
Abstract
Stakeholders can advocate for policies, standards, and additional training to support proactive, formal SE throughout adulthood for people with IDD.
The field of disability studies challenges and educates people about the stigma and oppression associated with disability and promotes access to civil rights, but thus far it has failed to adequately address the associated effects on sexuality (Shuttleworth, 2003). Sexuality, a fundamental human right, includes “sex, gender identities and roles, sexual orientation, eroticism, pleasure, intimacy and reproduction” and is integral to a person’s overall health and well-being (World Health Organization, 2015, p. 7). People with intellectual and developmental disabilities (IDD) 1 express interest in relationships and sexual activities, but at a slightly older age than their peers without disabilities (Kahn & Halpern, 2018). Despite a clear interest, they experience oppression surrounding their sexuality resulting from U.S. laws, related to their diagnosis, that prohibit them from consenting to sexual relationships (Linder, 2018) and offer only limited access to sexual health information (SHI; Grossman et al., 2004; Shuttleworth, 2003). Put more specifically, people with IDD lack opportunities to learn about SHI in school or at home; moreover, few sex education (SE) programs include the best practices identified for the general population (e.g., comprehensive programs; Barnard-Brak et al., 2014; Pownall et al., 2012; Schmidt et al., 2020).
Because of the limited information provided in schools and at home, the responsibility for SE provision may fall to health care providers, including occupational therapy practitioners who recognize the importance of understanding, respecting, and promoting sexuality. The American Occupational Therapy Association’s (2020) Occupational Therapy Practice Framework: Domain and Process (4th ed.) recommends that practitioners support clients’ participation in sexual activity as an activity of daily living; in formal education, including SE; and in social activities, such as dating. Few occupational therapy practitioners, however, currently provide SHI in practice (Young et al., 2020), perhaps because of the limited amount of time spent educating occupational therapy students about sexuality (Eglseder et al., 2018), despite models available to facilitate practitioners in addressing SHI (e.g., the Recognition Model [Couldrick et al., 2010] and the Ex-PLISSIT [Permission, Limited Information, Specific Suggestions, and Intensive Therapy] Model [Taylor & Davis, 2006]). Attention to SHI may be even more unlikely for occupational therapy clients with IDD, a population for whom little is known about best practices for SE provision (Schmidt et al., 2020).
Given that a person’s sexual citizenship or agency (i.e., the capacity to choose, engage in, and refuse sex acts and to be respected by others; Shildrick, 2013) can be affected by limited or inadequate SE, as can overall sexual health, a lack of comprehensive SE could have profound effects. Previous research has highlighted the need to explore recommendations and to identify occupational therapy practitioners as playing a unique role in the provision of SE (Krantz et al., 2016). To this end, our research sought to understand barriers to, the context of, and stakeholder recommendations for SE for people with IDD.
Method
Study Design
In this study, we used a qualitative design to understand (1) perceived barriers to SE, (2) the current context of SE, and (3) stakeholder recommendations for comprehensive SE for people with IDD.
Participants
A variety of stakeholders were recruited because of the limited evidence available regarding barriers to, the context of, and recommendations for SE practices specifically for people with IDD. Participants included residents of Ohio, ages 15 to 24 yr, with self-reported IDD; parents of children with IDD; health care providers; and sex educators in special education settings. Participants were excluded if they expressed an unwillingness to share their opinions in a group conversation.
A purposive, convenience sampling approach was used to identify local disability organizations, programs, and clinics through which to distribute emails and flyers for recruitment (Ritchie & Lewis, 2003). We sought to recruit 8 to 12 participants per stakeholder group, on the basis of evidence that data can be saturated within 12 interviews (Guest et al., 2006). Participants provided informed consent, assent, or parental permission before taking part in this study. All research was conducted in accordance with the approval of The Ohio State University’s institutional review board.
Qualitative Measures
Data were collected through semistructured focus groups and interviews; guides included open-ended questions followed by probing questions that were developed on the basis of literature regarding three topics: (1) best practices (e.g., comprehensive SE), (2) barriers, and (3) recommendations for people with IDD.
Procedure
All focus groups and interviews were completed, and audio recorded, in a private university laboratory space with a moderator (Elizabeth K. Schmidt) and assistant moderator (a graduate student). Focus groups were conducted separately with participants of the same sex and self-reported gender to increase participant comfort. The majority of interviews were completed over the phone (82%) with the moderator (Schmidt or graduate student). All participants received a $20 electronic gift card for their time.
Data Analysis
Data were analyzed using a constant-comparative approach to understand barriers to, the context of, and recommendations for SE for people with IDD. We familiarized ourselves with the data, engaged in the coding steps outlined in Figure 1, and reviewed all transcripts again using the identified themes (Glaser, 1965).
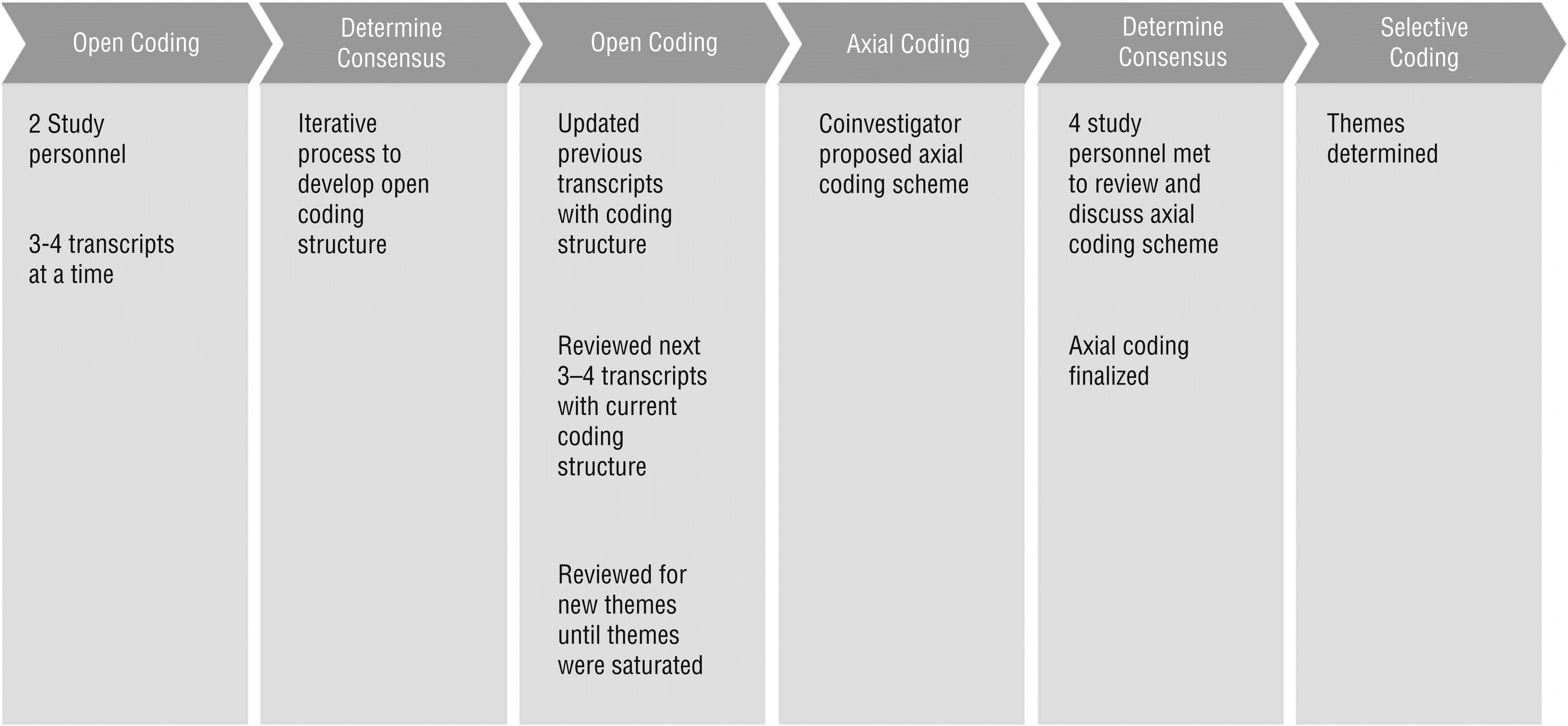
Steps for data analysis (Glaser, 1965).
Strategies to Achieve Trustworthiness
Triangulation of analysts and data sources was used to address credibility. Two researchers independently analyzed the transcripts and achieved a consensus of >85% on the coding structure. We also analyzed detailed field notes, from 50% of the interviews, to confirm alignment with transcript analyses. Finally, to address transferability of the analyses, we checked for representativeness across all stakeholders.
Results
Participants included people with IDD (n = 8), educators (n = 8), parents of children with IDD (n = 9), and health care providers (n = 12). They were interviewed between December 2018 and January 2019. Participants with IDD were ages 15 to 24 yr, were primarily male (75%), and had diagnoses such as Down syndrome, autism spectrum disorder, Prader–Willi syndrome, and intellectual disability. Educators and health care providers were primarily female (88% and 75%, respectively), and all parents (100%) were female. Health care providers came from a range of disciplines, including physicians (n = 2); nurses (n = 1); occupational (n = 1), physical (n = 1), and recreational therapists (n = 1); behavioral health providers (n = 5); and care coordinators (n = 1). Overall, our findings demonstrated three themes related to SE for people with IDD: (1) barriers, (2) context, and (3) recommendations.
Theme 1: Barriers to Sex Education
Our analyses revealed four major barriers to SE for people with IDD: (1) values and cultural issues, (2) parental attitudes toward their child’s sexuality, (3) a lack of organizational policies and standards, and (4) limited professional education or societal biases.
Values and Cultural Issues
Values and cultural issues refers to varying beliefs that affect SE regardless of disability status (e.g., difficulty navigating questions about masturbation and pornography). A health care provider emphasized that it was important “to understand cultural differences [in SE], which can be hard to learn.” Participants also discussed embarrassment as a barrier to SHI provision:
So again, I think it’s one of those nuanced things that is SUPER important to be asking about, but we as providers are so uncomfortable that we just ask about it really quickly and then disregard it, or it’s not really brought up at all. (Health care provider)
Parents and participants with IDD also reported being embarrassed to discuss these topics with one another or with educators and providers. One parent said, “It’s embarrassing” and “[my child] doesn’t want to talk about it.”
Parental Attitudes Toward the Child’s Sexuality
Health care providers and educators reported barriers related to parents’ attitudes about their child’s sexuality; for example, one educator said, “Their parents don’t really view them as adults [who] will be interested in sex.” Participants with IDD also reported this as a barrier. Specifically, they shared times when their parents or their friends’ parents had referred to them as childlike or “not ready” for relationships and sexual experiences: “Parents won’t talk about it because they don’t think it’s necessary, or they just don’t want to talk about it.”
Of interest is that parents also reported these characteristics as barriers. In fact, many parents reported using open communication to address sexuality with their child but recognized that other parents do not. Parents also identified specific topics throughout the interview they “probably should have addressed by now,” such as how to put on a condom.
Lack of Organizational Policies and Standards
Because SE is not mandated by the federal government, each state can develop its own requirements or allow schools to determine what is provided. Participants expressed that this inhibits educators from providing quality SE. Even in states that have SE standards, there are no requirements for accessibility; therefore, it is unclear whether education is meeting the needs of students with disabilities. One educator shared, “I would say he’s, you know, he’s the type of student who would need modifications for anything. So yeah, I would say, ideally, there would have been some support in place [for SE].”
Similarly, many health care providers suggested that “the biggest thing is there’s no real standards”; specifically, there is no institutional support to ensure that health care providers address SE with this population and to protect them against allegations of impropriety when they do address it. Therefore, providers and educators default to providing surface-level information.
Parents and participants with IDD also recognized this barrier. In fact, 1 participant with IDD shared that “unfortunately, in a school setting they don’t tell you—they just tell you a bit of [SHI] and some schools don’t have [SE].”
Limited Professional Education or Societal Biases
In addition to a lack of institutional support, health care providers and educators reported that they felt ill prepared to discuss SHI. According to 1 health care provider, “I think [we] as therapists tend to dance around it sometimes because we don’t know how to address it.” Others reported a clear need to educate professionals working with people with IDD to discuss SHI in an age-appropriate manner and eliminate biases. One educator described the biases that many professionals have toward the sexuality of people with IDD as a “weird overextension that all sex is bad and if anyone ever touches you it’s wrong” and shared that professionals need to be educated that “they’re still individuals [who] have the right to a healthy sex life as other adults if they want that . . . I mean I think offering trainings to help people with appropriate language—it’s not like ‘good touch, bad touch.’”
Parents and people with IDD identified societal biases as a concern as well. One mother reported that the biggest challenge to addressing SHI with her child was the perception others had of her child. She described a time when her daughter entered her first relationship and “the boy who liked her, he was a typical boy. [He] then came back and said, ‘My mom said I cannot be your boyfriend because you have a disability.’” Participants with IDD also took issue with these biases, emphasizing the importance of educating others to overcome them: “I have a disability, but that doesn’t change the fact that I want to make love and be loved.”
Theme 2: Context of Sex Education
The barriers just discussed led to SE that is currently either initiated by people with IDD or begun as a reactive response due to safety concerns or the onset of puberty.
Sex Education Initiated by Persons With Intellectual and Developmental Disabilities
SE often occurred through conversations initiated by people with IDD; specifically, participants reported their child, student, or patient sometimes asked questions about SHI or made incorrect statements that they then had to address:
For example, this past week the students were talking about childbirth and they were like “Babies come from mommy’s bellies” . . . and so we had to go into a little anatomy lesson about how there are other parts on a mom. (Educator)
In addition, participants reported that, as people with IDD got older, they expressed interest in learning more about relationships, dating, and intimacy:
Um, I think just because the general questions I may ask them during therapy sessions, like “How is school going?” Um some of the older kids, they bring up boyfriends and girlfriends spontaneously. So, I kind of ask questions about that. (Health care provider)
Sex Education as a Reactive Response
Other topics were initiated by parents, educators, and providers reactively because of concerns regarding safety or puberty (e.g., boundaries, consent, menstruation, masturbation, nocturnal emissions). One health care provider shared that “I think the most interaction I have with them is after there’s been an issue. So, I’m more a response team than proactive team.”
Theme 3: Recommendations for Sex Education
Participants suggested that SE can be improved by using (1) proactive, formal education with (2) multiple stakeholders and (3) continued learning.
Proactive, Formal Education
Participants suggested that SE be initiated proactively for people with IDD, before the onset of puberty. One parent said, “It is real important to take [SE] as early as possible.” Participants also suggested that formal educational standards be developed and implemented at a national level for students. Standards should also be developed for health care providers to address SHI for people with IDD. They felt that this would guarantee they would receive age-appropriate SHI in a developmentally appropriate way:
I think I alluded to [this] before, but it would be nice to know, like, legally. Because I don’t really know—[you should know] whether or not someone has a guardian [and whether] you’re still allowed to talk about this stuff. (Health care provider)
Multiple Stakeholders
Participants highlighted the importance of shared responsibility for providing SE to people with IDD; specifically, they reported the need to have an interdisciplinary team that addresses components of SE that relate to their disciplines and follow up with parents. As one educator put it, “I mean . . . it takes a village, and everyone should be able to nurture and support a child [in their SE].” They also suggested collaborating with other professionals to ensure all areas of SE are adequately addressed. One educator suggested that “a doctor come in . . . who could talk in detail about all the different birth control.”
Participants believed that if multiple stakeholders do not play their part, many people with IDD would go without the information they need to have safe, fulfilling relationships:
It needs to be discussed because there could be situations once they [are in a relationship], and if a person comes to them and tries to talk about [sexual activities] and they don’t know about it, it’s kind of not their fault. (Participant with IDD)
Continued Learning
Participants emphasized that, in addition to starting conversations at younger ages, SE should continue throughout the life span. They suggested that this population may be interested in romantic relationships at times different from those of their peers and that SHI may be more relevant at a later age. They also reported that people with IDD seem to benefit from repetition to improve accessibility of SHI. In fact, 1 educator felt this may be most important: “Frequent repetition [is helpful] to reinforce anything.” A parent echoed this for their own child: “You know, with [my child], a lot of [repetition] is better.” This highlights the necessity to continue providing SHI even beyond the school-age years and outside of education settings.
Discussion
In this study we sought to understand barriers to, the context of, and recommendations for SE. The results show that current practices are limited to conversations that are initiated by people with IDD or that are begun reactively. The current context for SE is impeded by values and cultural issues, parental attitudes toward their child’s sexuality, a lack of organizational policies and standards, and limited professional education or societal biases, which unintentionally oppress people with IDD because they inhibit the provision of comprehensive SE. Contrary to current practices, our participants recommended a proactive, formal education provided by multiple stakeholders across the life span. As Shuttleworth (2003) described,
In order for one to experience a sense of sexual well-being, one must also have access to the psychological, social and cultural supports that acknowledge and nurture sexuality and the individual’s right to sexual expression and to experience intimate relationships. (p. 6)
Values and cultural issues may be overcome by addressing the need for specific SE standards and guidelines for schools, health care providers, and organizations. In fact, SE policies in public education are associated with increased receipt of SE among adolescents (Rabbitte & Enriquez, 2019). A survey of nurses, educators, and administrators made it clear that stakeholders believe that community and organizational involvement is necessary when advocating for and securing SE (Dickson et al., 2020). Given that sexuality is a basic human right and that people with IDD face pervasive discrimination regarding their sexual health, it is particularly important that all stakeholders be involved in advocating for SE standards in education and health care settings.
As previously mentioned, sexual activity can be addressed by occupational therapy practitioners; however, few are educated as students about how to do so (Eglseder et al., 2018). Additional professional training may improve stakeholder comfort and delivery of SE to people with IDD; specifically, offering education about sexual health concerns among this population and clinical training to initiate these conversations may increase receipt of SE. One way this can be done is by training stakeholders to use either the Recognition Model, which draws on disability studies to address sexual health concerns with clients by first recognizing clients as sexual beings (Couldrick et al., 2010), or the Ex-PLISSIT Model, which educates health care providers on how to screen for and address concerns related to sexuality and aligns with a rights-based approach to SE in promoting clients’ occupational justice (Sakellariou & Algado, 2006; Taylor & Davis, 2006). Training on how to promote sexual citizenship and agency and overcome stigma is another important consideration for stakeholders involved in providing SE to people with IDD, including training on how to recognize and overcome their own biases. Education about how to help parents understand and see their children or young adults as sexual beings, as well as to help promote ownership and independence among people, may also help address barriers and promote overall sexual health (Krantz et al., 2016).
Policies and training will likely facilitate the provision of proactive, formal SE for people with IDD by multiple stakeholders, including occupational therapy practitioners. Occupational therapy practitioners can promote the accessibility of SHI in formal education settings with adolescents (Krantz et al., 2016). This education should draw on disability studies by promoting sexual citizenship and agency using a rights-based approach. Occupational therapy practitioners can also facilitate increased participation in occupations associated with one’s sexuality, including dating and intimacy, throughout the life span and across settings. This approach is important to encourage understanding and ensure that certain populations are receiving SHI at relevant times.
Limitations
This study is not without limitations. First, our sample was heterogeneous in nature and included few occupational therapy practitioners. Moreover, it is important to acknowledge the research team’s perspective as predominantly cisgender, heterosexual women without IDD. Future research should consider including more diverse identities as a part of the research team and recruiting larger, more specific samples of each stakeholder group.
Implications for Occupational Therapy Practice
The results of this study have the following implications for occupational therapy practice:
Occupational therapy practitioners should advocate for their hospitals, schools, and community settings to adopt standards for how to address SHI with all clients.
Educators should incorporate sexuality into the occupational therapy curriculum using a rights-based approach and including the Recognition Model and the Ex-PLISSIT Model.
Occupational therapy practitioners should not only focus on increasing participation in occupations associated with sexuality but also promote accessible SE with an emphasis on self-determination and self-advocacy as they pertain to sexuality and sexual citizenship (Wilkerson, 2002).
Conclusion
This study has revealed that current SE is either initiated by people with IDD or offered reactively, likely as a result of the four barriers described by key stakeholders: values and cultural issues, parental attitudes toward their child’s sexuality, a lack of organizational policies and standards, and limited professional education or societal biases. Our participants offered recommendations, including using a proactive, formal education that is provided by multiple stakeholders and continues throughout adulthood, that occupational therapy practitioners can embed in their work by advocating for standards, educating students, and addressing occupations related to sexuality across the life span.
Footnotes
Acknowledgments
This study was funded by the Coca-Cola Critical Difference for Women Research Grant from The Ohio State University’s Department of Women’s, Gender and Sexuality Studies. The authors have no conflicts of interest.
We use person-first language throughout this article to respect the majority opinion of people with IDD (Liebowitz, 2015).