
Abstract
Praxis, in the context of motor development, is the neurological process of conceiving, organizing, and directing movements (Ayres, 1985; May-Benson & Cermak, 2007). Dyspraxia (also called developmental dyspraxia) refers specifically to the observable problems with the execution of skilled motor movements that result from dysfunction of praxis (Steinman et al., 2010). Dyspraxia is a heterogeneous condition (Barnhart et al., 2003; Hoare, 1994) primarily associated with underlying difficulties in cognitive action planning (Adams et al., 2016), motor execution (Hoare, 1994; Piek & Skinner, 1999), visual perception (Schoemaker et al., 2001), and somatosensory processing (Allen & Casey, 2017; Elbasan et al., 2012; Piek & Coleman-Carman, 1995).
Somatosensory processing refers to the sensory functions processed by the somatosensory cortex, including touch and proprioception (Ayres, 1979; Cermak, 1991; Gibbs et al., 2007). Ayres (1972) documented a group of children whose motor planning deficits appeared to originate from difficulties with somatosensory processing, which was termed somatodyspraxia in the Sensory Integration and Praxis Tests (Ayres, 1989). Ayres (1972) hypothesized that motor deficits seen in children with dyspraxia may result from years of erroneous tactile and proprioceptive processing, providing poor feedback for motor learning and leading to ineffective and inconsistent motor patterns. Somatodyspraxia continues to be a term commonly used by pediatric therapists to refer to dyspraxia that appears to primarily result from deficits in tactile and proprioceptive processing (Reeves & Cermak, 2002). However, because of the lack of easily administered, objective clinical assessments of somatosensory processing that can be routinely used in pediatric therapy practice, the degree of accuracy with which therapists identify somatodyspraxia in the general pool of children with poor motor coordination remains unknown.
The purpose of this study was to begin to fill this gap by pilot testing methods for clinical assessment of proprioception in children. Research and clinical tests of proprioception in children and adults often focus on spatial awareness (also called kinesthesia), which includes position and movement sense (Fugl-Meyer et al., 1975; Sigmundsson et al., 2000; Smyth & Mason, 1998). In addition to spatial awareness, this study also considered force perception (including the sense of force and sense of effort), which, despite being a major component of proprioception (Chu, 2017; Proske & Gandevia, 2012), is not often examined because it is difficult to isolate. Studies specifically designed to examine force perception have shown that accurate perception of forces applied to and generated from one’s body plays an important role in motor control (Chu et al., 2015; Mugge et al., 2009; Yen & Li, 2015). Assessments that can specifically identify subtypes of proprioceptive deficits in children will allow the development and testing of targeted interventions.
I postulated that 100% of children with somatodyspraxia referred to this study would be able to complete the battery of proprioceptive assessments administered. Despite the importance of the proprioceptive system in motor performance, motor deficits can stem from poor vestibular processing. Studies of subtypes of children with developmental dyspraxia have shown that 10%–30% of such children demonstrate good proprioceptive processing but poor vestibular function (Hoare, 1994; Macnab et al., 2001). Allowing for the potential recruitment of children with dyspraxia because of poor vestibular functioning, I postulated that at least 80% of the children in the somatodyspraxia group would have deficits in proprioception using objective measures. I hypothesized that children with somatodyspraxia would demonstrate lower scores on all measures of proprioception compared with age-matched control children.
Method
Participants
I recruited 10 children with somatodyspraxia ages 6–8 yr (mean [M] = 7.1, standard deviation [SD] = 0.85; 5 male and 5 female) and 10 typically developing children ages 6–8 yr (M = 7.8, SD = 1.1; 5 male and 5 female). Children with somatodyspraxia were referred from a private therapy clinic in Southern California. The clinicians who made recommendations for research participation were experienced in evaluating and treating children with sensory processing disorders and dyspraxia, and all had completed advanced training in sensory integration theory (University of Southern California/Western Psychological Services Sensory Integration Certification Program). The 10 children with somatodyspraxia who participated in this study were receiving occupational therapy at the time. Age-matched typically developing children were recruited from the University of Southern California and the University of Illinois at Chicago and surrounding areas.
The study was approved by the institutional review boards at both institutions. I obtained informed assent and consent from all the children and their parents. Children were excluded if they had a diagnosis of any notable neurological or neuromuscular disorder (e.g., cerebral palsy, brain injury) or major developmental cognitive or behavioral disorder (e.g., autism, trauma-related disorder).
Procedure
Children were invited to a quiet research room, free from distractions, to complete a series of tests (outlined next). While the children were participating, their parents were asked to complete a parent questionnaire and a demographic form. Total testing time was 30–45 min, and I administered all tests. Following current standard clinical practice, I compared my results with responses on the parent-report questionnaire to capture sensory processing difficulties.
Measures
Spatial Awareness
In this study, spatial awareness was defined as the ability to know where one’s limbs are in space relative to the rest of the body. It includes joint position sense (the ability to perceive joint angles) and movement sense (the detection of change in relative joint positions). The research setup included a custom-made frame; the children rested their forearm or hand on the lower level of the frame and indicated where they thought their arm was pointing using a small arrow on the top level (Figure 1A). The angle-matching error was defined as the difference between the arm angle and the arrow angle.
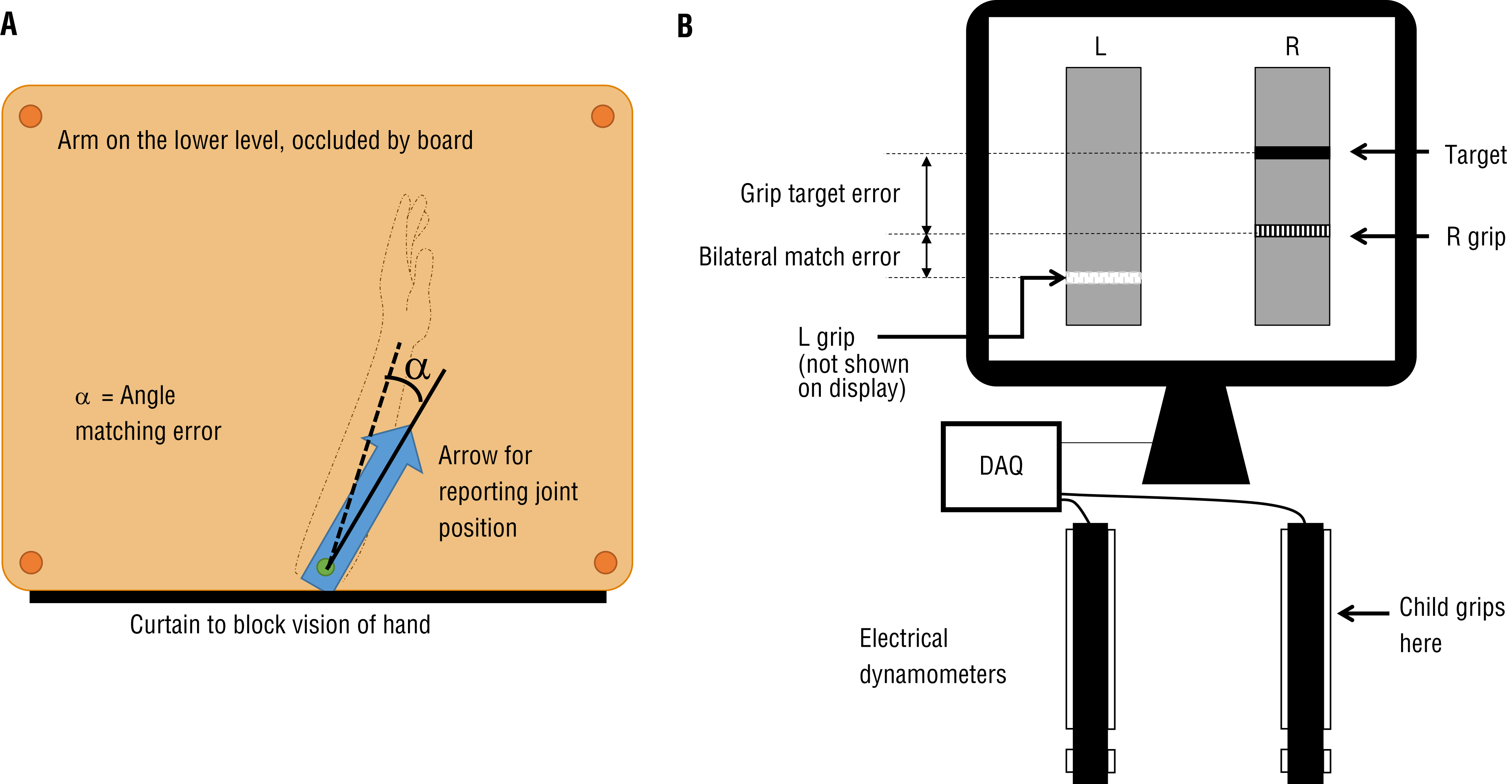
Experimental setup for the (A) spatial awareness and (B) joint perception tests.
Each child performed six trials on each of the following joints: left elbow, right elbow, left wrist, and right wrist. The testing angle range was divided into six sections that were evenly spaced (18° apart) to cover most of the physiological range of motion; the positions were selected at random for each trial. During each trial, the experimenter moved the joint to a new position while it was hidden under the curtain, and the child moved the visible arrow on the top to match the joint position of the unseen upper extremity. The six positions for each tested joint were presented in a random order. Joint position sense was measured by the angle-match error, the absolute difference between the arrow angle and the actual joint angle. I averaged the difference across all trials with the same joint (elbow and wrist). Movement sense was measured by movement direction accuracy, calculated as the percentage of times the child moved the arrow in the same direction as the joint movement.
Force Control and Perception
Force control is the motor system’s ability to coordinate muscles to grade forces exerted by the body (Lundy-Ekman et al., 1991; Smits-Engelsman et al., 2003), and force perception is the sensory system’s ability to detect and sense forces exerted by or applied to the body. In a test of force control and force perception, children sat in front of a computer screen with two electronic dynamometers (Hand Dynamometer HD-BTA, Vernier, Beaverton, OR) to perform the task. On the computer display, two bars provided feedback on the force measured by the dynamometers (Figure 1B). Children were first asked to grip the dynamometers as hard as they could, to measure their grip strength. Overall grip strength was calculated as the average of the maximum force produced by the two hands.
For the test trials, the children were asked to grip the dynamometers to match the target force displayed on the computer screen. The visual feedback of the force exerted was provided for only one hand. Matching the target force using the hand with the visual feedback provided a measure of force control because it measured the child’s ability to grade forces using visual feedback. Grip target error—the average difference between the target force and the actual force exerted on the hand with visual feedback, normalized by the child’s grip strength—provided a measure of force control.
To match the target for the hand without visual feedback, children had to match the forces in the hand without visual feedback to the hand with visual feedback. This required them to sense how it felt to exert a certain amount of force to match the target (hand with visual feedback) and then exert the same amount of force with the contralateral hand (hand without visual feedback). The bilateral match error—the average difference in forces exerted by the two hands, normalized by the child’s grip strength—provided a measure of force perception. The target forces were 5%, 10%, 15%, and 20% of the child’s maximum force. The four target forces were selected in the lower force range to minimize fatigue during testing. A total of eight trials were performed (four with visual feedback on the left hand and four with visual feedback on the right hand). The order of the trials was randomized.
Sensory Processing Measure
The Sensory Processing Measure (SPM; Parham & Ecker, 2007) is a 75-item questionnaire often used to characterize children’s sensory-related behavioral patterns as measured by parent report to aid in the identification of somatodyspraxia. I used the SPM to verify the referring clinicians’ judgments for somatodyspraxia and to compare the findings. The SPM categorizes responses into eight domains: Social Participation, Vision, Hearing, Touch, Taste and Smell, Body Awareness (BOD), Balance and Motion (BAL), and Planning and Ideas (PLA). Domain areas in the SPM that are related to somatodyspraxia include BOD, BAL, and PLA because these domains specifically examine the child’s sensorimotor function.
Data Analysis
Statistical analyses were performed using IBM SPSS Statistics (Version 26; IBM Corp., Armonk, NY). The number of children who completed the study was recorded. Descriptive statistics for the control group were computed for the six proprioceptive measures (elbow direction accuracy, wrist direction accuracy, elbow match error, wrist match error, grip target error, and grip matching error). Z scores on each measure were calculated for children in the somatodyspraxia group using the following formulas:

where X represents the raw data for elbow direction accuracy, wrist direction accuracy, elbow match error, wrist match error, grip target error, and grip matching error, and T represents the SPM subtest T scores. The SPM subtest T scores have a mean of 50 and standard deviation of 10 (Parham & Ecker, 2007). A Z score ≥2 is considered to denote considerable deficits. In Figures 2 and 3, the Z scores are capped at 3 for display purposes. For any measures for which the control standard deviation is 0, Z = 0 when X equals the control mean, and Z = 3 when X deviates from the control mean.
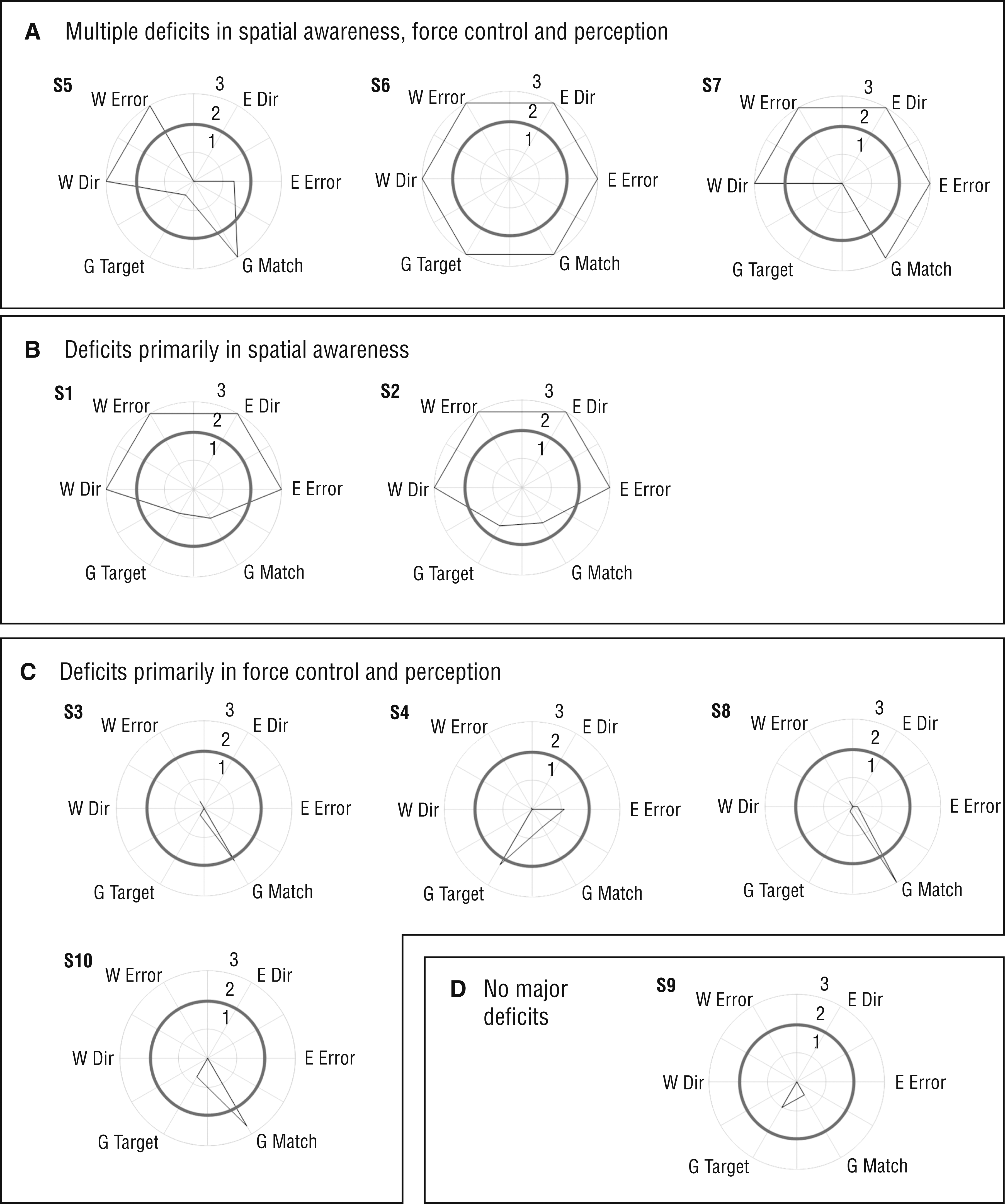
Z scores for proprioceptive measures for the somatodyspraxia participants (S1–S10), grouped by primary deficits observed.
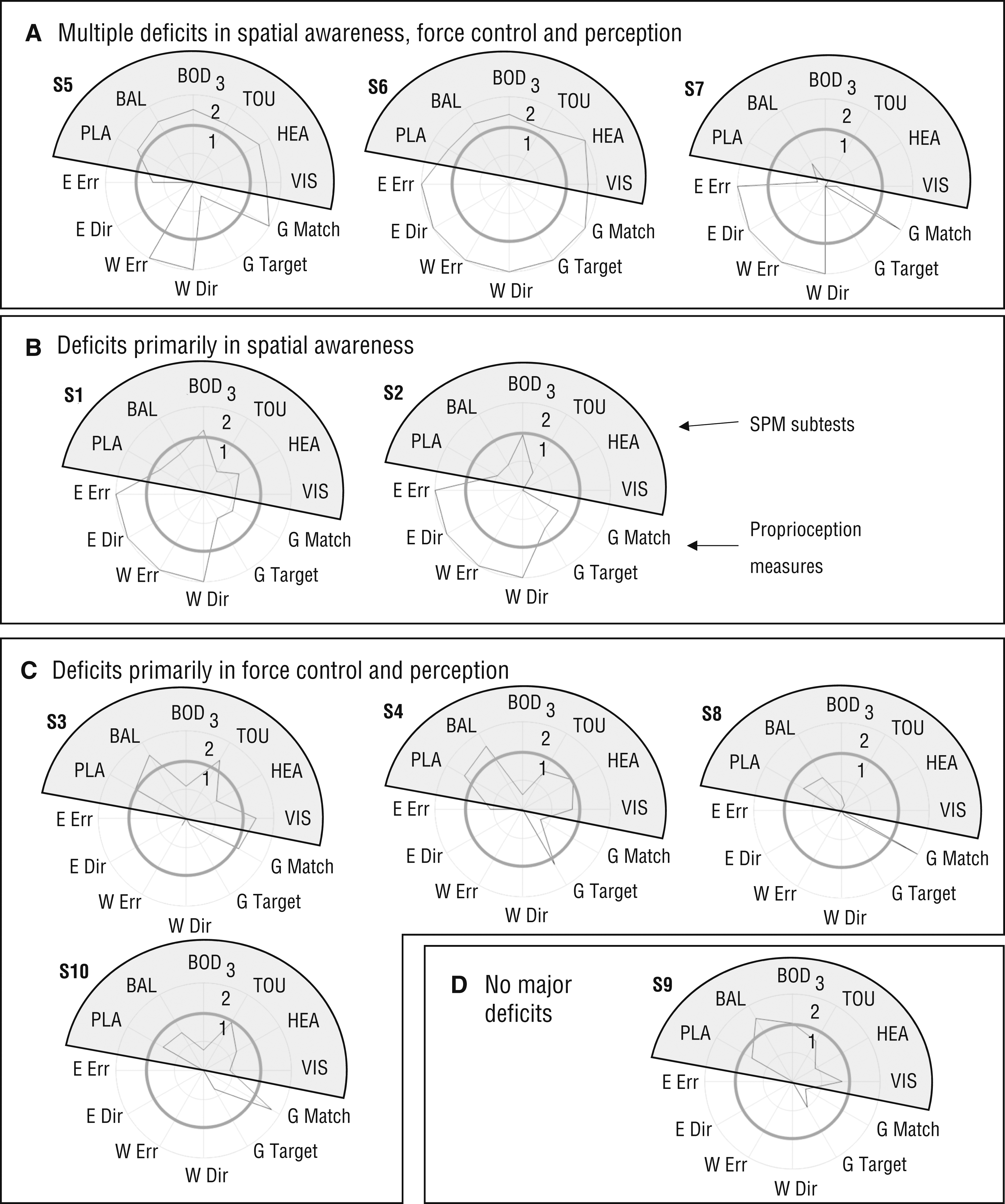
Z scores for the Sensory Processing Measure subtests and proprioceptive measures for the somatodyspraxia participants (S1–S10), grouped by primary proprioceptive deficits observed.
Because of the small sample size, group comparisons of the dependent measures (age, angle matching errors, direction accuracy, grip strength, force target matching error, and force bilateral matching error) were made with the nonparametric Kruskal–Wallis H test. The significance level was set at .05. Cohen’s d was also calculated for all measures to examine the effect size of the difference between the two groups. I also examined the group difference while controlling for the effect of age by conducting a general linear model on the ranks of the dependent measures with group as a fixed factor and age as a covariate, to parallel the nonparametric Kruskal–Wallis H tests.
Results
Children in the Somatodyspraxia Group
All children with somatodyspraxia referred to the study completed the battery of proprioceptive assessments. Nine of the 10 children in the somatodyspraxia group showed notable deficits (Z > 2) on at least one of the proprioceptive measures (see Figure 2). On the basis of a visual inspection of the graphs in Figure 2, the children can be categorized into four groups: those with deficits in both spatial awareness and force control and perception (3 children), those with deficits primarily in spatial awareness (2 children), those with deficits primarily in force control and perception (4 children), and those with no major deficits (1 child).
All but 1 child (Participant S7) in the somatodyspraxia group showed “some dysfunction” or “definite dysfunction” in at least one of the sensorimotor-related domains (BOD, BAL, and PLA) of the SPM. To examine the results of the proprioceptive measures in relation to the SPM, Z SPM scores were plotted alongside the proprioceptive Z scores in the same grouping as described earlier (Figure 3; note that Figures 2 and 3 describe the same proprioceptive measures but depict them slightly differently). Note that some children (S2, S7, and S8) did not score as having “definite dysfunction” (Z SPM > 2 or T > 70) on the SPM but showed notable deficits on the proprioceptive measures. However, 1 child (S9) scored as having “definite dysfunction” on the SPM but did not show major deficits on the proprioceptive measures.
Group Comparisons for Spatial Awareness and Force Control and Perception
The age difference between the two groups was not statistically significant (p = .112). Group comparisons were conducted to examine the difference in proprioceptive measures between typically developing children and children in the somatodyspraxia group. Children in the somatodyspraxia group had higher errors in identifying the direction of movement (elbow, p = .030; wrist, p = .036). In joint position angle matching, the difference between the two groups was significant in the elbow joint (p = .034) and neared significance for the wrist joint (p = .059). Children in the somatodyspraxia group performed notably worse on both grip target error (force control, p = .008) and grip bilateral matching (force perception, p = .001). The effect size was larger than 0.80 for all of the comparisons. Details of the statistical tests are presented in Table 1. The p values for the group factor for all spatial awareness and force perception measurements were similar after controlling for age, and they did not change the significance of any test results.
Summary of Statistical Results for Group Comparisons
Note. Effect sizes (d) were calculated for the differences between the two participant groups. All effect sizes were higher than 0.800 and thus considered large on the basis of statistical standards (Lakens, 2013). H = Kruskal–Wallis H score (df); M = mean; SD = standard deviation.
* p < .05.
Discussion
Feasibility of Testing Proprioception in Children
This study demonstrated the use of quantitative tests to examine spatial awareness and force perception in typically developing children and children with somatodyspraxia. Force perception is a difficult construct to test, especially in children, because of the reliance on cognitive, motor, and verbal output to assess sensory perception. Current clinical assessments that directly gauge proprioception (e.g., the Fugl-Meyer Assessment of Motor Recovery [Fugl-Meyer et al., 1975], finger-to-nose test, Sensory Integration and Praxis Tests) do not consider force perception separate from spatial awareness. The testing methods allowed me to differentiate force perception (which requires proprioception) from force control (which is primarily visual–motor in nature) and spatial awareness. All children were able to complete the assessments, and 90% of the children who were referred for having somatodyspraxia showed significant deficits in proprioception on the basis of the measures used, confirming that the measures align with the clinical judgment of pediatric occupational therapists. This demonstrates the feasibility of using this setup to examine proprioception in a larger population of children.
Individual Differences Among Children With Somatodyspraxia
Somatodyspraxia is a heterogeneous disorder. Examinations of the individual children’s data showed different patterns of deficits in children identified as having somatodyspraxia. Half of the children showed deficits in spatial awareness. Some of these children also showed deficits in force control and perception. The remaining children showed deficits only in force control and perception. On the basis of parent reports, the SPM showed that a majority of the children in the somatodyspraxia group had deficits in sensorimotor-related domains (BOD, BAL, and PLA); however, 3 children who showed significant deficits on the objective measures did not show “definite dysfunction” according to the SPM, thus suggesting the need for objective sensory testing in children with dyspraxia beyond relying solely on parent-report measures to guide appropriate intervention planning.
Group Differences in Proprioception
As a group, the children with somatodyspraxia had more difficulty identifying the direction in which their hand or arm had been moved, which is a core component of proprioception. They also had larger errors when they tried to match the angle of the elbow or hand with an arrow. These findings show that the deficits in proprioception of the children with somatodyspraxia often stem from poor proprioceptive discrimination. Group differences in force control and perception were also observed between the children with somatodyspraxia and the typically developing children. Even with visual feedback, children in the somatodyspraxia group had more difficulty matching force targets. Compared with typically developing children, they also had more difficulty matching forces in one hand to those in the other hand on the basis of proprioceptive input. The results show that the children with somatodyspraxia had significantly more challenges in their ability to grade forces and to perceive force exerted.
Future Directions
This pilot study had a small sample size of 20 children, which limits the generalizability of the results. Caution needs to be exercised when interpreting the Z-score results because they are derived from a small control sample. Future studies with more children can establish a baseline for comparison with children who have identified proprioceptive deficits. Further research is needed to establish diagnostic criteria for various proprioceptive deficits in children with motor delays and to help adapt proprioceptive training approaches for use in children with these deficits.
Dyspraxia has traditionally been treated as a motor disorder because of its key characteristics of motor coordination difficulties. The current study showed that children with somatodyspraxia demonstrated measurable proprioceptive deficits, highlighting the importance of assessing proprioceptive function in children who present with motor deficits. Future studies that link specific proprioceptive deficits with observable motor difficulties will provide further evidence on how proprioceptive deficits affect motor development. The ability to specifically identify proprioceptive deficits will allow for the development of targeted interventions for children with different kinds of proprioceptive deficits.
Implications for Occupational Therapy Practice
The results of this study have the following implications for occupational therapy practice:
Occupational therapy practitioners should be aware that children with dyspraxia can also experience difficulties with spatial awareness and force perception.
Deficits in spatial awareness and force perception should be taken into consideration when evaluating and treating children with somatodyspraxia to facilitate targeted interventions and improve treatment effectiveness.
Conclusion
This study tested methods for assessing position sense and force perception in children. On the basis of the results, I have presented a framework to quantify proprioceptive deficits in children that extends beyond clinical observations and parent-report measures. Additional research is necessary to establish diagnostic criteria for various proprioceptive deficits in children.
Footnotes
Acknowledgments
This research was conducted at the University of Illinois at Chicago (UIC) and the University of Southern California, Los Angeles, while I was a student at UIC.
This study could not have been completed without the assistance of the therapists and client families at the private therapy clinic in Southern California, and I thank them for their support of this research. I also thank S. Bodison (University of Southern California), and G. Fisher and K. Krishnan (University of Illinois at Chicago), who provided insight, expertise, and support that greatly assisted the research. I also acknowledge A. Sima, V. A. Rodriguez, and L. Thacker from the Virginia Commonwealth University (VCU) Department of Biostatistics and E. Boone from the VCU Department of Statistics for their consultation on statistical analysis for this project. Special thanks go to S. Reynolds for her assistance in reviewing the manuscript of the article.