
Abstract
Opportunities exist to expand the interventions used in occupational therapy to successfully address puberty-specific challenges among adolescents with ASD.
Adolescence (ages 8–16 yr) is marked by rapid physical, neurodevelopmental, and social–emotional changes (Eunice Kennedy Shriver National Institute of Child Health and Human Development, 2016; U.S. National Library of Medicine, 2020; World Health Organization, 2020). Although all adolescents must navigate these puberty-related changes, people with autism spectrum disorder (ASD) experience increased difficulty doing so (Beddows & Brooks, 2016). Because they struggle to accurately interpret and respond to social cues, they experience difficulty adapting to physical and emotional changes, managing new hygiene routines, and abiding by social norms (Cridland et al., 2014, 2015).
Puberty-related occupational performance challenges for adolescents with ASD include coping with puberty, menstruation, masturbation, personal hygiene, family routines, safety, emotional regulation, behavior management, and social participation (Bagatell, 2016; Ballan, 2012; Beddows & Brooks, 2016; Cridland et al., 2014, 2015; Hellemans et al., 2007; Holmes et al., 2016; Pecora et al., 2016). Cridland et al. (2014) illustrated caregivers’ apprehensions when anticipating pubertal changes and behaviors. In addition, Bagatell (2016) found that the onset of puberty brought on increased challenges and changes to the occupational and daily routines of the individual as well as the family. Beddows and Brooks (2016) identified a high prevalence of inappropriate sexual behaviors among adolescents with ASD, such as inappropriate arousal, exhibitionism, and offenses. Male adolescents with ASD were found to have challenges with hypermasturbation (masturbation so frequent it causes physical harm or interferes with daily functioning), masturbation in inappropriate settings, and use of inappropriate objects (Bagatell, 2016). Mothers of female adolescents with ASD reported that menstruation was the greatest puberty-related concern with their daughters (Cridland et al., 2014).
Occupational therapy is the second most common service that adolescents with ASD receive to support occupational performance skills, such as social interaction, self-care, and home management, and contextual factors, including consistency of routines and sensory environments (Tomchek et al., 2010). Specific examples may include a female adolescent starting menstruation and having increased difficulty managing hygiene routines or challenges with feminine products and bras secondary to sensory processing difficulties. Another example is a male adolescent having increased challenges determining socially appropriate places for masturbation or using appropriate comments in social situations. Although these challenges exist, puberty-specific challenges and best practice interventions used to address these challenges with people who have ASD remain undocumented in the occupational therapy literature.
Despite systematic reviews completed between 2006 and 2013 to identify effective occupational therapy interventions to support people with ASD (Tanner et al., 2015; Watling & Hauer, 2015; Weaver, 2015), none were specific to puberty-related challenges. However, the literature does provide evidence of the most common interventions used by occupational therapy practitioners working with people who have ASD and the most common interventions used by various disciplines to address puberty-related challenges that are within the scope of occupational therapy. Interventions within the scope of occupational therapy include behavioral strategies (McDonald & Machalicek, 2013; Weaver, 2015), behavioral skills training specifically incorporating applied behavioral analysis (Ballan & Freyer, 2017; Matson et al., 2012; Veazey et al., 2015), cognitive strategies (Tanner et al., 2015; Weaver, 2015), social learning approaches (Ballan & Freyer, 2017; Klett & Turan, 2012; Mathews et al., 2013; McDonald & Machalicek, 2013; Tanner et al., 2015), technology (Bimbrahw et al., 2012; McDonald & Machalicek, 2013; Tanner et al., 2015; Weaver, 2015), Ayres Sensory Integration® (ASI) treatment (Watling & Hauer, 2015), sensory processing integration (Watling & Hauer, 2015; Weaver, 2015), exercise (McDonald & Machalicek, 2013; Tanner et al., 2015; Weaver, 2015), parent training approaches (McDonald & Machalicek, 2013; Weaver, 2015), hippotherapy (Ajzenman et al., 2013), and curricula for puberty education (Corona et al., 2016; Jamison & Schuttler, 2017; Visser et al., 2017).
Understanding the practice patterns of occupational therapy practitioners provides a baseline to evaluate current practice to determine needs for the advancement of effective interventions for addressing puberty-related challenges. Therefore, the purpose of this study was to identify what puberty-related challenges occupational therapy practitioners address and what interventions are provided.
Method
Research Design
A nonexperimental survey design was used to explore puberty-related challenges addressed by practitioners and interventions used with adolescents ages 8–16 yr with ASD. University of North Dakota institutional review board approval was received, and informed consent procedures were followed.
Participants
Inclusion criteria for participation were being an occupational therapy practitioner in the United States working with people who were diagnosed with ASD between ages 8 and 16 yr. Three recruitment methods were used: (1) mailing postcards to a stratified random sample of 500 practitioners from American Occupational Therapy Association (AOTA) Developmental Disabilities, Sensory Integration, and Early Intervention and School Systems Special Interest Sections; (2) convenience sampling by posting in four AOTA OTConnections blog posts; and (3) convenience sampling by emailing 106 pediatric fieldwork coordinators to forward to practitioners from the University of North Dakota database. In total, 606 participants were directly invited, and 71 participants were included in the analysis, for an estimated response rate of 11.72%.
Instrumentation
After an extensive literature review, we developed a survey—the Occupational Therapy–Autism and Puberty Survey—that identified the challenges experienced by adolescents with ASD, the interventions used by occupational therapy practitioners when working with adolescents who have ASD, and the interventions for which practitioners received training or education within the past 10 yr (the survey is available online with this article at https://ajot.aota.org).
The survey first presented nine challenges, including coping with puberty, menstruation, masturbation, personal hygiene, family routines, safety, emotional regulation, behavior management, and social participation. Thereafter, each challenge offered five to nine subchallenges for practitioners to identify as being addressed in their practice or not (Table 1). Finally, for each of the nine challenges, participants were asked to identify intervention approaches used from 11 options, including behavioral strategies (reinforcement, positive behavioral supports, picture prompts, visual supports and aids, activity schedule), behavioral skills training (incorporating applied behavioral analysis), cognitive strategies (CO-OP: goal–plan–do–check, joint attention training), social learning approaches (social stories, modeling, peer mediation, social skills training), technology (iPhone, iPad, iPod, self-prompting personal device assistant, computer-based interventions), ASI, sensory processing integration, exercise, parent training approaches, hippotherapy, and curricula for puberty education.
Prevalence of Reported Puberty-Related Subchallenges Addressed With Adolescents With ASD by 71 Occupational Therapy Practitioners
Note. ASD = autism spectrum disorder.
Average percentage of 6 challenges chosen = 66.43%. bAverage percentage of 8 challenges chosen = 47.36%. cAverage percentage of 6 challenges chosen = 40.85%. dAverage percentage of 8 challenges chosen = 40.69%. eAverage percentage of 4 challenges chosen = 40.56%. fAverage percentage of 6 challenges chosen = 35.61%. gAverage percentage of 4 challenges chosen = 25.63%. hAverage percentage of 5 challenges chosen = 24.51%. iAverage percentage of 4 challenges chosen = 18.87%.
The development of the survey did not include expert review, pilot studies, or procedures to establish psychometrics. However, internal consistency reliability was high for questions regarding both challenges and interventions, with Cronbach’s α at .90 and .92, respectively. Participants accessed the survey using the Qualtrics (Provo, UT) online platform through a direct link or quick response code available October 2017 through January 2018.
Data Analysis
Descriptive statistics were used (frequencies and percentage of total choices) for each challenge addressed and intervention used. The percentage of practitioners who selected each subchallenge within a challenge was also recorded to describe the composition of each challenge. We then found the percentage of practitioners who used each of the 11 named interventions for a specific challenge, and participants were asked to indicate which of the 11 interventions they received training in. Using a z test for difference in proportions, we compared the percentage of participants who were trained in an intervention with the percentage of participants who used the intervention. Any missing values in a variable were deleted in a listwise fashion, causing that participant with unknown values to not be used for that analysis. SAS software (Version 9.4; SAS Institute, Cary, NC) and an α of .05 were used for all tests.
Results
Of the 71 participants, 88.7% were occupational therapists (n = 63) and 11.3% were occupational therapy assistants (n = 8). Nearly all were female (n = 68; 95.8%) and identified as White (n = 68; 95.8%). More than one-third resided in Minnesota (n = 15; 21.1%) or North Dakota (n = 11; 15.5%). The average number of years in occupational therapy was 15.63 (SD = 11.41), with one-third having less than 10 yr. The average years working in pediatrics was 13.28 (SD = 10.64), with one-third having less than 6 yr, and about half spent one-fourth or less of their time working with adolescents who have ASD. Although participants were well distributed in terms of age and years in occupational therapy, this distribution was by chance because the sample was not stratified in this manner.
Challenges
Table 1 presents each challenge and the percentage of respondents who addressed that challenge with youth. The challenges addressed by more practitioners were emotional regulation (66.4%), personal hygiene (47.4%), behavior management (40.9%), social participation (40.7%), and family routines (40.6%). The challenges addressed by fewer practitioners were menstruation (18.9%), safety (24.5%), and masturbation (25.6%). It is noteworthy that practitioners addressed subchallenges such as genital cleansing, sexual behavior, interaction with the opposite sex, and sexual comments the least (for more examples, see Table 1).
Interventions
Occupational therapy practitioners reported using the 11 interventions across all challenges: behavioral strategies (used by 93.0%), social learning approaches (91.5%), behavioral skills training incorporating applied behavioral analysis (85.9%), sensory processing integration (67.6%), exercise (63.4%), parent training approaches (60.6%), cognitive strategies (46.5%), technology (42.3%), ASI (29.6%), curricula specifically designed for puberty education (7.0%), and hippotherapy (7.0%). Figure 1 illustrates how many practitioners reported using each intervention for each challenge, and Table 2 provides specific percentages for each challenge and intervention. Behavioral strategies and social learning approaches were the two most common interventions across all nine challenges. More than 40% of participants used these two interventions for all challenges except for safety and masturbation. Parent training was the third most common intervention used to address family routines (45.1%), personal hygiene (42.3%), coping with puberty (35.2%), safety (23.9%), masturbation (18.3%), and menstruation (18.3%). Sensory processing integration was the third most common intervention for emotional regulation (59.2%) and behavior management (54.9%). More than 40% of participants used exercise to address emotional regulation and behavior management. Equine-assisted therapy and curricula specific to puberty education were least likely (<10%) to be used across all challenges.
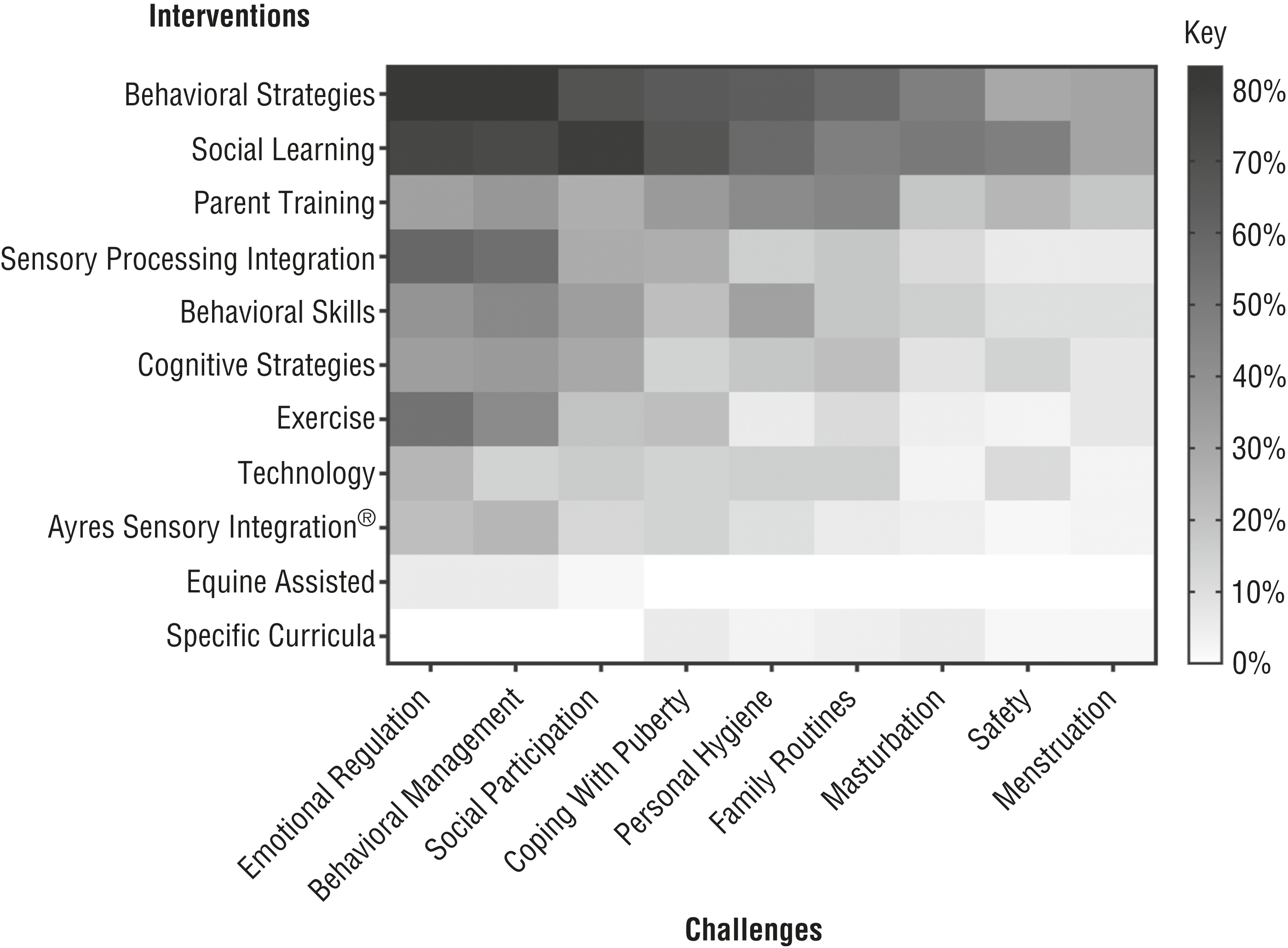
Visual representation of reported use of interventions for specific challenges by 71 occupational therapy practitioners.
Percentage of Participants (N = 71) Who Reported Use of Each Intervention for Each Challenge
Training
Practitioners most commonly reported receiving education in behavioral strategies (94%), sensory processing integration (82%), and social learning approaches (80%); they least commonly reported receiving education in curricula designed for puberty education (3%), hippotherapy (13%), and parent training (35%). Figure 2 represents the association between reported education in and use of each intervention by practitioners. Eight interventions had no significant difference in reported education and use. Significantly more respondents reported using behavioral skills training incorporating applied behavioral analysis (z = 5.07, p < .001) and parent training (z = 3.01, p = .002) than having received education in these interventions. In contrast, significantly more respondents reported having received education in technology-based interventions than actually using this type of intervention (z = 2.76, p = .003).
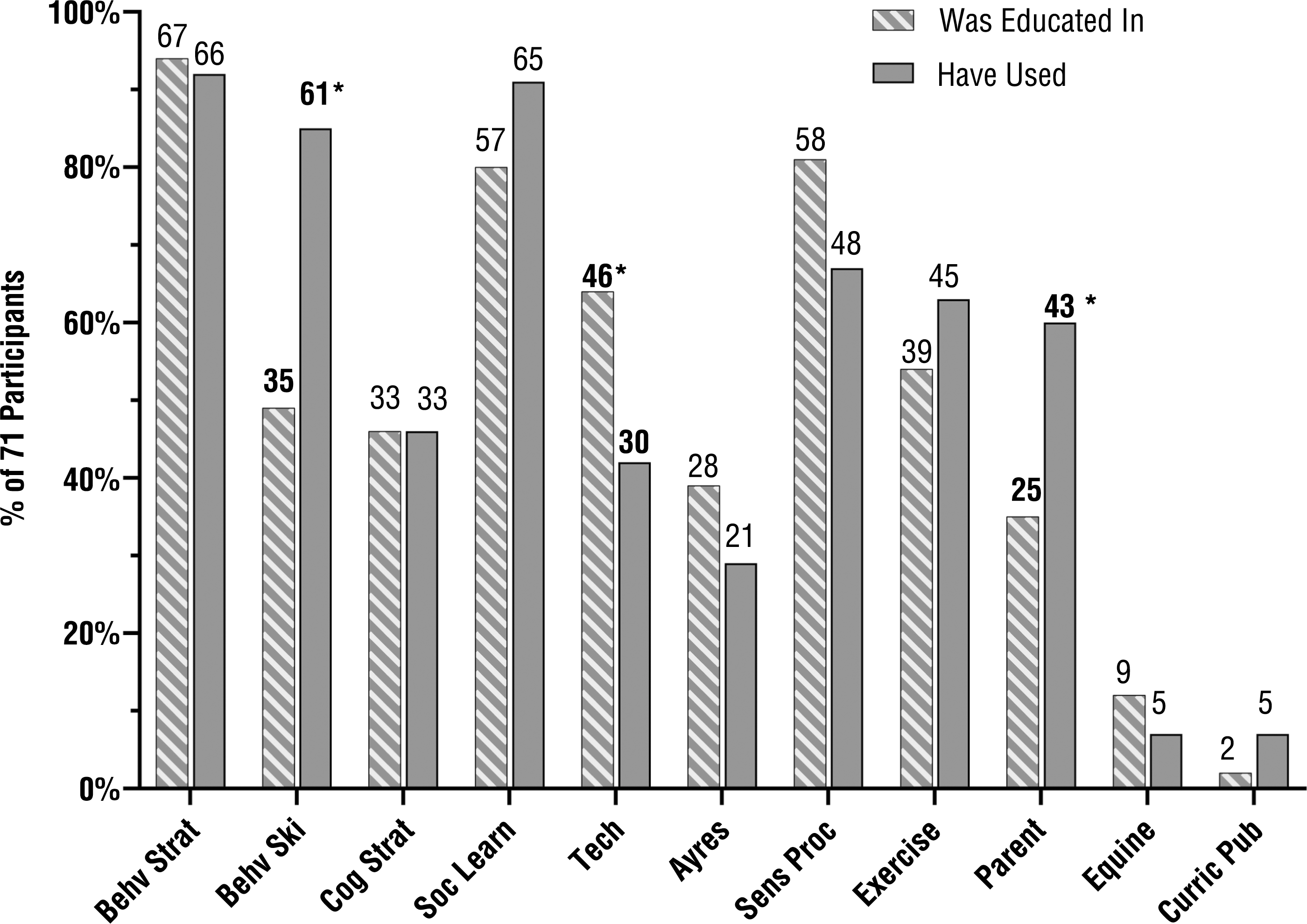
Percentage and frequency of reported education in and use of each intervention by 71 occupational therapy practitioners.
Discussion
More practitioners in our sample addressed the challenges of emotional regulation, personal hygiene, behavior management, social participation, and family routines, which is consistent with the occupational therapy literature for individuals with ASD (Scott, 2011; Tanner et al., 2015; Tomchek et al., 2010). Fewer practitioners addressed the puberty-specific challenges of menstruation and masturbation (Bagatell, 2016; Cridland et al., 2014). Additionally, when looking at the challenges being addressed, puberty-specific subchallenges—such as genital cleansing, sexual behavior, exhibitionism, interaction with the opposite sex, sexual comments, and sex-specific maturation—were addressed by fewer practitioners (Beddows & Brooks, 2016). Therefore, these results show that practitioners may be neglecting to address puberty-specific challenges that adolescents with ASD experience.
Consistent with interventions supported by the literature, practitioners used behavioral strategies and social learning approaches to address puberty-related challenges (Ballan & Freyer, 2017; McDonald & Machalicek, 2013). Practitioners used other interventions supported by the literature to address challenges: behavioral skills training incorporating applied behavioral analysis to address behavior management, emotional regulation, social participation (Ballan & Freyer, 2017), and personal hygiene (Veazey et al., 2015); cognitive strategies for social participation (Tanner et al., 2015); technology to address social participation (McDonald & Machalicek, 2013; Tanner et al., 2015) and personal hygiene (Bimbrahw et al., 2012); and exercise to address emotional regulation and behavior management (Tanner et al., 2015; Weaver, 2015). Few practitioners used evidence-based curricula to address puberty-specific challenges such as self-care skills, appropriate social skills, developing relationships, and psychosexual awareness (Corona et al., 2016; Jamison & Schuttler, 2017; Visser et al., 2017).
Practitioners reported recent education or training in three of the four interventions most commonly used to address puberty-related challenges—behavioral strategies, social learning approaches, and sensory processing integration—which are well documented in the occupational therapy literature and academic textbooks. However, it is concerning that practitioners reported significantly less education in parent training strategies and behavioral skills training incorporating applied behavioral analysis. Practitioners should be educated in interventions used in practice to ensure accuracy and increase successful and positive outcomes. In contrast, practitioners reported significantly less use of than education in technology-based approaches. Computerized devices have been shown to assist with skills required for activities of daily living and instrumental activities of daily living for people with ASD (Bimbrahw et al., 2012; Weaver, 2015). Therefore, gaps exist between practitioner education, practice patterns reported, and use of evidence-based strategies when addressing puberty-related challenges.
The findings from the study provide a baseline understanding of puberty-related challenges addressed and interventions used by practitioners when working with adolescents who have ASD. Further consideration is needed to fully understand these findings and how they affect practice. Several factors may contribute to these findings, such as currently available publications, practitioner education and training, and practitioner experience and level of comfort, as well as cultural context and caregiver goals.
Limitations
Instrumentation was the first limitation of this study because the survey lacked psychometric rigor. Participation limitations included lack of diversity, limited number of participants, and a large portion of respondents being from North Dakota and Minnesota. This sample limits generalizability of the study’s findings because results could vary between different regions or populations because of various factors, including, but not limited to, educational backgrounds (i.e., regional universities or occupational therapy programs), cultural beliefs, or social norms. Additionally, the questionnaire did not go through procedures to establish psychometric properties or expert review before deployment. Finally, the scope of the survey did not allow us to investigate whether each challenge was a current need for practitioners’ adolescent clients with ASD that was going unaddressed, or whether the challenges were being addressed by another discipline; the survey also did not include questions related to the effectiveness of the provided interventions.
Implications for Occupational Therapy Practice
On the basis of the findings of this study, we recommend the following measures for occupational therapy practice:
Training programs on how to effectively address puberty-specific challenges to maintain occupational therapy’s role in addressing the needs of adolescents with ASD
Development of an effective occupation-based curriculum to assist practitioners in addressing puberty-specific challenges
Further research to identify the barriers to addressing puberty-specific challenges and implementation of specific interventions
Further research on the effectiveness of specific interventions within the scope of occupational therapy to address puberty-specific challenges for adolescents with ASD.
Conclusion
The adolescent transition of puberty comes with many challenges that can affect occupational performance. This study provides a basic understanding of puberty-related challenges addressed and associated interventions used by occupational therapy practitioners with adolescents with ASD. Identification of barriers that practitioners face when addressing puberty-specific challenges would more fully serve adolescents and their families.