
Abstract
According to the National Institutes of Health, approximately 1 in 285 children in the United States will be diagnosed with cancer before their 20th birthday, and an increasing number of these children are surviving but with significant side effects (Noone et al., 2018). These side effects include impaired growth and development, impaired cognitive functioning, difficulty obtaining employment, and reduction in quality of life (Robison et al., 2009).
The increase in survival rates is due in part to improvements in medical treatment options, including hematopoietic cell transplantation (HCT), or bone marrow transplant, which is commonly used when other treatments have been unsuccessful. HCT involves the infusion of hematopoietic stem cells—harvested from bone marrow, peripheral blood, or umbilical cord blood—into the recipient using either the recipient as the donor (autologous) or another person as the donor (allogeneic). However, allogeneic transplant is associated with life-threatening complications, including infection, organ dysfunction, and graft-versus-host disease (GvHD). Moreover, prolonged hospital admission for HCT is associated with significant physical deconditioning (Hacker et al., 2017), which may further increase risk for health complications.
Oncology is an emerging practice area for occupational therapy practitioners, as evidenced by the development of the American Occupational Therapy Association’s Occupational Therapy Practice Guidelines for Cancer Rehabilitation With Adults (Braveman & Hunter, 2017). However, evidence that addresses the role of occupational therapy practitioners in pediatric oncology is lacking. In addition, the benefits and efficacy of occupational therapy interventions as preparation for occupational engagement for pediatric patients undergoing HCT need to be explored.
Children treated with HCT have an increased risk of experiencing performance limitations that restrict participation in activities of daily living (ADLs) and social participation (Ness et al., 2005). In addition, more than 70% of childhood cancer survivors treated with HCT experience physical dysfunction, psychological stress, and problems with social adaptation (Ishida et al., 2010). Specifically, these children are more likely to experience congestive heart failure, secondary cancer diagnoses, stroke, emotional difficulties, and participation restrictions than their healthy peers who have not undergone HCT (Ness et al., 2005). Pediatric transplant recipients also experience increased fatigue, decreased physical activity, and impaired social functioning (Hacker et al., 2006). Experiencing such side effects could have a profound impact on a child’s motivation to participate in meaningful activities, including ADLs, play, and leisure.
Occupational therapy practitioners can provide skilled interventions to address performance limitations throughout the transplant process. Occupational therapy interventions include engagement in meaningful activities throughout hospitalization to improve coping and motivation. In addition, physical activity can be incorporated into purposeful tasks to enable patients to maintain or rebuild the strength, coordination, and endurance necessary for engaging in daily life activities. The current literature supports physical activity, including exercise, as a mode of therapeutic intervention for pediatric and adult patients undergoing HCT, demonstrating its positive effects on overall health and physical performance.
Beginning exercise interventions during the inpatient phase of pediatric HCT hospitalization is feasible and effective (Chamorro-Viña et al., 2010), has positive effects on physical function and functional performance (Yildiz Kabak et al., 2016), and is associated with increased muscle strength and improved overall health benefits (San Juan et al., 2008). Although the literature shows positive effects of therapeutic exercise on aerobic fitness, physical fitness, strength, emotional status, and other health-related factors, variability across the studies in service settings (e.g., inpatient, outpatient, home exercise programs) and in levels of intensity suggests that further study is needed to optimize intervention delivery.
Ibanez and colleagues (2018) demonstrated the safety of occupational therapy interventions with this population, concluding that bleeding events in children who received exercise interventions while undergoing HCT are minor and rare. However, most published studies involve adult patients and do not address the impact of physical activity on occupational therapy’s domain of concern, that is, participation in occupations. The available evidence does not expand beyond the scope of exercise to include physical activity that occurs through engagement in meaningful tasks. Therefore, there is a critical gap in the literature regarding the efficacy of pediatric occupational therapy interventions for children undergoing HCT.
The purpose of this study was to evaluate the functional benefits and effects of two therapeutic frequencies on client-centered, evidence-based occupational therapy interventions for pediatric patients admitted for HCT. The objective was to demonstrate the benefits of participation in occupational therapy throughout a patient’s inpatient stay for HCT on upper extremity (UE) strength, independence in ADLs, and fine motor coordination. Specifically, the goals were to decrease the functional decline typically experienced by children undergoing HCT and to demonstrate that these children were able to return closer to baseline performance by the time of discharge instead of experiencing lasting effects on function. In addition, the study explored whether pediatric patients who have undergone HCT have better functional outcomes when participating in frequent occupational therapy (i.e., 4–5×/wk) than when participating in less frequent occupational therapy (i.e., 1–3×/wk).
Method
This study was prompted by an interdisciplinary project aimed at improving medical outcomes among children admitted for HCT treatment by providing them with a variety of skilled therapies that promote engagement in physical activity throughout their hospital admission (Gonzales et al., 2019). The disciplines involved were physical therapy, occupational therapy, speech therapy, massage therapy, therapeutic recreation, child life, art therapy, music therapy, and psychology. The program was developed and led by a transplant physician and physical therapist at a large Midwestern children’s hospital. Professionals from each discipline selected their preferred assessment tools and outcome measures and developed a treatment protocol based on commonly accepted standards of care.
The occupational therapy treatment protocol was created after a systematic literature review and survey of occupational therapy practitioners treating patients in oncology at top pediatric cancer hospitals. Members of the interdisciplinary team worked together to create an electronic treatment schedule for each patient. Children were evaluated by professionals from each discipline within 3 days of admission for baseline, or pretransplant, performance level. An occupational therapy plan of care was established immediately after the initial evaluation, and treatment was offered daily for the remainder of the admission.
Occupational therapy sessions were generally scheduled in the morning to allow for participation in ADLs as part of the morning routine. Per the protocol of this program, occupational therapy treatment was offered 5 days/wk, with a duration goal of 30 min per session, to all patients receiving HCT. Treatment was suspended for medical instability (e.g., decreased activity as a result of low hemoglobin or platelets, severe nausea or vomiting, acute events such as new-onset organ dysfunction, infection, GvHD). The determination to suspend therapy was made on an individual basis and done in collaboration with the medical team. In addition, some patients elected not to participate 5 days/wk because of disinterest or child or parent refusal.
Treatment varied according to individual needs and included out-of-bed physical activity, such as engaging in meaningful play and leisure tasks, participating in ADLs and modified ADLs (when appropriate), practicing fine motor skills through purposeful activities, and performing UE strengthening exercises. Examples of activities for school-age children included playing dress up or make believe, standing to dance or play a movement-based video game, practicing developmental skills such a writing their name or tying their shoes, and making a beaded bracelet for a parent or sibling. Examples of activities for teenagers included getting out of bed to complete ADLs before a friend came to visit, going for walks in the hallway and interacting socially with those present, and participating in an UE exercise program.
A final occupational therapy assessment was completed before discharge to guide discharge planning, evaluate the need for home-based therapy referrals, and create individualized home education programs. All members of the interdisciplinary team met 1×/wk to discuss patients’ medical status and needs and to provide an update on the progress of each discipline. Before the implementation of this program, patients typically received treatment from clinical therapies an average of 2–3×/wk.
Retrospective chart review was used to determine which patients were seen at the higher frequency (4–5×/wk) and which were seen at the lower frequency (1–3×/wk). Grip strength, fine motor coordination, and ADL functional scores were recorded by the treating therapist at pretransplant time of admission (baseline), weekly throughout admission (to determine peak decline after transplant), and at time of discharge. Note that peak decline indicates the lowest occupational therapy metric after admission for transplant. The Pediatric Evaluation of Disability Inventory–Computer Adaptive Test (PEDI–CAT; Dumas et al., 2012) Daily Activities score was recorded at baseline and at time of discharge. All data for analysis were obtained retrospectively.
Participants
Thirty-two pediatric transplant recipients participated in the occupational therapy interventions within the interdisciplinary project. These patients were admitted for HCT between September 2016 and December 2018 and met the following criteria: English or Spanish speaking, English- or Spanish-speaking caregiver or parent, and age <21 yr and >5 yr. Participants were excluded if they were unable to follow directions to complete required assessments. The limitation to only English- and Spanish-speaking participants, parents, and caregivers was used because one of the standardized assessments, the PEDI–CAT, was only available in English and Spanish. Patient data were prospectively entered into flowsheets within the electronic medical record and then retrospectively obtained from chart reviews for data analysis. All occupational therapy assessments were completed according to the standard of care.
Institutional review board approval for a retrospective patient data analysis was obtained. All procedures in this study were conducted according to regular standards of care for this patient population and as part of a quality improvement initiative. Therefore, a waiver for the requirement of written and verbal informed consent was granted.
Variables and Outcome Measures
The study used a retrospective time-series design to investigate the relationship between the independent variable (frequency of occupational therapy services per week) and the dependent variables (grip strength, fine motor dexterity, and level of ADL performance). Quantitative measures, which were recorded at pretransplant time of admission (baseline), at weekly intervals throughout admission to capture peak decline, and at time of discharge, included independence in daily activities using a child-appropriate functional measure of ADL, grip strength using a dynamometer, and fine motor dexterity using the 9-Hole Peg Test (9HPT). In addition, scores from the PEDI–CAT Daily Activities domain were used to assess level of child participation in ADLS at initial evaluation and discharge.
Activities of Daily Living Functional Measure
The ADL functional measure is a modified measure of independence in daily activities, adapted from the WeeFIM® (McCabe & Granger, 1990) to be applicable to this patient population. Items were rated on a scale ranging from 1 (completely dependent) to 7 (completely independent). Higher scores represent a more independent patient, and lower scores represent a patient who needs more assistance with ADLs. Items included feeding and eating, grooming, UE dressing, lower extremity dressing, toilet hygiene, functional toilet transfer, and bed mobility. The WeeFIM was modified to exclude bathing because the patient population was unable to bathe or shower in a traditional manner. No reliability or validity data are available for the adapted version. However, the WeeFIM has been used with a wide variety of populations and has well-established psychometric properties (Tur et al., 2009). Scores were obtained using skilled therapist observation, and the same therapist consistently worked with each patient.
Dynamometer
The B&L Engineering hydraulic hand dynamometer (Santa Ana, CA) measures grip strength with an acceptable interinstrument reliability and concurrent validity with the gold-standard Jamar dynamometer (Sammons Preston Rolyan, Bolingbrook, IL; Mathiowetz et al., 2000). A one-repetition score was recorded at baseline, weekly throughout hospitalization, and at time of discharge.
9-Hole Peg Test
The 9HPT is a commonly used test of fine motor dexterity that has excellent test–retest reliability (.95) and interrater reliability (.98; Oxford Grice et al., 2003). The assessment was completed by all patients using the standardized protocol; a stopwatch was used to record time to the nearest second.
Pediatric Evaluation of Disability Inventory–Computer Adaptive Test
The PEDI–CAT was designed for use with children and youth ranging in age from 0 to 20 yr with a variety of physical or behavioral conditions. The Daily Activities domain assesses the level of assistance required in four content areas: Getting Dressed, Keeping Clean, Home Tasks, and Eating and Mealtime. Dumas et al. (2017) identified the PEDI–CAT as a reliable and valid tool for use with children with a variety of conditions in any clinical setting. This parent-report measure was used at baseline and at time of discharge.
Data Analysis
Demographic data were summarized using descriptive statistics. Mean and standard error or median and range were used for quantitative variables, and frequency and percentage were used to summarize categorical variables. Comparisons of demographic and transplant characteristics between the two occupational therapy frequency groups were done using nonparametric statistical methods. For quantitative characteristics (i.e., age), the Mann–Whitney U test was used, and for categorical characteristics (i.e., gender), a χ2 or Fisher’s exact test was used. To determine overall and by-group differences in occupational therapy outcome measures over time, linear mixed-effect models were used with a random intercept as a random effect, and time point of measurement, frequency group, and their interaction were included as fixed effects. An additional mixed model was created to further assess grip strength measure by controlling for age and gender. The p values were two sided, and outcomes with p < .05 were considered statistically significant. Those p values resulting from linear mixed models were adjusted for multiple comparisons using the Holm method. We checked assumptions for linear mixed models while running analyses. All analyses were performed using SAS software (Version 9.4; SAS Institute, Cary, NC)
Quality
Several methods were used to ensure the validity, fidelity, and quality of the study. For interrater reliability, the two therapists who completed the assessments throughout the study were trained together in the use of each assessment to ensure consistency. Specific patients were evaluated and treated consistently by the same therapist throughout their admission. All patients were treated according to the established standard of care and had an equal opportunity for participation in occupational therapy services.
Results
Patient Demographics
Thirty-two patients were included in the study. No significant differences were noted between the high- and low-frequency groups regarding age, type of transplant, or diagnosis (Table 1). Twenty patients were in the high-frequency group (4–5×/wk), with a mean frequency of 4.3×/wk (standard deviation [SD] = 0.3). Twelve patients were in the low-frequency group (1–3×/wk), with a mean frequency of 2.5×/wk (SD = 0.9).
Patient Demographics (N = 32)
Note. BMT = bone marrow transplant; Mdn = median; OT = occupational therapy; TPN = total parenteral nutrition.
Donor type includes allogenic transplant patients only.
An intensive chemotherapy regimen that destroys bone marrow cells (Atilla et al., 2017).
A conditioning regimen that uses less chemotherapy and radiation than the standard myeloablative conditioning regimen (Atilla et al., 2017).
The first of 3 consecutive days when the absolute neutrophil count was greater than 500 as measured in the peripheral blood of the recipient after receiving hematopoietic stem cells.
Fine Motor Dexterity
Fine motor dexterity was determined using the 9HPT (task completion time scores shown here as mean [M] ± standard error of the mean [SEM]). For all patients, there was an expected decrease in performance from baseline to posttransplant peak decline (26.8 ± 11.1 vs. 36.9 ± 2.4 s, respectively, p < .0001; linear mixed model) and then a significant return toward baseline at time of discharge (36.9 ± 2.4 vs. 26.3 ± 1.1 s, respectively, p < .0001; linear mixed model; Figure 1A).
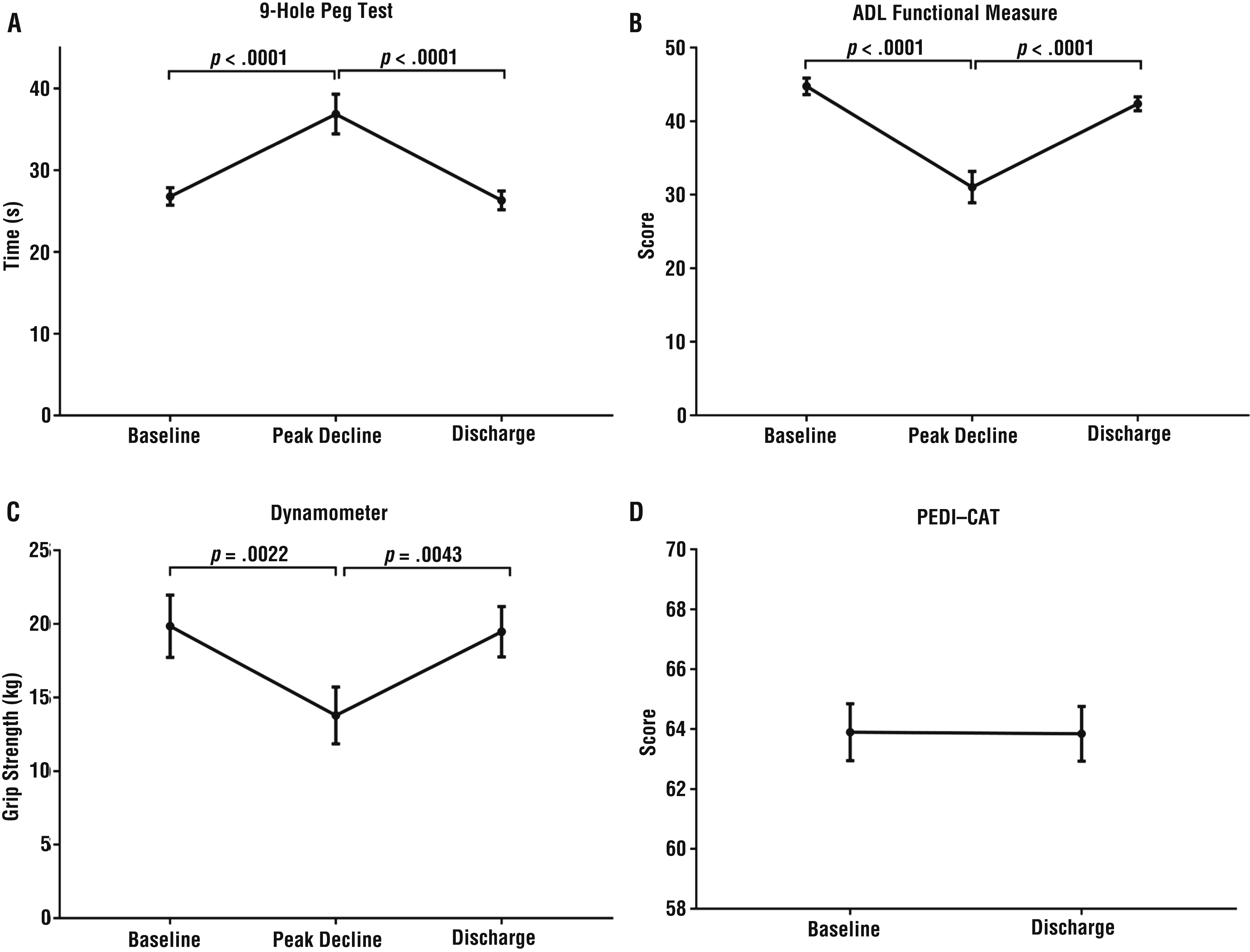
Participant performance in occupational therapy interventions from baseline to discharge.
The patients in both the high- and the low-frequency groups had similar 9HPT scores at baseline (27.7 ± 1.4 s vs. 25.3 ± 1.6 s, respectively). However, those in the low-frequency group had a significantly greater decrease in fine motor function at posttransplant peak decline (44.3 ± 5.0 s) than the high-frequency group (32.4 ± 2.0 s, p = .0027; linear mixed model; 95% confidence interval [CI] [6.1, 22.4]). Both groups were close to their baselines at time of discharge (high-frequency group, 25.6 ± 1.1 s; low-frequency group, 27.5 ± 2.4 s; Figure 2A). Together, these results show that the decrease in fine motor coordination throughout hospital admission was significantly less among patients who received therapy at the higher frequency than among patients who received therapy at the lower frequency (Figure 2A), suggesting that a higher frequency of occupational therapy was effective at preventing as significant a decline in fine motor dexterity during their hospital admission. However, no significant difference was found at time of discharge.
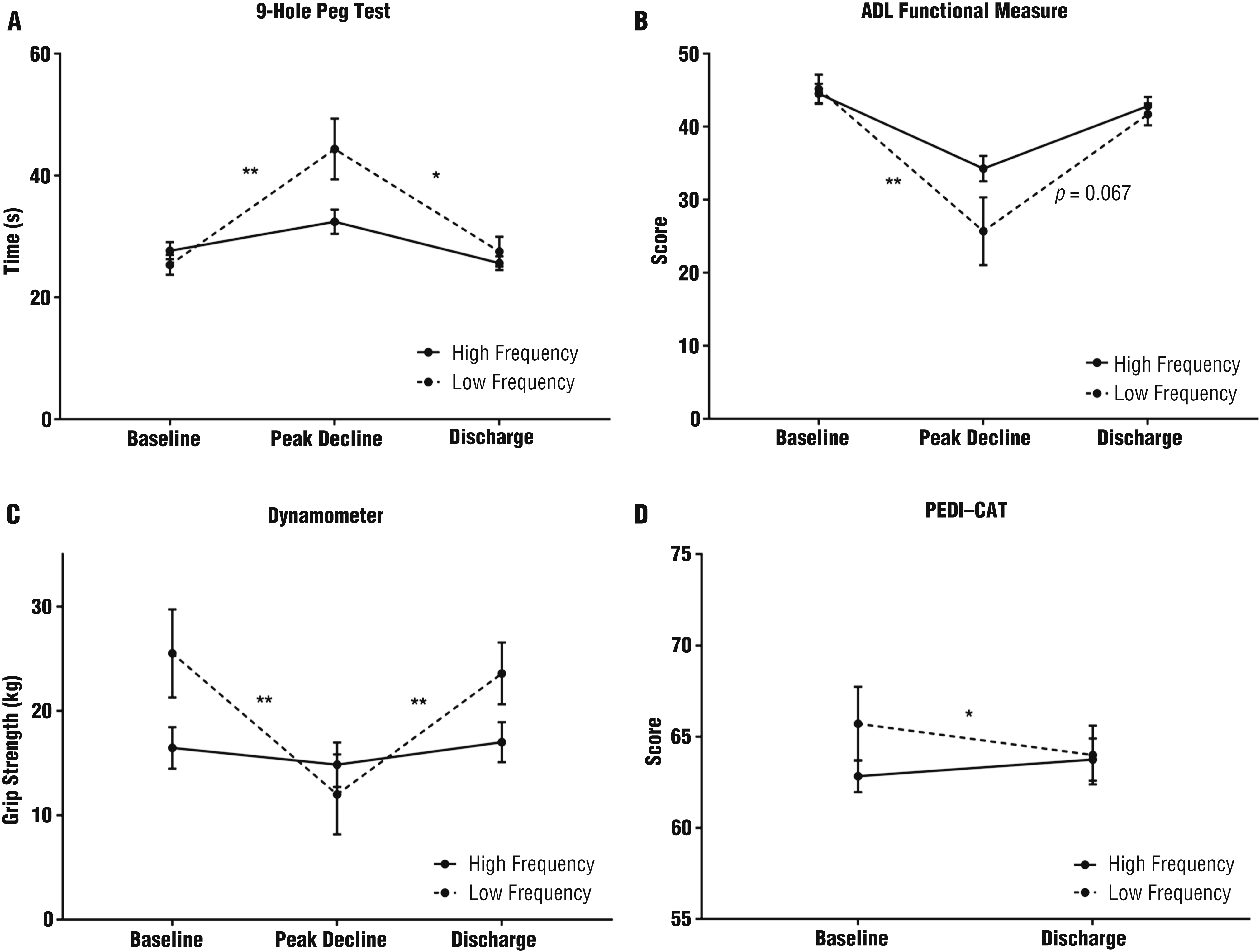
Low- and high-frequency group performance in occupational therapy interventions from baseline to discharge.
Performance in Activities of Daily Living
Performance in ADLs (scores shown here as M ± SEM) was examined using two different assessment tools, one through parent report (PEDI–CAT) and one through skilled therapist observation (ADL functional measure). ADL performance improved from posttransplant peak decline to discharge. For all patients, there was an expected decrease in performance from baseline to posttransplant peak decline (44.8 ± 1.1 vs. 31.0 ± 2.1, respectively, p < .0001; linear mixed model) and a significant return toward baseline at discharge (31.0 ± 2.1 vs. 42.4 ± 0.9, respectively, p < .0001; linear mixed model; Figure 1B).
To determine differences between the high- and low-frequency groups, additional analyses were conducted. Baseline scores for the ADL functional measure were similar for the high-frequency (44.5 ± 1.4) and low-frequency (45.2 ± 2.0) groups. However, the decrease in performance from baseline to posttransplant peak decline was greater for the low-frequency group (25.7 ± 4.6) than for the high-frequency group (34.3 ± 1.7; p = .0267; linear mixed model, 95% CI [ 2.4, 16.1]) before returning toward baseline at time of discharge (high-frequency group, 42.8 ± 1.2; low-frequency group, 41.7 ± 1.5; Figure 2B). Together, these results show that the high-frequency group experienced less significant decline in level of independence in ADLs than the low-frequency group before returning toward baseline at discharge (Figure 2B).
For all patients, PEDI–CAT scores were consistent at time of discharge with pretransplant scores (63.9 ± 1.0 vs. 63.8 ± 0.9; Figure 1D). The PEDI–CAT Daily Activities scores at time of admission for the high-frequency group and low-frequency group were 62.8 ± 0.9 and 65.7 ± 2.0, respectively. The high-frequency group experienced an increase in independence from time of admission to time of discharge (63.8 ± 1.2), and the low-frequency group demonstrated a decrease from time of admission to time of discharge (64.0 ± 1.6; p = .0170; linear mixed model, 95% CI [0.5, 4.7]; Figure 2D). Overall, patients who participated more frequently in occupational therapy had better outcomes for level of independence in ADLs.
Grip Strength
For grip strength (scores shown here as M ± SEM), there was an expected decrease in strength from baseline to posttransplant peak decline (19.8 ± 12.1 vs. 13.8 ± 1.9 kg, respectively, p = .0022; linear mixed model) and a significant improvement back toward baseline at discharge (13.8 ± 1.9 vs. 19.5 ± 1.7 kg, respectively, p = .0043; linear mixed model; Figure 1C). There was not a statistically significant difference between the high-frequency and low-frequency groups at baseline. However, the low-frequency group had a greater drop in grip strength from baseline to posttransplant peak decline (from 25.5 ± 4.2 to 12.0 ± 3.8 kg) than the high-frequency group (from 16.5 ± 2.0 to 14.9 ± 2.1 kg; p = .0015, 95% CI [5.5, 18.3]; Figure 2C). In addition, a return toward baseline at discharge was observed for the low-frequency group (23.6 ± 3.0 kg) but did not significantly differ for the high-frequency group (17.0 ± 1.9 kg; p = .09; linear mixed model; Figure 2C). Similar grip strength results were observed even when controlling for patient age and gender (data not shown).
Discussion
This study is the first to demonstrate that participation in occupational therapy throughout an inpatient hospital admission for pediatric HCT has a significant positive effect on grip strength, fine motor coordination, and self-care outcomes. In addition, study results demonstrate that participating in occupational therapy sessions at higher frequency (i.e., 4–5×/wk) is more effective than participating in occupational therapy sessions at lower frequency (i.e., 1–3×/wk). Results also provide further evidence that therapy participation leads to improved outcomes in physical function and functional performance, including increased muscle strength.
Outcomes of the current study are consistent with previously published research showing that participation in physical activity programs during an inpatient stay for pediatric patients is safe and feasible (Chamorro-Viña et al., 2010). No previously published research, however, has shown that participation in physical activity has a positive effect on independence in ADLs. In addition, no previous study has explored the benefits of a program promoting out-of-bed activity engagement that incorporates play and leisure, meaningful occupations, and ADL participation. Yildiz Kabak et al. (2016) studied the effect of aerobic and strengthening exercises on independence in ADLs among children undergoing HCT using the WeeFIM as an outcome measure. Statistical significance was not achieved in this study because of the baseline high level of independence among the study participants.
In the current study, the PEDI–CAT Daily Activities domain was added to measure complex daily tasks because the majority of children were independent at baseline in basic ADLs. This approach enabled us to show that participation in high-frequency therapy had a positive effect on independence in ADLs. Although both the high- and the low-frequency groups had an initial decline in ADL independence after transplant and then returned toward baseline according to the ADL functional measure, the high-frequency group improved from admission to discharge, but the low-frequency group declined, according to the PEDI–CAT results. This discrepancy could be the result of several factors, such as the parent-report nature of the PEDI–CAT (i.e., a parent may feel discouraged and frustrated with the hospital stay and hurriedly fill out the assessment before discharge, not reading questions as carefully as at time of admission) or the increased complexity of the PEDI–CAT tasks, which go beyond the basic ADLs that are part of the ADL functional measure.
Every effort was taken throughout this study to provide individualized, client-centered treatment. Treatment was provided on the basis of standards of care; however, individual interventions were tailored according to the needs of each child. A retrospective chart review revealed that the most common treatment methods for both the high- and the low-frequency groups included participation in ADLs, fine motor skills practice, UE exercise, and engagement in developmentally appropriate play or leisure occupations.
It could be argued that the high-frequency group had better functional outcomes as a result of covariates such as differences in preparatory regimen, treatment time, or acuity of illness throughout the treatment process. In other words, it may be hypothesized that the patients who were sicker participated less often in therapy and had worse outcomes. However, no clear underlying differences between the high- and low-frequency groups were noted regarding transplant type, conditioning regimen, length of stay (LOS), or total parenteral nutrition (Table 1). Moreover, both groups had a similar number of days of neutrophil engraftment and platelet engraftment (data not shown) as well as similar rates of infection (data not shown). Of note, differences in LOS approached statistical significance between the two groups, suggesting that participation in occupational therapy at a higher frequency may result in shorter hospital stays. However, further research with larger patient numbers is needed to confirm these findings.
The current study has several limitations. First, given the multidisciplinary approach to therapy received by inpatient transplant patients, positive functional outcomes directly attributed to participation in one specific therapy are potentially confounded by participation in all therapies. Nonetheless, metrics specific to occupational therapy were found to be significantly influenced by the interventions listed. Moreover, these findings suggest that participation in a novel, interdisciplinary program aimed at promoting engagement in out-of-bed physical activity has positive effects on ADL performance, fine motor dexterity, and grip strength. In addition, participation in more frequent therapy (4–5×/wk) resulted in more favorable outcomes than less frequent therapy.
Second, this study lacked randomization and a control group. It can be hypothesized that without participation in occupational therapy, children would not have returned to their baseline level of function; however, without a randomized controlled trial, this hypothesis is impossible to demonstrate. Because of the young age of the participants and the known benefits of participation in therapy, the care providers believed that withholding treatment from some patients would not be prudent. Also, the study lacked blinded outcome measures because the treating and evaluating therapists were the same, and one of the outcome measures (ADL functional measure) did not have established psychometric properties despite being based on an assessment tool whose psychometric properties are well established.
Third, the small patient sample size is limiting for certain outcomes such as resource utilization. Yet, statistical significance was achieved in the measured occupational therapy metrics and outcomes as presented.
Implications for Occupational Therapy Practice
This study provides evidence supporting the benefits of a multidisciplinary program in achieving therapy goals in a pediatric HCT unit. Specifically, the study has the following implications for occupational therapy practice:
Occupational therapy is an important component of a multidisciplinary therapy program for pediatric patients undergoing HCT.
Occupational therapy dosing of 4–5×/wk is more effective than a lower dose of occupational therapy (1–3×/wk).
Conclusion
In summary, children who participated in skilled occupational therapy services 4–5×/wk as part of an interdisciplinary program aimed at engagement in physical activity throughout transplant admission had improved UE and ADL functional outcomes compared with children receiving lower frequency occupational therapy intervention. Further research is needed to provide additional supporting evidence for the intensity and specifics of selected occupational therapy intervention strategies in reducing resource utilization in this patient population. Findings from this study can serve as a model for the development of interdisciplinary programs to treat the vast complexities of pediatric patients undergoing HCT. In addition, this study provides a foundation for discussion on the development of pediatric-specific occupational therapy practice guidelines for oncology rehabilitation.
Footnotes
Acknowledgments
We thank our colleagues at Nationwide Children’s Hospital (Columbus, OH), including all the clinical staff who provided support during this study. Julia Colman also thanks her occupational therapy faculty advisors (Ruth Benedict and Kristen Pickett) at the University of Wisconsin–Madison for their guidance and support.