
Abstract
A 4-hour experiential boot camp was found to increase students’ capacity and confidence for delivering wheelchair skills training to future clients.
Wheelchair skills training is one of eight essential best practice steps in manual wheelchair (MWC) service provision (World Health Organization, 2008). Comprehensive structured training, such as the Wheelchair Skills Training Program (WSTP; Dalhousie University, 2012), improves skill capacity and self-efficacy in MWC users (MacPhee et al., 2004; Sakakibara et al., 2013), which, in turn, positively affect participation, quality of life, and safety (Hosseini et al., 2012; Lemay et al., 2012). Despite the potential benefits, skills training is often inadequate or absent in clinical practice among occupational therapy practitioners (Best, Routhier, & Miller, 2015; Kirby et al., 2015).
Among the barriers identified as contributing to this practice gap are limited knowledge, capacity, and confidence to demonstrate and train MWC mobility skills as well as perceptions of limited potential for clients to acquire advanced skills (Giesbrecht et al., 2015). Evidence suggests that occupational therapy practitioners typically receive insufficient preparation to deliver MWC skills training during their entry-to-practice professional education. A 2015 survey of 11 accredited Canadian occupational therapy programs reported that 36% did not incorporate MWC skills training in their curricula; among programs that did, only 29% used a validated approach incorporating advanced mobility skills (e.g., WSTP; Best, Miller, & Routhier, 2015).
Emerging evidence suggests that providing experiential training through an MWC boot camp can have a considerable impact on occupational therapy students’ skill capacity and self-efficacy (Coolen et al., 2004; Giesbrecht et al., 2015; Kirby et al., 2011; Rushton & Daoust, 2019). The boot-camp format integrates pedagogical elements of Kolb’s (1984) Experiential Learning Theory, such as concrete learning strategies that contextualize experiences and promoting self-reflection on application to clinical practice (Coker, 2010; Knecht-Sabres, 2013). Concurrently acquiring MWC performance skills while conducting assessment and intervention may contribute to consolidation of learning. Although the reported boot-camp benefits are encouraging, little evidence exists to confirm that improvements are sustained. Coolen et al. (2004) reported retention of skill capacity among occupational therapy students 9 to 12 mo after boot camp but only in a subset of participants (8 of 22). Research to date has focused only on students’ capacity and self-efficacy in MWC use rather than their MWC service delivery skills with clients. This gap in knowledge is critically important in optimizing professional education programs.
The following research questions were addressed in this study:
Does boot-camp participation improve skill capacity; self-efficacy in MWC use; and self-efficacy with assessing, training, spotting, and documenting MWC skills?
Is improvement retained after 4 mo?
What boot-camp factors do participants perceive as positively affecting future clinical practice?
We hypothesized that there would be significant improvements in all outcomes, and improvements would be retained at follow-up.
Method
A mixed-methods design implemented concurrent embedded data collection with a quantitative emphasis (Creswell, 2003). A repeated-measures, within-groups approach used quantitative data collection before (Time 1 [T1]) and after (Time 2 [T2]) a 4-hr comprehensive MWC skills training boot camp, and again at 4-mo follow-up (Time 3 [T3]), when a qualitative questionnaire was also administered. At follow-up, participants were still students but had completed their penultimate fieldwork placement.
Participants were recruited from a convenience sample of all second-year master’s students in occupational therapy attending a compulsory boot camp. Advertisement was done via posters, social media postings, and a brief in-class presentation by a classmate (a student coinvestigator). Participants provided written consent to complete questionnaires and were assigned an identification (ID) number to maintain confidentiality. Ethical approval was obtained from the University of Manitoba Research Ethics Board. Questionnaires were completed within 1 wk of distribution at T2 and T3, and all questionnaires were identifiable only by ID number.
Procedure
The boot camp is a 4-hr concentrated experiential learning workshop embedded in the wheelchair service delivery component of a compulsory advanced clinical skills course. Principles of MWC use, safety, and motor learning are previewed in an online tutorial. An expert instructor hosts four to five student pairs, sequentially providing demonstration and verbal instruction. Students alternate performance and training roles with each skill, from basic to advanced, as per the WSTP (Dalhousie University, 2012). The trainer uses task analysis and clinical reasoning to assess their partner’s performance and to provide appropriate direction. Instructors circulate, providing strategic feedback on performance as well as assessment and training approaches.
Measures
The Wheelchair Skills Test–Questionnaire (Version 4.2; WST–Q) is a well-established, self-administered measure of skill performance capacity (Dalhousie University, 2013). A total score (0–64) is obtained by summing 32 skill items (each scored 2 for “yes”; 1 for “yes, with difficulty”; or 0 for “no”) and converting the total to a percentage (0%–100%). The WST–Q has demonstrated strong internal consistency (Cronbach’s α = .90) and test–retest reliability (intraclass correlation coefficient [ICC] = .78; Rushton et al., 2016) as well as high concurrent validity with objective capacity evaluation (ρ = .89; Rushton et al., 2012).
The Self-Efficacy in Assessing, Training, and Spotting (SEATS) test is a self-report questionnaire evaluating confidence in provision of MWC training services (Rushton et al., 2019). Test items are rated on a 5-point Likert scale ranging from 1 (not at all confident) to 5 (completely confident). Three subscales, each composed of the same 32 items from the WST–Q, address Assessment (SEATS–A), Training (SEATS–T), and Spotting (SEATS–S). The Documentation (SEATS–D) subscale includes five items related to documentation. The SEATS has demonstrated excellent internal consistency (Cronbach’s α = .90–.97) as well as good reliability (ICC = .81–.95) and responsiveness (smallest real difference = 6.2%–8.2%) for all subscales (Rushton et al., 2019).
The short form of the Wheelchair Use Confidence Scale (WheelCon) is a self-report questionnaire assessing self-efficacy with MWC use (Sakakibara et al., 2015). Confidence performing MWC-related activities is rated on an 11-point Likert scale ranging from 0 (not confident) to 10 (completely confident). The 21-item total score (WheelCon–T) subsumes two subscales: Mobility (WheelCon–M: 13 items) and Self-Management (WheelCon–S: 8 items). Good internal consistency reliability has been demonstrated (Cronbach’s α ≥ .70; Sakakibara et al., 2015), as has high test–retest reliability (ICC = .98) with an Italian translation (Berardi et al., 2018).
Investigators composed three open-ended questions asking participants to provide their perceptions of how the boot-camp experience affected their confidence with MWC skills training provision in clinical practice (Appendix A). Question construction was informed by Kolb’s (1984) Experiential Learning Theory (Knecht-Sabres, 2013).
Data Analysis
A repeated-measures, within-subjects analysis of variance (ANOVA), with time as the within-subjects factor, was conducted for each measure to detect change across data collection points (p < .05). For retention, post hoc analyses were run with T2 and T3 scores. Retention was assumed if no significant difference (p > .05) or a significant improvement was found. Cohen’s d effect sizes were calculated for pairwise comparisons, and ηp2 was computed for ANOVA. Effect size interpretation was based on Cohen (1988). A directed content analysis approach was used for qualitative data (Hsieh & Shannon, 2005).
Before analysis, a preliminary thematic framework was constructed that articulated the pedagogical components of the learning experience and participants’ reflection on self-efficacy in applying their learning in clinical practice (Coker, 2010). Three student coinvestigators, who received qualitative analysis training and supervision from the principal investigator, independently coded questionnaires to parse unique concepts; emergent themes were collaboratively developed by coalescing the coded content. Quantitative and qualitative findings were integrated into a summary matrix of overarching themes (Creswell, 2003). To promote trustworthiness, the investigators documented a detailed audit trail. Triangulation was used with four investigator perspectives to promote debate and to achieve a consensus during data coding, analysis, and interpretation (Ohman, 2005). Overall cohesion and absence of outliers or emergent concepts after coding suggested data saturation.
Results
Among 44 eligible boot-camp attendees, 42 (95.5%) enrolled in the study. All measures except for SEATS–T, SEATS–S, and SEATS–D were corrected for sphericity with the Greenhouse–Geisser procedure. ANOVA results indicated statistically significant improvement in scores with large effect sizes for all three measures (Table 1). Post hoc analyses revealed a significant increase from T1 to T2 for all measures and subscales (Table 2). At follow-up, WST–Q scores had decreased significantly (p < .001), indicating that T2 capacity scores were not maintained. The WheelCon–T and WheelCon–S showed a statistically significant increase, indicating that scores had been maintained and improved further by T3. The remaining measures did not demonstrate significant change, indicating that they were also maintained at follow-up.
ANOVA Summary With Time as the Within-Subjects Factor
Note. Effect size interpretation of ηp2 values: small ≥ .01, medium ≥ .06, and large ≥ .14 (Cohen, 1988). ANOVA = analysis of variance; SEATS–A = Self-Efficacy in Assessing, Training, and Spotting test–Assessment subscale; SEATS–D = Self-Efficacy in Assessing, Training, and Spotting test–Documentation subscale; SEATS–S = Self-Efficacy in Assessing, Training, and Spotting test–Spotting subscale; SEATS–T = Self-Efficacy in Assessing, Training, and Spotting test–Training subscale; WheelCon–M = Wheelchair Use Confidence Scale–Mobility subscale; WheelCon–S = Wheelchair Use Confidence Scale–Self-Management subscale; WheelCon–T = Wheelchair Use Confidence Scale–total score; WST–Q = Wheelchair Skills Test–Questionnaire.
Mean Values and Post Hoc Analyses for All Outcome Measures
Note. Values in bold indicate statistically significant results. Mean scores are out of a total of 100 (WST), 10 (WheelCon), or 5 (SEATS). CI = confidence interval; Diff = difference; SEATS–A = Self-Efficacy in Assessing, Training, and Spotting test–Assessment subscale; SEATS–D = Self-Efficacy in Assessing, Training, and Spotting test–Documentation subscale; SEATS–S = Self-Efficacy in Assessing, Training, and Spotting test–Spotting subscale; SEATS–T = Self-Efficacy in Assessing, Training, and Spotting test–Training subscale; T1 = Time 1; T2 = Time 2; T3 = Time 3; WheelCon–M = Wheelchair Use Confidence Scale–Mobility subscale; WheelCon–S = Wheelchair Use Confidence Scale–Self-Management subscale; WheelCon–T = Wheelchair Use Confidence Scale–total score; WST–Q = Wheelchair Skills Test–Questionnaire.
Three broad themes emerged from the qualitative analysis: knowledge acquisition, experiential learning, and client empathy (Figure 1). The following boot-camp factors were identified as the most effective in building participants’ self-efficacy in assessing, training, and spotting (in descending order): opportunity to practice skills, experience of doing skills, the environment (safe and supportive), the instructors (knowledgeable and encouraging), spotting (being spotted and being a spotter), working in pairs, grading of skills, and feedback (giving and receiving). The following factors were identified by participants as the most influential on their self-efficacy and capacity to provide MWC skills training (in descending order): experience and ability to perform skills, time to practice, resources to consult, and previous experience.
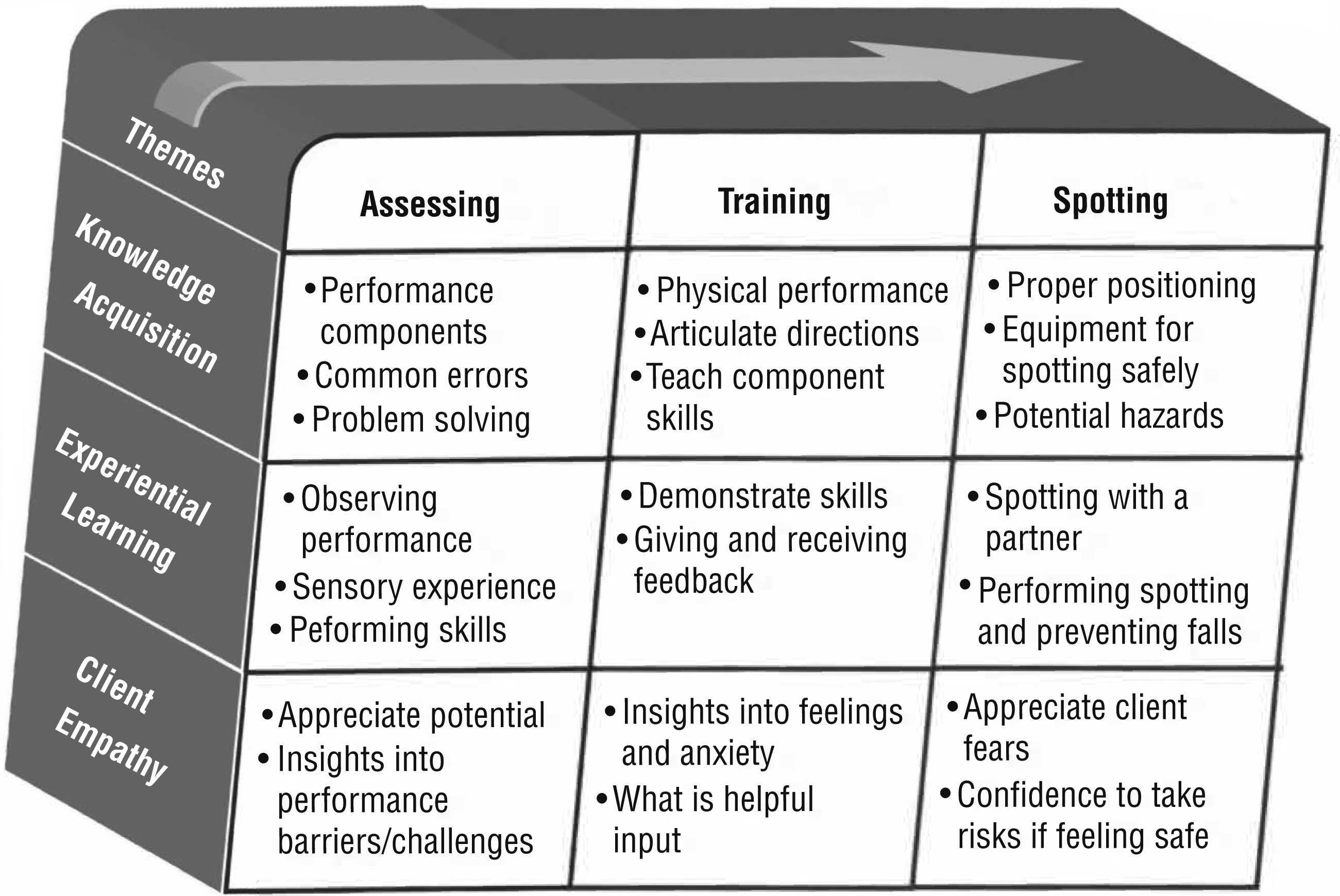
Summary of themes reflecting the impact of boot camp on clinical practice.
Discussion
Our findings provide evidence to support the immediate and sustained impact of comprehensive wheelchair skills training on clinical skills among occupational therapy students. Improvements on all measures between baseline and postintervention confirm our first hypothesis, that a boot-camp delivery format is an effective means of enhancing students’ skill capacity, self-efficacy in skill performance, and self-efficacy in the delivery of MWC training. The statistically significant improvement of nearly 40% in skill capacity is similar to results reported by Giesbrecht et al. (2015), who used a comparable intervention (39%), and Rushton and Daoust (2019), who compared boot-camp (37%) and distributed-practice (29%) approaches.
Similarly, a statistically significant 26% improvement in self-efficacy with skill performance is consistent with other studies of boot-camp intervention, in which results ranged from 28% to 30% (Giesbrecht et al., 2015; Rushton & Daoust, 2019). Statistically significant improvements of self-efficacy in delivering wheelchair services are similar to those of Rushton and Daoust (2019), with slightly larger improvements in training (32.4% vs. 26.7%), assessment (38.1% vs. 33.0%), and spotting (40.8% vs. 35.6%), whereas documentation had slightly lower improvement (26.9% vs. 31.7%). Moreover, postintervention scores are very similar between studies, suggesting that participants achieved comparably high ratings of self-efficacy (70%–90%) in their delivery of wheelchair-related services.
Beyond confirming the initial impact of consolidated training, this is the first study to evaluate retention of these benefits. A small but statistically significant decrease in skill capacity was reported at follow-up (approximately 5%). Slight performance declines might be expected, given that T2 data collection was conducted immediately after training, whereas T3 followed a 4-mo period during which participants may not have used these skills. Despite this time frame, participants’ skill capacity was still notably higher than at baseline and nearly identical to those reported immediately after boot camp in another study (Rushton & Daoust, 2019). Retention of performance self-efficacy suggests that participants felt competent in demonstrating MWC skills. This outcome is important clinically because occupational therapy practitioners have previously identified lack of skill and confidence as limitations in providing comprehensive training (Best, Routhier, & Miller, 2015).
This is the first study to evaluate retention of self-efficacy in clinical skills of wheelchair service delivery. Participants retained post–boot camp improvements on all four components of the SEATS test. The findings are encouraging. First, they suggest that the MWC boot camp is pedagogically sound in teaching students how to teach skills, in addition to performing the skills themselves. Second, improved self-efficacy in clinical skills was sustained beyond the immediacy of the boot camp. Third, high self-efficacy reported on the SEATS test suggests that study participants are more likely to implement comprehensive wheelchair training with their future clients (Rushton & Daoust, 2019). Although self-efficacy was high on all four components, SEATS–D scores were somewhat lower. Because participants identified experiential learning and time to practice as the most influential factors in increasing self-efficacy in other domains, greater focus on documentation during future boot camps may garner comparable improvements.
Participants’ responses to the qualitative questionnaire provided a fuller appreciation for how the boot camp was successful in contributing to their confidence in the delivery of clinical services. Three emergent themes were revealed: knowledge acquisition (the training content), experiential learning (the training process), and client empathy (insights into application). Participants reported that the boot camp provided concrete knowledge about the motor demands, sequencing, and timing required to successfully perform mobility skills. Understanding these components allowed them to assess barriers to performance, diagnose an appropriate training intervention, and ensure they could safely spot and supervise clients. Participants reported that the boot camp’s problem-solving approach promoted assessment of performance barriers, enabling targeted intervention and training strategies. The boot camp also explicitly addressed teaching strategies, such as motor learning principles and provision of appropriate feedback (Morgan et al., 2017; Wulf et al., 2010). Participants identified that learning how to teach MWC skills was also a critical component to instilling confidence in their clinical abilities.
The experience of learning through performance of MWC skills proved to be an important contribution to self-efficacy. Physical and sensory information derived while attempting MWC skills is helpful in translating abstraction into practice. Participants were able to anticipate and hypothesize performance barriers (i.e., assessment) and propose adaptive responses to correcting performance (i.e., training) because they had experiential knowledge and memory rather than just cognitive knowledge of instruction. Moreover, the trial-and-error experience (knowledge of outcomes), awareness of feedback structure and frequency, experience of both providing and receiving feedback, and reflection on the training experience seem to have contributed to their confidence in delivering training. The experiential learning approach is likely a contributing factor because research related to experiential learning with occupational therapy students has demonstrated improvements in both skill development and clinical reasoning (Coker, 2010; Knecht-Sabres, 2013).
Participants also highlighted insights into the “client experience” of learning to use an MWC, which generated a greater sense of empathy during their trainer role. Participants became increasingly aware of the time and practice required to integrate motor skills safely and efficiently. The amount, frequency, and type of feedback provided to clients were affected by their personal experience with learning. In addition, participants recognized the anxiety inherent in attempting skills with a higher risk for tipping and falling and how this anxiety can be allayed (for both client and trainer) with good communication and spotting technique. Many participants articulated that their own successful experience of learning to perform skills, in particular more advanced ones, altered their perceptions about what clients might be capable of learning and shattered previously held limiting stereotypes.
Study Limitations
Demographics were not collected, but participants were predominantly women in their early to mid-20s. Investigators included colleagues and an instructor, which may have influenced participation and positive response bias. To minimize this bias, the instructor was not involved in recruitment or enrollment, and data collection was anonymized. Although this is the first study to evaluate retention of both wheelchair skill (capacity and self-efficacy) and service delivery (self-efficacy), the follow-up period was limited to 4 mo. This time frame is likely sufficient to capture any natural decline after initial training; however, we were pragmatically incapable of following this cohort into their practice careers, and the persistence of positive outcomes beyond graduation cannot be assumed. Outcome measures were all subjective self-report, although the WST–Q is highly correlated with the objective WST version (Rushton et al., 2012).
Implications for Occupational Therapy Education
For occupational therapy professional programs, a boot-camp approach leverages experiential learning as an alternative strategy to deliver content on wheelchair service provision. The findings of this study have the following implications for occupational therapy education:
Use of a boot-camp approach effectively increases students’ capacity and confidence in performing MWC skills.
Improving MWC skill capacity and self-efficacy as a student increases their confidence in clinical service delivery will affect future practice.
Using a peer training approach develops both assessment and intervention skills.
The boot-camp approach might be further enhanced by better integration of documentation learning.
Conclusion
This study is the first to document improvement and retention of occupational therapy students’ MWC skill capacity and self-efficacy, as well as their self-efficacy in assessing, training, spotting, and documenting wheelchair skills, with clients after an MWC skills training boot camp. Statistically significant improvements were found in all outcomes, with large effect sizes. Self-efficacy for personal skill performance, as well as for assessing, training, spotting, and documenting skills with clients, were all retained or improved further at follow-up. Participants identified acquisition of new knowledge, the experiential training milieu, and a new appreciation for the client experience as important factors that contributed to improvements in clinical practice. This finding provides new evidence for the long-term benefit of comprehensive MWC skills training for rehabilitation professionals as part of their entry-to-practice education.
Footnotes
Acknowledgments
We gratefully acknowledge Jason Robillon, who participated in data collection and initial data analysis.
Qualitative Questionnaire Administered at Follow-Up
Please answer the following questions about developing your confidence to provide assessment, training, and spotting of manual wheelchair skills with clients in clinical practice.