, Kynø et al. (2012) found no significant group differences in an RCT investigating a semistructured MITP consisting of 11 60-min educational sessions.
Group-Based Parent Training
Low-strength evidence from 5 studies (4 Level I, 1 Level II) with moderate risk of bias addresses group-based parent training interventions, including facilitated and self-directed parenting groups (Barlow et al., 2016; Elizur et al., 2017; Finch et al., 2016; Herbert et al., 2013; Keen et al., 2010). A systematic review found that group-based parent training reduced emotional and behavioral problems in children ages 0–3 yr; however, findings were based on low-quality evidence, and the authors recommended using these interventions with caution (Barlow et al., 2016). An RCT by Finch et al. (2016) found that a group-based parenting intervention had a significant effect on child cognitive skills at age 4 yr, whereas a Level I study by Elizur et al. (2017) found that a group-based intervention mediated treatment effects on both effortful control and callous–unemotional behavioral traits.
The Parenting Your Hyperactive Preschooler Program, a group-based program that teaches parents behavioral techniques and socialization strategies, was associated with significantly decreased disruptive and hyperactivity–impulsivity behaviors, yet it had high performance and detection bias (Herbert et al., 2013). Finally, Keen et al. (2010) found no significant differences between facilitated and self-directed parent training groups regarding parenting sense of competence or parent-related stress; however, the self-directed group reported significantly decreased child-related stress.
Teacher (Prekindergarten) Training
Moderate-strength evidence from 5 studies (3 Level I, 1 Level II, 1 Level III) with moderate risk of bias examined teacher training to improve mental health and positive behavior for children ages 0–5 yr (Pears et al., 2015, Level I; Stanton-Chapman et al., 2016, Level III; Ştefan & Miclea, 2012, Level II; Strain & Bovey, 2011, Level I; Vancraeyveldt et al., 2015, Level I). Two RCTs on training focused on individual teacher–child interactions in the classroom (e.g., conflict resolution, functional skills development, social interaction, adaptive behavior) found significant improvements in child behaviors with moderate to high effect sizes (Strain & Bovey, 2011; Vancraeyveldt et al., 2015). An RCT of a school readiness program that collaborated with children and their families to promote self-regulation skills and parental involvement at school found significant reductions in ineffective parenting and improvements in parental involvement (Pears et al., 2015). Two smaller studies examined teacher training workshops and coaching sessions focused on positive behavioral supports and social–emotional competencies, typically 60–90 min for up to 10 sessions; both found significant improvements in positive child behavior and reductions in aggression and noninteractive play (Stanton-Chapman et al., 2016; Ştefan & Miclea, 2012).
Parent Training for Child Sleep
Low-strength evidence from 2 Level I studies with mixed results and low risk of bias addressed parent training interventions for child sleep (Douglas & Hill, 2013; Gradisar et al., 2016). In an RCT by Gradisar et al. (2016), two intervention groups demonstrated a significant improvement in sleep latency; no significant differences between groups were found in maternal mood or infant stress, but the graduated extinction group, which involved placing an infant for sleep and returning at gradually longer intervals, had significantly lower cortisol levels at 1-mo follow-up. A systematic review by Douglas and Hill (2013) found that behavioral interventions for sleep in infants younger than 6 mo old were not effective in decreasing infant crying, preventing sleep and behavioral problems in later childhood, or protecting against maternal postnatal depression.
Discussion
The purpose of this systematic review was to examine the current evidence for interventions within the scope of occupational therapy that address mental health and positive behavior for children ages 0–5 yr and their families. Infancy and early childhood experiences are critical to brain development and provide a foundation for healthy attachment and positive mental health. The mental health of young children continues to gain attention as emerging research highlights the effects that attachment and trauma can have on the developing brain, including cortical structural differences associated with behavioral and regulation difficulties in young children. In addition, an infant’s or child’s social, behavioral, and emotional functioning can affect parental stress and well-being. Thus, caregivers are essential in supporting infants’ and young children’s mental health and positive behavior, and many are in need of assistance themselves.
The results of this review reflect these issues and explore important interventions that may support mental health and positive behavior in children and parents. All interventions included in this review were considered within the scope of occupational therapy, which means that occupational therapy practitioners either currently possess the requisite skills to administer the interventions or qualify to complete specific training to administer them. However, none of the studies explicitly included an occupational therapy practitioner as an interventionist.
Strong evidence supports the use of touch-based interventions to support infant self-regulation; evidence for their effectiveness in improving maternal stress and anxiety, social behavior, and attachment is of moderate strength. Low-strength evidence addresses their role in reducing maternal depression. Although the majority of evidence focuses on KC administered by the infant’s mother, fathers should also be encouraged to participate in skin-to-skin contact to improve attachment and decrease parental stress and anxiety. In addition, the use of lullaby music during KC sessions may help decrease maternal anxiety. Manualized massage protocols, such as Baby’s First Massage and qigong massage, can improve infant self-regulation and may also reduce parental stress and improve the child’s social behavior. Occupational therapy practitioners should provide touch-based interventions, including skin-to-skin, KC, and infant massage, to parents of children ages 0–5 yr with or at risk for mental health concerns.
Moderate-strength evidence supports PCIT to address child mental health and positive behavior. Occupational therapy practitioners should use PCIT to improve positive behavior in young children by reducing externalized and challenging behaviors; however, additional high-quality studies are needed to support the effectiveness of PCIT in improving positive parenting behaviors and decreasing parental stress.
A wide variety of instruction-based interventions are addressed in the literature. Strong evidence supports parent training to improve parenting behavior and maternal–infant attachment, and moderate-strength evidence supports its use to improve parent mental health; the evidence for its use to improve child behavior and child mental health is of low strength. Occupational therapy practitioners can use a variety of parent training models, such as parent coaching, consultative counseling, and structured parent training protocols, administered in weekly sessions in the home, clinic, or hospital setting or over the phone. For example, the IY program can be administered in 10 weekly sessions to improve positive parenting strategies and consistent discipline. Parent training interventions can also be used to improve parent mental health; educational sessions on attachment behaviors lasting 60–90 min can be used with expectant mothers to decrease maternal anxiety, and a home-based parent training program can be used to decrease parental depression.
Occupational therapy practitioners should use parent training, especially with first-time mothers, to promote maternal–infant attachment, including sensitivity to the infant’s cues, response to the infant’s distress, and understanding of social–emotional growth. It is unclear what dosage of parent training provides optimal efficacy for maternal–infant attachment; protocols ranged from 60 min to 8 hr per session over an average of 10 wk. Because of limited or conflicting findings, the evidence addressing the use of parent training intervention to influence child mental health, behavior, or sleep in infants younger than 6 mo old is of low strength.
The evidence for instruction-based interventions to improve child mental health and positive behavior is of low strength for group-based parent training, of moderate strength for teacher training, and of low strength for sleep training. Group-based parent training to promote mental health and positive behavior in early childhood should be implemented with caution because of methodological flaws in the current evidence. Teacher (prekindergarten) training focused specifically on individual teacher–child interactions in the classroom can be used to improve child behaviors. Moreover, teacher training interventions in which teachers collaborate with the child and family to promote self-regulation skills and parental involvement at school can be used to improve parenting behavior and involvement. Occupational therapy practitioners should consider conducting teacher training workshops and coaching sessions to improve child behavior in the school environment.
Limitations
Many studies relied heavily on self-report measures of child behavior, child mental health, and parent mental health. In many studies, caregivers were aware of their treatment condition when reporting. Additional well-controlled trials are needed that include systematic randomization, objective measures, and blinding of participants and personnel to reduce the risk of bias seen in many studies in this review. Studies are needed that include interventions designed specifically for occupational therapy practice or delivered by occupational therapy practitioners to increase their applicability to occupational therapy.
This review includes analysis and discussion only of studies that examined interventions within the scope of occupational therapy for children ages 0–5 yr that included a mental health or positive behavior outcome. In addition, only studies providing Level I, II, and III evidence were included because of their greater rigor and ability to control for confounding variables. These restrictions may have resulted in the exclusion of studies of other valuable interventions that were conducted in less controlled settings or with more variable populations; thus, other effective interventions to improve child and parent mental health may not have been included, and the applications of the review may be limited.
Implications for Occupational Therapy Practice
The results of this systematic review have the following implications for occupational therapy practice:
• Practitioners should coach caregivers to use massage to increase infant self-regulation, reduce parental stress, and improve child social behavior.
• KC or skin-to-skin contact should be used to address maternal stress, anxiety, and attachment.
• PCIT should be considered only to address child behavior.
• Practitioners should implement individualized parent or teacher training to promote child mental health and positive behavior.
• Occupational therapy educational programs should train practitioners to incorporate parent-mediated intervention to promote infants’ and young children’s positive mental health.
Conclusion
A variety of interventions within the scope of occupational therapy practice support the mental health and well-being of children and caregivers who may exhibit symptoms of or risk factors for social, emotional, or behavioral difficulties. Many of these interventions are taught to caregivers and teachers to promote positive mental health and behavior in the child, and others are focused on fostering personal connection and positive interaction between the adult and child. Individualized training given to parents and teachers appears to be the most effective way to engage these caregivers and produce positive results.
Footnotes
Acknowledgments
This systematic review was completed as part of the American Occupational Therapy Association’s Evidence-Based Practice Program.
Appendix
*
Indicates studies that were systematically reviewed for this article.