
Abstract
For many people with attention deficit hyperactivity disorder (ADHD), interactions with peers can be challenging. Approximately 6.1 million children ages 2–17 yr in the United States have a diagnosis of ADHD (Centers for Disease Control and Prevention, 2018). According to the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; American Psychiatric Association [APA], 2013), ADHD is defined as a pattern of inattention, hyperactivity, or both (i.e., combined). Inattention can lead to difficulty with maintaining attention to tasks, difficulty organizing and planning activities, and ease of becoming distracted (APA, 2013). Hyperactivity is evident in problems such as fidgeting, leaving the classroom at inappropriate times, having difficulty waiting for one’s turn, and interrupting others. Because of these issues with attention and hyperactivity, children with ADHD are aversive to peers and have lower social skills necessary for engagement in social participation than do typically developing (TD) peers (Mikami, 2010; Mrug et al., 2012; Waschbusch, 2002; Young & Amarasinghe, 2010).
Social Skills Deficits in Children With Attention Deficit Hyperactivity Disorder
Social skills are the competencies people use to communicate, learn, get needs met in appropriate ways, get along with others, make friends, develop healthy relationships, protect themselves, and interact with society (Dowd & Tierney, 2017). Social dysfunction is a common characteristic among children with ADHD (Hoza et al., 2005). Hodgens et al. (2000) found that children with hyperactive or inattentive forms of ADHD can experience peer rejection in as little as a few hours after meeting a new peer. Negative social behaviors can vary depending on the subtype of ADHD. Children with hyperactive or combined ADHD more frequently demonstrate impulsive actions and aggressive characteristics that are sources of annoyance to their peers. Children with the inattentive type of ADHD display socially withdrawn behaviors and often make inappropriate social statements because of lack of awareness of the feelings of others or difficulty managing their own emotions (Hodgens et al., 2000).
Impact of Social Skills Deficits
The symptoms and social characteristics associated with ADHD often result in social dysfunction and lead to peer rejection and less meaningful friendships (Mrug et al., 2012). Children with ADHD were found to be twice as likely as TD children to have no friends (Hoza et al., 2005); of those who reported having friends, 56% of those friends did not consider these children to be their friends. Even when children with ADHD have friends, the friendships tend to be of lower quality and less stable than those of their TD peers (Hoza et al., 2005) and to last a shorter time than friendships of TD children (Normand et al., 2011).
Social dysfunction, peer rejection, and poor friendship quality can persist over time if not resolved. Constant social difficulties and peer rejection have been associated with adverse outcomes later in life (Mrug et al., 2012). In an 8-yr follow-up of children with ADHD, Mrug et al. (2012) found that symptoms of ADHD were correlated with higher levels of substance abuse and depressive symptoms. Peer rejection was positively associated with delinquency, smoking, anxiety, and social impairment, whereas friendship was associated with lower delinquency and lower depressive symptoms.
Need for Peer Involvement
Because problems with peer relationships are likely a causal factor in persistent long-term impairments, approaches that address peer relationships are important (Mrug et al., 2012). Of the currently accepted interventions targeted at social skills improvement, those involving TD peers in treatment have been shown to result in improved generalization (Ang & Hughes, 2002; DuPaul & Weyandt, 2006). This outcome was especially true when the same peers engaged in social interactions outside of treatment sessions in an environment where practice, corrections, and reinforcement could occur organically (Ang & Hughes, 2002; DuPaul & Weyandt, 2006). Incorporation of peers in parent training interventions also has demonstrated the potential to improve positive social behaviors and friendship development (Antshel, 2015).
Few studies examining the use of peers during interventions have been published, and no systematic review has been conducted to evaluate the available literature. A systematic review is warranted to clarify the effectiveness of peer inclusion during social interventions for children with ADHD. The objective of this systematic review, therefore, was to evaluate whether social skills interventions incorporating peers are effective in improving social skills in children with ADHD. The knowledge gained from the studies included in this review can be implemented in practice to improve social participation in children with ADHD while reducing peer rejection and the negative long-term outcomes resulting from social dysfunction.
Method
Search Strategy
Intervention studies from peer-reviewed journals were selected for this systematic review on the basis of a topic and search protocol agreed on by members of the research team (the authors). Databases searched were CINAHL, PubMed, Web of Science, Google Scholar, and PsycINFO. Other sources included to ensure a comprehensive search of the literature were reference lists from published literature and hand searches of electronic journals. The aim of our review was to examine the effects of social skills interventions for children with ADHD that included some type of interaction with peers and outcome measures within the domain of occupational therapy.
Selection Criteria
To meet inclusion criteria, studies had to have participants younger than age 18 yr with any ADHD pattern, provide a social skills training intervention with peer involvement, use outcome measures within the domain of occupational therapy, and be published in English. Studies needed to use a peer as the sole or primary component at some point in the social skills intervention (search terms are listed in Table 1). Peers were defined as TD children, children with ADHD, playmates, schoolmates, or siblings who were similar in age to the children with ADHD. Initially, only publications in the past 10 yr were included, yielding 10 articles, so search criteria were expanded to the past 20 yr to provide more comprehensive coverage of the available literature, yielding 15 articles. All review databases, including the Cochrane database, were screened for systematic reviews on social skills interventions for children with ADHD that included peers to ensure that the systematic review had not already been completed.
Key Search Terms
Note. ADHD = attention deficit hyperactivity disorder.
Studies that addressed adults with ADHD and articles written in a language other than English were excluded. Additionally, studies that used participants with comorbidities or multiple conditions, such as autism spectrum disorder and conduct disorder, were excluded to prevent characteristics that were not consistent with ADHD diagnoses from affecting the results of the interventions.
Procedure
Each member of the research team performed comprehensive searches and screened the results on the basis of the inclusion criteria. From there, the team, with the guidance of additional experienced researchers, discussed and analyzed the full-text articles to determine which studies to include in this systematic review. Each article was reviewed by at least two team members to ensure accuracy of data. Disagreements were addressed by involving the rest of the research team and outside researchers until a consensus was reached (for a diagram of the flow of articles through the selection process, see Figure 1). Finally, the data were compiled into an evidence table (Table A.1 in Appendix A) and classified by level of evidence on the basis of the American Occupational Therapy Association’s (2017) Guidelines for Systematic Reviews, which are based on Sackett (1989).
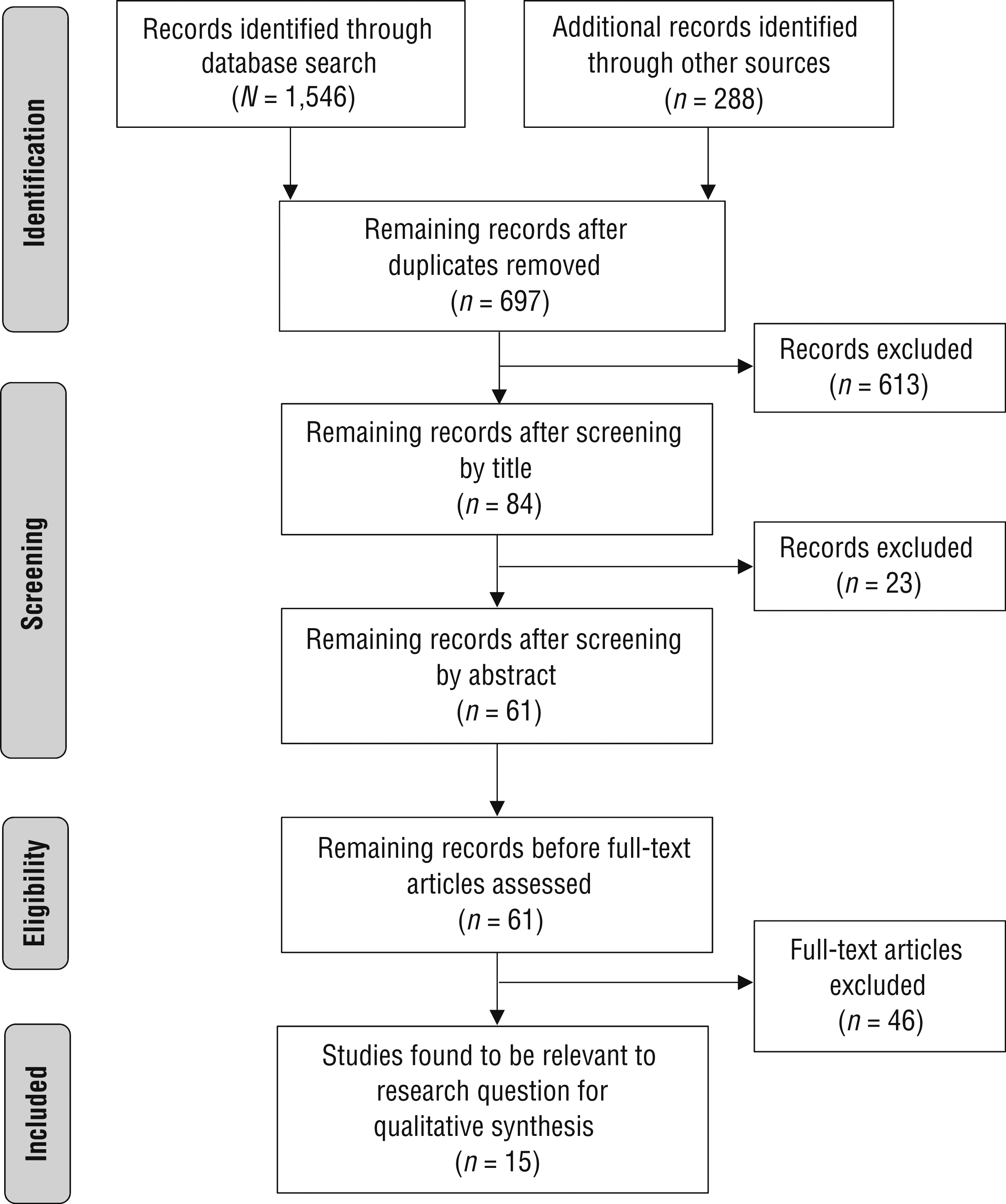
Flow diagram for inclusion and exclusion of peer-reviewed studies in the systematic review.
Results
Fifteen studies met the inclusion criteria (1 Level I study, 1 Level II study, 10 Level III studies, and 3 Level IV studies). Intervention methods were categorized as incorporating either peers with ADHD or peers without ADHD. The methods incorporating peers without ADHD were subcategorized as play-based and school-based interventions. Study participants ranged in age from 5 to 16 yr, with most being between ages 5 and 11 yr. The participants with ADHD were predominantly male, which is reflective of the population of children with an ADHD diagnosis. In the case of peers, more equal numbers of male and female peers were common, and some samples had more girls. Dosage for the interventions ranged from one to five times per week, for 20 min to 9 hr in each session, over 12 days to 15 wk.
Interventions were evaluated individually to see how they affected social skills in children with ADHD. Eleven studies produced statistically significant improvement in social skills with peer involvement, whereas four studies did not. Table 2 lists the methods, peer roles, and settings used for the interventions.
Components of the Interventions Used in the 15 Studies in This Systematic Review
Risk of Bias
We used Higgins et al.’s (2011) methods to assess for risk of five types of bias: selection bias, performance bias, detection bias, attrition bias, and reporting bias (Table A.2). Blinding of outcome assessment for objective outcomes occurred in 7 of the 15 studies reviewed. Six studies had high risk for attrition bias because of incomplete outcome data. None of the studies had high risk of selective reporting bias. Avoiding most of these types of bias is often impractical and problematic in studies with Level II–IV designs. In spite of these risks, we deemed the findings useful and valuable to inform the use of interventions to support the social skills development of children with ADHD. Several researchers participated in multiple studies included in this systematic review, although different participants were included in each of the studies.
Interventions Incorporating Peers Without Attention Deficit Hyperactivity Disorder
Of the 15 articles, 11 involved interventions incorporating peers without ADHD. We classified these studies into two subcategories: play-based interventions and school-based interventions.
Play-Based Interventions
Evidence from eight studies supports play-based interventions incorporating peers without ADHD. In a Level I study, Wilkes-Gillan, Bundy, Cordier, Lincoln, and Chen (2016) used an intervention-first group and a control-first group to evaluate a 10-wk play-based program. Children with ADHD were paired with a TD peer playmate and participated in sessions involving video feedback, discussion of social skills, cooperative play, and therapist modeling. Parents joined video feedback sessions, participated in discussions with their children, observed play sessions, received training, and delivered home modules weekly. Parents also facilitated four 40-min play sessions in their homes between a TD playmate and their child with ADHD. The change in the overall play skills of the intervention-first group after the intervention phase was significantly greater than the change in the overall play skills of the control-first group, t(14) = 8.02, p < .001. Test of Playfulness (Bundy, 2004) scores on play skills items improved significantly from pre- to postintervention and from preintervention to 1-mo follow-up in the intervention-first group (p < .001). Social items scores revealed significant improvement from pre- to postintervention and from preintervention to 1-mo follow-up (p < .001) but no significant difference from postintervention to 1-mo follow-up (p > .05).
Barnes et al. (2017) conducted a Level III study using a play-based intervention involving both home and clinic settings for children with ADHD, TD peer playmates, and the children’s parents. Video recordings, parent surveys (Parenting Relationship Questionnaire, Kamphaus & Reynolds, 2006; Social Skills Improvement System, Gresham & Elliott, 2008), and direct observation were used to evaluate play. Improvement in social play skills was sustained in the home environment but not in the clinical environment, as demonstrated by an increasing trend with a medium effect size (d = 0.68, p = .36). Parents reported continued use of the activities after the initial intervention, which may have influenced maintenance of improvement demonstrated by the follow-up scores.
Wilkes-Gillan, Bundy, Cordier, and Lincoln (2016) conducted a Level III study of a 7-wk, parent-delivered, play-based intervention for children with ADHD and TD peer playmates. Parents received 1 hr of training, administered home modules to promote social interactions, and provided feedback to their children before, during, and after facilitated playdates. Parents observed and discussed three clinic sessions of therapist-supported free play and promotion of prosocial behaviors. Social play skills of children with ADHD significantly improved from pre- to postintervention (p = .03) and 1-mo follow-up (p = .02). Additionally, social play skills of TD playmates significantly improved from pre- to postintervention (p = .02). The long-term effectiveness of the study was evaluated in a Level III 18-mo follow-up study by Cantrill et al. (2015). Semistructured interviews with parents and play observations revealed that play skills for both children with ADHD and TD playmates improved, but not significantly, from postintervention to 18-mo follow-up, demonstrating maintenance of skills (p = .07).
Three Level III studies used a 7-wk, play-based intervention program in which a TD peer playmate of similar age was paired with a child with ADHD (Cordier et al., 2013; Docking et al., 2013; Wilkes et al., 2011). The intervention occurred in 40-min sessions once a week in a playroom and included video feedback–feedforward and modeled play by the therapist, peer, and child, while parents received training and education on social skills through play. Significant improvements in play were found for both children with ADHD and their TD playmates (p < .01), and all children with ADHD significantly improved their play skills (p < .01), whether they had language difficulty (p = .002) or not (p = .007; Docking et al., 2013; Wilkes et al., 2011). Cordier et al. (2013) discovered significantly improved mean overall posttest scores for pragmatic language on two outcome measures (Pragmatic Protocol, p = .006; Structured Multidimensional Assessment Profiles, p = .001). However, Docking et al. (2013) reported that communication and pragmatic language abilities of children with ADHD did not significantly improve over the course of the intervention (p = .528).
A Level III study by Wilkes-Gillan et al. (2014) investigated the effects of the 7-wk, play-based intervention performed by Wilkes et al. (2011) at 18-mo follow-up through parent interviews and a 30-min clinic play session with a TD peer playmate. The children with ADHD maintained their gains 18 mo after the intervention.
School-Based Interventions
Evidence from 3 Level IV studies supports school-based interventions incorporating peers without ADHD. Davies and Witte (2000) examined the effect of a self-monitoring and group contingency approach to address inappropriate verbalizations in the classroom. Peers played the roles of collaborative partner, class member, and behavior monitor. The intervention was implemented in a third-grade classroom for 30-min sessions in two intervention periods. Ten students were removed from the group, and the children with ADHD were rematched with TD students. Baseline assessments were completed before each intervention period. At the initial baseline assessment, the children with ADHD made significantly more inappropriate verbalizations (p < .05) than their TD peers. At the second baseline assessment, the difference was no longer significant, indicating that the peer intervention had equalized the number of inappropriate verbalizations by both groups.
Plumer and Stoner (2005) used the Classwide Peer Tutoring (CWPT) approach and peer coaching to improve positive social behaviors of 2 fourth-grade children and 1 third-grade child with ADHD. CWPT is a teaching strategy that may be applied with an entire class of students. In this study, CWPT was implemented using student pairs who alternated between the roles of tutor and tutee during spelling practice. A point-reward system of reinforcement was used to reward good performance, and in-the-moment error correction was provided. For the children with ADHD, peers played the roles of tutor, behavior coach, and behavior monitor. An intervention stage that used only CWPT was implemented for 20–25 min 3 days/wk for approximately 10 wk. Students reviewed goals each day and assigned performance ratings for each. The Peer Social Behavior Code of the Systematic Screening for Behavior Disorders (Walker & Severson, 1992) was used to measure positive social behaviors. In the academic setting, the 3 participants increased positive social behaviors by 84%, 84%, and 87%. Generalized effects of CWPT were not found for social-setting behaviors. In the social setting, 2 children increased positive social behaviors by 28% and 21%; 1 student’s result was an outlier. Once peer coaching was added to the CWPT in later phases, the 3 students’ mean positive social behaviors increased from 32% to 62%, 47% to 75%, and 69% to 90%, respectively. Comparing performance when peer coaching was added to the CWPT-only phase suggests that peer coaching improved student outcomes in social settings relative to CWPT alone. When using the Attention Scale of the Behavior Assessment System for Children (Reynolds & Kamphaus, 1992) to address behavior and emotional qualities, the teacher reported improvements of varying amounts in all 3 students.
Watkins and Wentzel (2008) examined the difference that involvement of a peer partner as a facilitator during a planning task would make regarding social participation dynamics and problem-solving methods of children with ADHD. Each child was provided with a shopping list and asked to plan possible routes through an imaginary town to the stores needed to obtain the items in 25 min. Several days after the pretest, the children repeated the same task with a trained peer partner without a time limit. Systematic observational coding of eight target behaviors during the collaborative sessions indicated that the participants significantly increased joint participation (p < .01, d = 0.70) and collaborative (p < .01, d = 0.60) behaviors and decreased dominance behaviors (p < .01, d = 0.83).
Interventions Incorporating Peers With Attention Deficit Hyperactivity Disorder
Four studies assessed the influence of social skills interventions involving interactions with peers with ADHD in a group therapy setting. In a Level II study, Frankel et al. (1997) explored the efficacy of a social skills training intervention that involved role-play and coached play with a peer. Compared with the wait-list control group, the intervention group had significantly better scores on the teacher-reported Aggression scale of the Pupil Evaluation Inventory (PEI; p < .05; Pekarik et al., 1976) and the parent-reported Assertion and Self-Control subscales of the Social Skills Rating System (SSRS; p < .05; Gresham & Elliott, 1990). No significant difference was found between groups in performance on the Hyperactivity and Inattention scales of the PEI (p > .25).
In a Level III study, Corkum et al. (2010) examined the effectiveness of the Working Together Program, which focuses on a range of social skills including making conversation, giving introductions, making positive statements to others, speaking assertively, using courtesy words, asking for help, offering and giving help, giving and accepting criticism, joining a play activity, and negotiating conflict. The intervention included role-play and group activities with peers that targeted the social skills. Parent and teacher ratings of overall social skills on the SSRS improved significantly (ps = .05 and .04, respectively). Student self-ratings at posttreatment were slightly higher than at pretreatment but did not reach statistical significance.
Hoza et al. (2003) conducted a Level III study of the effects of a summer treatment program that consisted of a behavioral point system, peer-oriented interventions, dyadic peer interventions, sports skills training, academic remediation, participation in recreational activities, and weekly parent trainings. Each child was paired with a buddy to promote friendship skills while participating in program activities. The buddy’s antisocial behavior was significantly predictive of the children’s academic improvement and normalization. Children paired with a less antisocial buddy were viewed as more normalized (p < .001), showed more improvement in academic performance, and had higher quality friendships (p < .001). Parental compliance with the buddy system was predictive of the children’s perception of companionship (p < .001) and was marginally predictive of positive adaptation (p < .10).
In a Level III study, Hansen et al. (2000) examined the Kids Together program, which uses play therapy, role-playing, board games, and expressive arts to enhance social skills in a group therapy setting. Children practiced emotion identification, nonverbal communication, self-image and others’ perceptions of them, self-monitoring and organization, impulse control, conflict resolution, and responsibility with their peers. After the intervention, the children demonstrated significant improvements in internalizing behavior problems (p = .008) and total behavior problems (p = .011). Externalizing behaviors decreased, but not significantly (p = .051).
Discussion
The purpose of this systematic review was to investigate existing evidence for the benefits of incorporating peer interactions into interventions promoting social skills attainment in children with ADHD. Fifteen articles explored social skills interventions incorporating TD peers or peers with ADHD. The children with ADHD who were paired with TD peers showed more consistent and significant improvement in social play skills, pragmatic language, and problem solving postintervention. Follow-up performance assessments in 5 studies indicated that children maintained improvements in social skills but did not demonstrate further improvement (Barnes et al., 2017; Cantrill et al., 2015; Wilkes-Gillan et al., 2014; Wilkes-Gillan, Bundy, Cordier, & Lincoln, 2016; Wilkes-Gillan, Bundy, Cordier, Lincoln, & Chen, 2016). However, none of the studies incorporating peers without ADHD included a follow-up assessment past 18 mo, so the long-term impact of the interventions cannot be generalized. Interventions involving peers with ADHD focused on improving a variety of social skills in addition to reducing negative behaviors.
The considerable adult (e.g., parent, teacher, therapist) involvement in the social skills interventions of these studies requires further discussion. The extent to which the social skills improvements can be attributed to the incorporation of peers when adults were also part of the intervention (albeit in a different role from that of peers) is unknown. However, a systematic review by Storebø et al. (2019) of 25 randomized clinical trials on social skills training for children with ADHD found no significant differences between groups that participated in social skills training and groups that received no intervention. In that review, social skills training focused on teaching the children how to read subtle cues in social interactions, typically with parents and teachers. Storebø et al. found that interventions primarily using parents and teachers, rather than peers, had no significant effects on outcomes, unlike the results from studies in our review, in which incorporating peers in the interventions produced significant improvements in most cases.
Overall, study outcomes provide moderate evidence supporting the use of social skills interventions for children with ADHD that incorporate peers both with and without ADHD to increase play skills, reduce undesirable social behaviors, and improve communication and social participation. The findings of this systematic review can be used in practice to improve social skills development and ultimately social participation by children with ADHD. Occupational therapy practitioners can use these findings to support inclusion of peers in the intervention process across multiple settings and in a variety of roles. Regardless of intervention modalities used, studies incorporating peers were effective at improving social skills of the children with ADHD. Targeting behaviors in the natural environment can help efforts made in therapy generalize beyond the intervention and promote further improvements in play skills with repetition after intervention has ceased. Improved outcomes and generalizability of skills across environments resulting from teaching and involving parents during the intervention process were an additional practical implication of this review. However, it is important to note that the lack of high-level studies addressing this topic limits understanding of the role that peer inclusion plays in occupational therapy practice and how it can be used to promote generalization of social skills learned in therapy.
Strengths and Limitations
Strengths of the 15 studies include statistically significant improvements after implementation of a social skills intervention and promotion of interactions with peers. In addition, a majority of the studies (9 of 15) used multiple outcome measures, providing more data to qualify results. Involvement of parents during the intervention process demonstrated a positive influence on outcomes and increased generalizability of skills across environments. Finally, 5 studies reported maintenance of improvements at follow-ups of previously conducted intervention studies, suggesting that children with ADHD were able to maintain improved skills over time, even though outcomes were not always significantly different between postintervention and follow-up assessments.
Limitations across the 15 studies included the lack of a control group (13 studies), participant dropout (6 studies), lack of blinding of researchers scoring assessments (7 studies), small sample sizes and limited generalizability to pediatric populations (5 studies), and insufficient evidence regarding generalizability of skills across environments and long-term outcomes. In addition, discussion was limited regarding medication use and its effects on children’s social interactions during interventions. Only 1 study demonstrated Level I evidence; the remaining 14 studies provided lower evidence because randomized groups were not used, indicating that groups were not blinded to intervention, which may have influenced performance outcomes. Finally, many studies had small sample sizes (<20 total participants).
The primary limitation of this review is that the studies did not always use peers as the primary intervention. Many modalities were used in addition to peer involvement, making it difficult to clearly identify the incorporation of peers as the reason for improvements in social skills. Additionally, peers were often siblings or of the opposite gender, possibly resulting in different social expectations for the interactions. Inclusion only of studies available in English and published in peer-reviewed journals was a limitation of the study selection process.
Future Research
Further research is needed to provide additional support for incorporating peers in social skills interventions for children with ADHD. Higher level studies are needed that strive to create specific intervention guidelines and that include control groups, blinding of researchers, randomization of participants, and larger sample sizes. Future research should also include longitudinal studies to track long-term outcomes.
Implications for Occupational Therapy Practice
Our findings from the 15 studies indicate that social skills interventions incorporating the use of peers are beneficial for children with ADHD, and in some cases their TD peers as well. The findings suggest the following implications for occupational therapy practice:
• Social skills interventions incorporating the use of peers with or without ADHD are feasible and have the potential to be an effective method for improving social interactions for children with ADHD.
• Play-based and school-based interventions that incorporate TD peers can help improve social skills of children with ADHD.
• Social skills interventions combining multiple modalities—for example, parent involvement, video feedback, and play—in addition to incorporating peers have the potential to result in greater improvements in social behaviors for children with ADHD than one intervention method alone.
Conclusion
Research has demonstrated that social skills interventions incorporating peers for children with ADHD can contribute to improved social interactions and participation across multiple environments. Social skills interventions involving multiple modalities that incorporate peers in various roles can result in improvements in social behaviors for children with ADHD. It is important to practice social skills in natural environments to generalize skills across different contexts. Educating parents and caregivers about supportive strategies and appropriate play can help children generalize skills to the home environment. More research is needed to demonstrate the long-term effectiveness of interventions incorporating peers and generalization across environments.
Footnotes
Acknowledgments
This study was completed at the University of Texas Medical Branch, Galveston. We thank Chelsea Jordan for assistance with establishing a research topic and initial article searching.
Appendix
*
Indicates studies that were systematically reviewed for this article.