
Abstract
The ICF Core Sets for schizophrenia were validated from the perspective of occupational therapists and found to be potentially useful tools for clinical practice.
Schizophrenia is a severe psychiatric Disorder characterized by alternating periods of stability and exacerbation of symptoms, including positive symptoms (e.g., hallucinations, thought disorders), negative symptoms (e.g., listlessness, apathy), and cognitive deficits (American Psychiatric Association, 2013; World Health Organization [WHO], 2001). Although schizophrenia has a low worldwide prevalence (Baxter et al., 2013), it is considered a highly disabling mental illness (Vos et al., 2016) because people who live with it commonly experience a high degree of deterioration in multiple areas of daily functioning, including personal care, daily life activities, education, and employment (Cook et al., 2009; Foruzandeh & Parvin, 2013). Occupational therapy practitioners play a key role on mental health teams by promoting clients’ optimal occupational performance in their daily life activities regardless of mental, physical, and environmental barriers. Practitioners facilitate participation in activities and occupations that are important to the individual client, promoting satisfactory participation in the community (Pettersson et al., 2012).
The International Classification of Functioning, Disability and Health (ICF; WHO, 2001) provides a common and universal language to describe functioning, disability, and health in people with all types of health conditions for use by professionals in rehabilitation disciplines (Farrell et al., 2007). The ICF is based on a biopsychosocial model that provides a holistic, multidimensional, and interdisciplinary vision for understanding health and health-related conditions (Pettersson et al., 2012) and the dynamic interactions among the underlying health condition, functioning and disability, and personal and contextual factors. In consideration of this holistic approach, the World Federation of Occupational Therapists was one of the first associations to recognize the potential usefulness of the ICF in clinical practice, rehabilitation, intensive care, and research (Hemmingsson & Jonsson, 2005).
In clinical practice, it is not viable to use the whole ICF, which contains more than 1,400 categories. To facilitate its application, ICF Core Sets (ICF–CSs) have been developed for different health conditions, including schizophrenia (Gómez-Benito et al., 2018). The Comprehensive ICF–CS for schizophrenia includes 97 categories that cover the spectrum of typical problems in functioning experienced by people living with schizophrenia. The Brief ICF–CS is a subset of 25 of these 97 categories considered essential for the evaluation and treatment of this population. Further information about the ICF is available in Supplemental Figures 1 and 2 (available online at https://otjournal.net; navigate to this article, and click on “Supplemental”).
The next step toward the application of the ICF–CSs for schizophrenia in clinical practice is to validate them from the perspectives of all health professionals who play a key role in treating people living with schizophrenia. To date, this validation has been carried out from the perspectives of psychiatrists, psychologists, and mental health nurses, obtaining results that support the validity of the ICF–CSs for schizophrenia (Nuño, Barrios, et al., 2019; Nuño et al., 2018; Nuño, Guilera, et al., 2019). The objectives of this study were twofold: (1) to identify the problems, resources, and aspects of the environment addressed by occupational therapists in intervention with people living with schizophrenia and (2) to analyze, through a Delphi study, the content validity of the ICF–CSs for schizophrenia from the perspective of occupational therapists.
Method
Design
The study was conducted as a worldwide email survey using a three-round Delphi method. The Delphi method is a multistage process that aims to obtain consensus from a panel of individuals with knowledge of the topic being investigated (“experts”; Trevelyan & Robinson, 2015), in this case occupational therapists. Methodological rigor was ensured by applying the Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist (Booth et al., 2014).
Participant Recruitment
We identified and contacted international associations of occupational therapists, universities, care units, hospitals, and other institutions and asked them to publicize the study. Participation was allowed for speakers of five of the more frequently spoken languages in which the ICF is available (English, Spanish, French, Chinese, and Russian) to avoid language barriers and increase the representativeness and participation of experts from around the world. All materials were translated and supervised by at least two independent native speakers. Occupational therapists who agreed to participate received an email with study and participation details, and they were asked to confirm their expertise in schizophrenia treatment and to provide written consent to be included in the study. Demographic and professional data were also requested.
Professionals with specific training as occupational therapists and at least 1 yr experience in the treatment of people with schizophrenia were eligible to participate. No knowledge about the ICF was required. Occupational therapists who had participated in an earlier stage of the development of the ICF–CSs for schizophrenia were excluded. A total of 127 experts were eligible to participate and invited to start the first round of this study. The Institutional Review Board Committee of the University of Barcelona (IBR00003099) approved the study.
Delphi Process
A web-based survey was conducted using Qualtrics (Provo, UT) from April 2017 to January 2018. All potential participants received an email with instructions and a link to the survey. Three reminders were sent: 1 week before the deadline, 2 days before the deadline, and on the deadline day itself.
In the first Delphi round, the experts received a questionnaire with six open-ended questions that covered all the ICF components (i.e., Body Functions, Body Structures, Activities and Participation, Environmental Factors, and Personal Factors). They were asked to list all the aspects they considered to be relevant when assessing or treating people with schizophrenia (see Figure 1). Answers were linked to the ICF categories (see the “Linking” section), and the categories reported by at least 5% of participants were included in the survey for the second Delphi round.
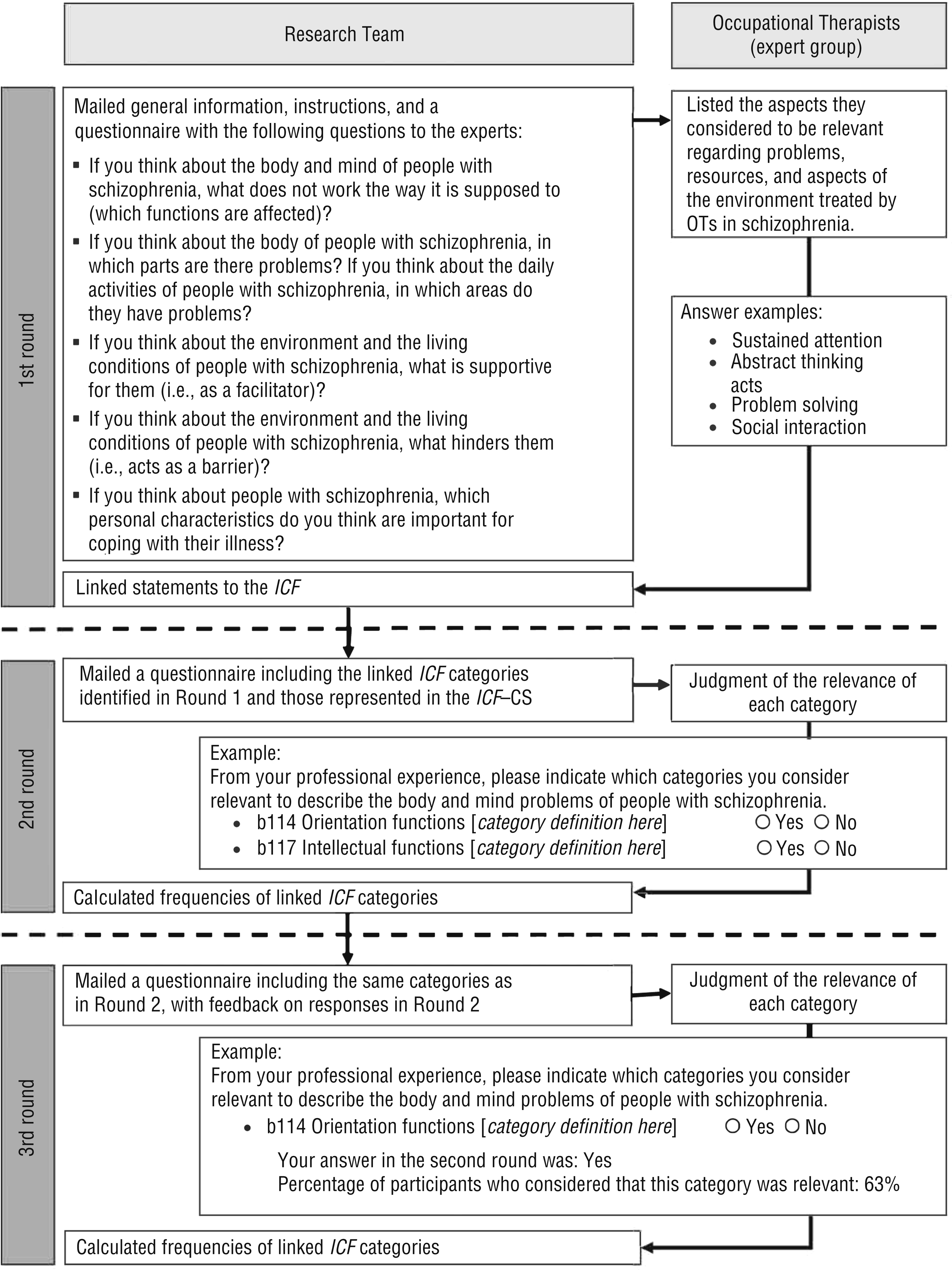
Delphi process for the study of occupational therapists’ perspective on the ICF Core Sets for schizophrenia.
In the second round, all participants received a survey with a list of the codes and definitions of (1) the 97 ICF categories from the Comprehensive ICF–CS for schizophrenia and (2) ICF categories that were not included in the Comprehensive ICF–CS but that corresponded to relevant aspects reported by at least 5% of participants. Participants did not know which categories belonged to the Comprehensive ICF–CS for schizophrenia and which did not. They had to decide whether the listed ICF categories did or did not (yes–no response) represent problems, resources, or environmental factors treated by occupational therapists in work with people with schizophrenia, and they were asked to take into account that the final list should be as short as possible to be practical but as comprehensive as needed to capture the most relevant needs of people with schizophrenia.
In the third round, participants received the same list of ICF categories with codes and definitions, this time with feedback on the responses of the expert panel as a whole and their own previous responses. They were asked again to judge the relevance of each ICF category (yes–no response).
Linking
Each component of the ICF except Personal Factors contains an exhaustive, hierarchical list of categories. In line with established linking rules (Cieza et al., 2019), each response from the first Delphi round was linked to the most precise ICF category by two health professionals trained in the use of the ICF. Because of the large number of responses to be linked, we created three coding teams, each with two health professionals trained in the use of the ICF and experienced in providing care to people with schizophrenia. Any disagreement between the two independent coders was reviewed and discussed by members of the research team (Georgina Guilera, Morris Bell, Laura Nuño) to reach consensus. The definitions of the ICF categories, along with inclusion and exclusion examples, can be found in the ICF manual (WHO, 2001). Because Personal Factors are not yet classified in the ICF, they were categorized by consensus among three psychologists (Guilera, Bell, Nuño) on the basis of theories of personal factors such as the Big Five personality traits (McCrae & Costa, 2008), previously proposed categorizations (Grotkamp et al., 2012; Nuño et al., 2018), and the experts’ responses.
Data Analysis
Descriptive statistics were used to characterize the sample and the frequencies of ICF categories selected in the second and third rounds. On the basis of previous studies (Kaech Moll et al., 2016; Nuño, Barrios, et al., 2019), we considered consensus to be agreement of at least 75% among the occupational therapists in the third round of the Delphi survey. A κ coefficient with bootstrapped confidence intervals (CIs) was calculated to analyze intercoder reliability. Statistical analyses were performed using IBM SPSS Statistics (Version 23.0; IBM Corp., Armonk, NY).
Results
A total of 92 occupational therapists from 29 countries representing all six WHO regions completed the first-round questionnaire (72.4% of the 127 who were invited to participate). Seventy-three (79.3%) completed the third round. On average, they had 9.9 yr experience treating people with schizophrenia (range = 1–44 yr). Their professional roles primarily involved clinical practice (mean of 52.5% of their time), followed by teaching and training (18.8%), research (14.7%), management (12.4%), and other tasks (1.6%). Table 1 shows participants’ demographic and professional characteristics.
Demographic and Professional Data Summary of Survey Respondents (N = 92) Across the Three Delphi Rounds
Note. WHO = World Health Organization.
It was possible to select more than one option.
South Africa and Zimbabwe.
Brazil, Canada, Chile, and United States.
Saudi Arabia and United Arab Emirates.
Belgium, Denmark, Finland, France, Germany, Greece, Iceland, Ireland, Israel, Netherlands, Portugal, Spain, Sweden, and United Kingdom.
India.
Australia, China, Japan, Singapore, and Taiwan.
In the first Delphi round, the experts named 2,527 meaningful concepts, which were linked to 209 ICF categories. Of these, 88 categories were excluded because they were reported by fewer than 5% of participants. Regarding Personal Factors, the experts named 38, of which 7 were excluded because they were reported by fewer than 5%. Thus, 121 ICF categories and 31 Personal Factors were presented to the experts in the second round. The κ coefficient and its bootstrapped CI for the linking process were 0.73 [0.71, 0.75].
Of the 121 ICF categories presented in the second Delphi round, agreement of at least 75% was reached for 97 (80%). Consensus was reached for all categories included in the Brief ICF–CS for schizophrenia with agreements of 95% or more. The comparative analysis that follows therefore focuses on the Comprehensive ICF–CS. As shown in Table 2, of the 97 ICF categories for which consensus was reached, 89 are included in the Comprehensive ICF–CS. At the same time, of those categories represented in the Comprehensive ICF–CS, participants reached consensus on 89 (92%). Table 3 gives details on the 16 categories that did not overlap both sets of categories. Further information about the study results can be found in Supplemental Tables 1–5 (available online at https://ajot.aota.org; navigate to this article, and click on “Supplemental”). In addition,
Regarding the Body Functions component of the ICF, the experts reached consensus on 14 of the 23 categories (61%). Of these, 13 were also included in the Comprehensive ICF–CS (e.g., b140 Attention functions). The only category for which consensus was reached but that was not represented in the ICF–CS was b126 Temperament and personality functions. Consensus was not reached for 4 categories of the ICF–CS.
Concerning the Body Structures component, 8 ICF categories were presented to the experts, and they reached consensus on only 1 (s110 Structure of brain). The ICF–CS does not contain any category from this component.
From the Activities and Participation component, consensus was reached on 46 of the 51 categories (90%) presented to the experts; only 1 category (d810 Informal education) is not included in the ICF–CS. Consensus was not reached for 3 categories of the ICF–CS (d166 Reading, d330 Speaking, and d335 Producing nonverbal messages).
Of the 39 ICF categories analyzed from the Environmental Factors component, consensus was reached for 36 (92%). Of these, only 5 categories were not included in the ICF–CS (e.g., e135 Products and technology for employment). Of the included categories, consensus was not reached for only 1 (e125 Products and technology for communication).
In all, 31 Personal Factors were presented to the experts. Consensus was reached on 27 (90%) of them, 8 with agreement of 99% or more.
Summary of ICF Categories That Yielded Consensus and Comparison With the Categories Represented in the Comprehensive ICF–CS for Schizophrenia
Note. ICF = International Classification of Functioning, Disability and Health; ICF–CS = ICF Core Sets for schizophrenia.
Categories That Did Not Match When Comparing the Comprehensive ICF–CS for Schizophrenia With the Categories That Yielded Consensus
Note. ICF = International Classification of Functioning, Disability and Health; ICF–CS = ICF Core Sets for schizophrenia.
Categories for which consensus was reached but that do not appear in the Comprehensive ICF–CS.
Categories in the Comprehensive ICF–CS for which consensus was not reached.
Discussion
The results of this study show that the content validity of the ICF–CSs for schizophrenia has support from the perspective of occupational therapists worldwide. These results are in agreement with those of previous studies from the perspectives of psychiatrists (Nuño et al., 2018), psychologists (Nuño, Guilera, et al., 2019), and nurses (Nuño, Barrios, et al., 2019), further supporting the international validity of the ICF–CSs for schizophrenia. For all categories included in the Brief ICF–CS, consensus was reached with a high level of agreement. Of the 97 categories represented in the Comprehensive ICF–CS, consensus was achieved for 92%.
Regarding the Body Functions component of the ICF, most categories belong to the b1 Mental functions chapter and only one to the b6 Genitourinary and reproductive functions chapter (i.e., b640 Sexual functions). All the categories that achieved a high level of agreement within the b1 Mental functions chapter correspond to typical symptomatic manifestations of schizophrenia. Indeed, schizophrenia is associated with the presence of alterations in perception (e.g., b156 Perceptual functions), negative symptoms such as decreased expression and motivational deficits (e.g., b130 Energy and drive functions), alterations in thinking (e.g., b160 Thought functions), and cognitive deficits (e.g., b164 Higher-level cognitive functions; Bailliard & Whigham, 2017). This finding accounts for the relevance of this component and the categories in the b1 Mental functions chapter to defining functioning in people with schizophrenia from the perspective of occupational therapists. These results coincide with the findings obtained from other professional perspectives (Nuño, Barrios, et al., 2019; Nuño et al., 2018; Nuño, Guilera, et al., 2019). They also show that occupational therapists play a key role because they can guide clients, caregivers, and the treatment team with respect to multiple factors that influence the recovery or development of functional capacities (Tanaka et al., 2014). In fact, cognitive functioning has been related to occupational engagement and thus to the ability to perform daily occupations in a balanced rhythm (Lexén & Bejerholm, 2018).
As in the previous studies, one category of the b1 Mental functions chapter for which consensus was achieved (in fact, with 95% agreement) is not included in the ICF–CSs for schizophrenia: the category b126 Temperament and personality functions. Our expert participants agreed on the relevance of addressing aspects of personality in people with schizophrenia, which can expand the understanding of these clients and their symptoms. Therefore, the inclusion of this category in the ICF–CSs for schizophrenia should be considered. Likewise, although more than 60% of participants considered four categories that are part of the ICF–CSs (i.e., b117 Intellectual functions, b330 Fluency and rhythm of speech functions, b530 Weight maintenance functions, and b765 Involuntary movement functions) to be relevant, they did not reach consensus. The level of agreement may be low because this set of functions is not usually treated by occupational therapists, who focus mainly on helping people recover and participate in significant life roles.
In relation to the Body Structures component, the ICF–CSs for schizophrenia do not include any related categories. However, the category s110 Structure of brain obtained a broad consensus among the participants. This finding coincides with the results of our previous studies from other professional perspectives. Indeed, schizophrenia is associated with changes in the structure and functioning of several brain systems that are considered to underlie the cognitive disorders described in people with schizophrenia (Chang et al., 2018). Intervention by occupational therapists has been related to improvements in neurocognitive functioning (Shimada et al., 2016) and may therefore influence these brain structures. Further study of anomalies in these systems is needed to improve the understanding of their causes, their progression, and the effects of treatment to address them. Thus, from the perspective of occupational therapists, the inclusion of this category in the ICF–CSs for schizophrenia should be considered.
The Activities and Participation component had the largest number of categories for which consensus was reached. This result is not surprising because promoting participation in daily activities (e.g., productive activities, daily life skills, self-care tasks) is a priority work area for occupational therapy practitioners (Foruzandeh & Parvin, 2013). Improvements in clients’ functioning, participation in meaningful activities, self-determination, confidence, and satisfaction with community life are treatment objectives in occupational therapy (Morris et al., 2018; Tapfumaneyi et al., 2015). In accordance with our previous studies, the categories associated with work participation obtained a high level of consensus, showing that from the perspective of occupational therapists, addressing employment and involvement in meaningful activities for people living with schizophrenia is a necessary aspect of intervention (Eklund et al., 2012).
Three categories from the ICF–CSs were not confirmed in the current study: d166 Reading, d330 Speaking, and d335 Producing nonverbal messages. These categories are usually treated by other health professionals such as psychologists or neuropsychologists, which may be why they were not selected. It is also worth noting that a high level of agreement was reached for d810 Informal education, a category that is not included in the ICF–CSs, which may reflect the importance given by occupational therapy practitioners to continuous training and learning through informal education (Andersen, 2001).
The current study also shows the importance of the Environmental Factors component of the ICF for occupational therapists; consensus was reached on 31 of the 32 categories present in the ICF–CSs for schizophrenia. Consensus was also reached on other categories not represented in the ICF–CSs, such as various categories from the e1 Products and technology chapter and the e5 Services, systems and policies chapter, although the ICF–CSs already include four categories of the e1 chapter and 10 of the e5 chapter. Given that the ICF–CSs should be as short as possible, participants may have considered that the areas not included were sufficiently covered by the categories already there. The emphasis on categories in these two chapters is consistent with the importance occupational therapy practitioners place in their clinical practice on the social resources, products, and technologies people can use to facilitate activities required for daily life (e115 Products and technology for personal use in daily living), leisure and recreation activities (e140 Products and technology for culture, recreation and sport), and participation in the labor market (e135 Products and technology for employment). In addition, the categories e310 Immediate family and e355 Health professionals had high levels of agreement, showing the relevance of these agents as possible facilitators or obstacles in the recovery process of people with schizophrenia (Marwaha et al., 2009).
The Personal Factors component of the ICF has not yet been developed. In our study, the occupational therapists achieved consensus on 27 Personal Factors, 24 of them with agreement of 90% or higher. Many of the Personal Factors with a high level of agreement coincide with those identified from the perspective of psychiatrists, nurses, and psychologists. For example, 100% agreement was reached on the categories of Resilience, Personal history and biography, and Lifestyle, reflecting the important role these factors play in the recovery and well-being of people with schizophrenia (Mizuno et al., 2016), as well as in the presentation and evolution of the disease (Rajkumar, 2015). These results indicate that a classification of Personal Factors in the ICF is necessary so that professionals such as occupational therapists can describe in a detailed and exhaustive manner the relevant personal aspects that influence the health and daily functioning of people with schizophrenia to aid clients in strengthening their participation in meaningful and satisfactory occupations (Doroud et al., 2015).
Strengths and Limitations
This study has several methodological strengths. First, the Delphi method is a widely recognized and appropriate method for the purpose of this study, and its usefulness was maximized by including a large number of participants from around the world. The response rate in the study was high, and broad worldwide representation was achieved. In addition, the sample consisted of highly qualified occupational therapists with extensive experience in the treatment of people with schizophrenia in both acute and chronic stages and rural and urban settings.
However, some limitations should be considered. Despite the worldwide participation, some WHO regions, particularly Southeast Asia and the Eastern Mediterranean, are underrepresented. This imbalance may be attributable to a lower presence of the occupational therapy profession or less frequent intervention with people with schizophrenia in these regions, as well as to greater difficulties in accessing these professionals (e.g., as a result of limitations on the use of the Internet).
Implications for Occupational Therapy Practice
The findings of this study have the following implications for occupational therapy practice:
The ICF–CSs for schizophrenia can be highly useful tools for occupational therapy practitioners in clinical practice. Especially in multidisciplinary clinical settings, use of these tools may serve to enhance communication within multiprofessional teams and guide the management and treatment of people with schizophrenia by different health professionals.
The ICF–CSs for schizophrenia can provide a comprehensive framework for organizing information according to the biopsychosocial perspective of the ICF, considering both health conditions and their relationship to clients’ daily lives and environments.
Conclusion
The results of this study support the use of the ICF–CSs for schizophrenia by occupational therapy practitioners in clinical practice with people with schizophrenia. The ICF–CSs for schizophrenia appear to be clear and useful guides to describing and classifying clients’ functioning, health, and rehabilitation using a language and frame of reference shared by other health professionals (Hemmingsson & Jonsson, 2005). Occupational therapy practitioners are essential in the rehabilitation of people with schizophrenia, and their perspective has contributed to the development and enrichment of the ICF–CSs for schizophrenia.
Supplemental Material
Supplementary material for Occupational Therapists’ Perspective on the International Classification of Functioning, Disability and Health Core Sets (ICF–CS) for Schizophrenia
Supplementary material, sj-docx-1-aot-10.5014_ajot.2021.041509.docx for Occupational Therapists’ Perspective on the International Classification of Functioning, Disability and Health Core Sets (ICF–CS) for Schizophrenia by Laura Nuño, Georgina Guilera, Morris Bell, Emilio Rojo, Juana Gómez-Benito, Caterina Calderón and Maite Barrios in The American Journal of Occupational Therapy
Footnotes
Acknowledgments
We thank the participating experts for their time and commitment, without which the study would not have been possible. Further information about the experts who participated in this study is available in Supplemental Table 6.
This work was supported by Spain’s Ministry of Economy and Competitiveness (Grant PSI2015–67984-R) and by the Agency for the Management of University and Research Grants of the Government of Catalonia (Grant 2017SGR1681). The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript. The authors have no conflict of interest to declare.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.