
Abstract
This study supports the need for occupational therapy entry-level programs to reexamine the categories and amount of AT training their curricula currently provide.
From the workplace to the home, technology is embedded in every aspect of people’s daily lives. This technology explosion has allowed people with disabilities access to many new opportunities through assistive technology (AT). An AT device is defined in the Technology-Related Assistance for Individuals With Disabilities Act of 1988 (Pub. L. 100-407) as “an item, piece of equipment, or product system, whether acquired commercially off the shelf, modified, or customized, that is used to increase, maintain, or improve functional capabilities of individuals with disabilities” (p. 3). Occupational therapists are in an ideal position to recommend and implement the appropriate use of AT. Occupational therapists’ education and experience provide them with the knowledge and basic skills to evaluate clients and provide AT devices and services to support their occupational success (American Occupational Therapy Association [AOTA], 2015).
The history of educating occupational therapists in the provision of AT began in 1990, when the National Board for Certification in Occupational Therapy established focus groups to determine the need to include AT on the certification exam (Angelo et al., 1997). This was followed in 1991 by AOTA requiring that occupational therapy programs include AT in their curricula to be accredited (Angelo et al., 1997). The AOTA Technology Special Interest Section developed AT competencies for occupational therapists, including a textbook that focused on the categories of seating and mobility, prosthetics and orthotics, rehabilitation technology, and computer access and determined that “all occupational therapists should know about technology applications within a functional perspective at a minimal level” (Hammel & Smith, 1993, p. 971). These AT competencies were foundational; they directed that practitioners know about basic AT devices, how to use them, and how to determine each client’s need for them (Hammel & Smith, 1993). The Accreditation Council for Occupational Therapy Education (ACOTE®) 2011 and 2018 requirements include two standards referring to the provision of AT, including designing, fabricating, applying, fitting, and training; currently, the standards specify only two AT categories: electronic aids related to daily living (EADLs) and seating and positioning systems (ACOTE, 2018).
AT is broadly defined as including many different categories: augmentative and alternative communication (AAC), cognitive aids, computer access, EADLs, sensory (vision or hearing), seating and mobility, recreation, environmental modification, accessible transportation, and technology for learning disabilities (Rehabilitation Engineering and Assistive Technology Society of North America [RESNA], 2017). AT is used in occupational therapy practice across different settings for a variety of diagnoses and populations, and it is often provided as part of an interdisciplinary team, including speech-language pathologists, physical therapists, and, in the school setting, special education teachers.
Despite AT content being required in higher education curricula for more than 20 yr, many therapy professionals do not feel comfortable and confident in using AT as part of their intervention strategies. Gitlow and Sanford (2003) identified the amount of AT education allied health practitioners (N = 62; 21 occupational therapists) received in their programs. More than two-thirds of participants reported having rudimentary or no knowledge in most AT areas, and more than half reported a moderate to significant need for education in all areas of AT apart from activities of daily living. Perceived competence of participants was low, with 67% reporting that they had some knowledge with critical gaps, and 15% rating themselves as lacking basic competence.
If occupational therapists are not comfortable with or confident in using AT in intervention, then how much education on AT are they receiving in their collegiate experience? Brady et al. (2007) surveyed 32 program directors of occupational therapy, physical therapy, speech-language therapy, and special education programs to determine the extent to which education on AT was provided in college. Of occupational therapy program directors, 25% indicated students receive 1 to 20 hr of AT education, 23% receive 21 to 40 hr, and 25% receive 41 to 60 hr. They found that 40% of occupational therapy programs surveyed provide education on AT in a course solely dedicated to AT, and 28% embed AT education in other courses. In another study of exclusively occupational therapists, Long et al. (2007) surveyed 272 pediatric occupational therapists and their perceptions of the need for training in AT and delivery of AT services. They discovered that 39% of participants reported they had inadequate training in AT, and 5% had received no training. Although the literature reviewed indicated that AT education is being provided in entry-level occupational therapy curricula, many therapists reported that they did not feel competent in providing AT devices and services in practice (Long et al., 2007).
Missing from the recent literature is information about the specific categories of AT education provided in higher education curricula. An expected outcome of this research was to gather evidence to support the need to embed more categories of AT into occupational therapy curricula. The purpose of this study was to describe the perceived educational needs of occupational therapists using AT in practice. This study’s outcomes will contribute to a determination of what categories of AT are missing from occupational therapy educational curricula and what further education therapists may need to develop competency.
Method
Participants
Participants (N = 148) were occupational therapists certified as ATPs recruited through the RESNA email list (21% response rate). Occupational therapists pursue ATP certification to validate knowledge and professional experience in a variety of AT categories (RESNA, 2017). ATP-certified occupational therapists were selected because of their knowledge of categories of AT, including AAC, cognitive aids, computer access, EADLs, sensory (vision and hearing), seating and mobility, recreation, environmental modification, accessible transportation, and technology for learning disabilities. Therapists were excluded from the study if they were not both an occupational therapist and ATP certified by RESNA.
Instrument
We created a Qualtrics survey tool (Qualtrics, Provo, UT) to capture the specific experiences of occupational therapists in AT education, focusing on quality, intensity, and categories. Survey questions focused on demographics, practice setting, years of experience, training in categories of AT during the occupational therapy program, and categories of need for AT training. Responses were measured with Likert-scale, multiple-choice, or ordinal ranking-scale questions. Open-response questions were included to capture information unique to participants. The final 44-question survey included 33 Likert-scale (rated as 1 = none, 2 = a little, 3 = some, and 4 = a lot), 5 multiple-choice, 3 ordinal ranking, and 3 open-response questions.
Data Collection and Analysis
After institutional review board approval, we collected contact information for 700 ATP-certified occupational therapists from the RESNA database. The purpose and content of the survey were addressed in a cover letter sent via email with the survey link and information, including the purpose and a description of the study. Deadlines and instructions for completion of the survey were also included.
Data were analyzed using Qualtrics, Microsoft Excel (2016; Microsoft Corp., Redmond, WA), and IBM SPSS Statistics (Version 24; IBM Corp., Armonk, NY). Descriptive statistics, including frequency distributions, means, and standard deviations, were calculated. Chi-square analyses of Likert-scale questions were performed to determine the association among categorical variables of the participants’ years of experience, practice areas, specialty training, frequency of AT use, and importance ascribed to AT. Independent-samples t tests were performed to discern the relationship between types of AT education received preprofessionally and types of AT used in practice. Pearson correlations were calculated to examine the association between experience as an occupational therapist, ATP, and the importance participants ascribed to using AT in practice. Statistical significance was set a priori at p ≤ .05. Qualtrics and Microsoft Excel were used to develop tables and charts to describe the results of the research study. Open-ended questions were included to provide qualitative data on the participants’ definition of AT and education that would best benefit occupational therapy practitioners.
Results
A total of 148 surveys were completed and analyzed, for a response rate of 21%. Most participants (71%) reported having 15 or more years of experience as an occupational therapist. Years of experience as an ATP varied, with most participants (26%) having 2 to 5 yr of experience. Of the participants, 112 (76%) indicated that they had obtained additional specialty certification or training, with seating and mobility being the most common. The most prevalent practice areas were school-based practice, seating and mobility, and outpatient settings.
We asked participants to indicate in which of 10 categories they received AT education during their entry-level occupational therapy program (bachelor’s, master’s, or doctorate level). Participants reported environmental modifications, seating and mobility, and sensory (hearing and vision) as the top three AT categories of training during their entry-level occupational therapy program and technology for learning disabilities, computer access, and AAC as the AT categories in which they received no training (Figure 1). Participants also reported that seating and mobility, computer access, AAC, and technology for learning disabilities were the AT categories in which they desired more training during their entry-level occupational therapy program (Figure 2).
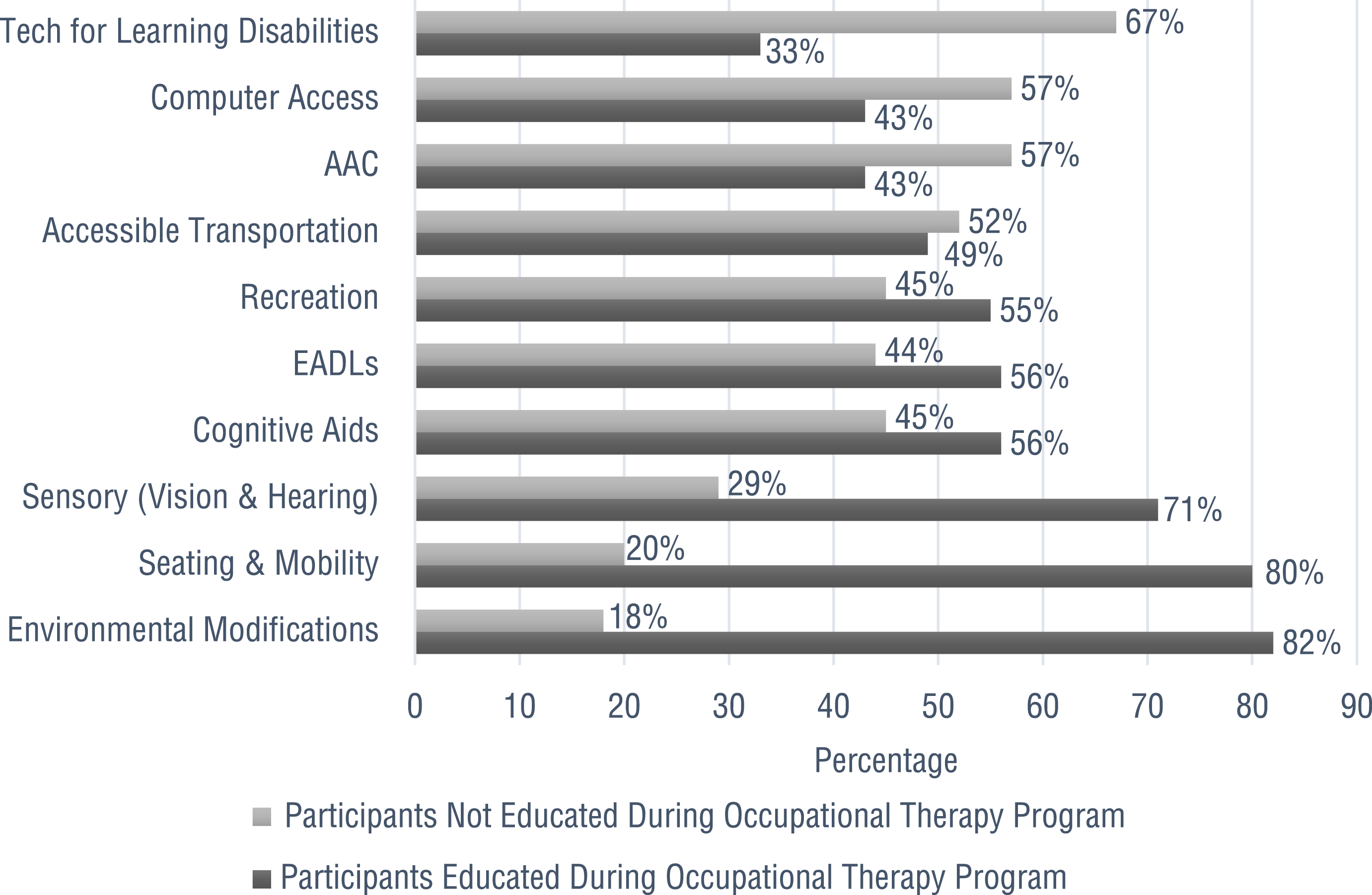
Percentage of OT participants educated compared with those not educated in AT categories during OT curricula.
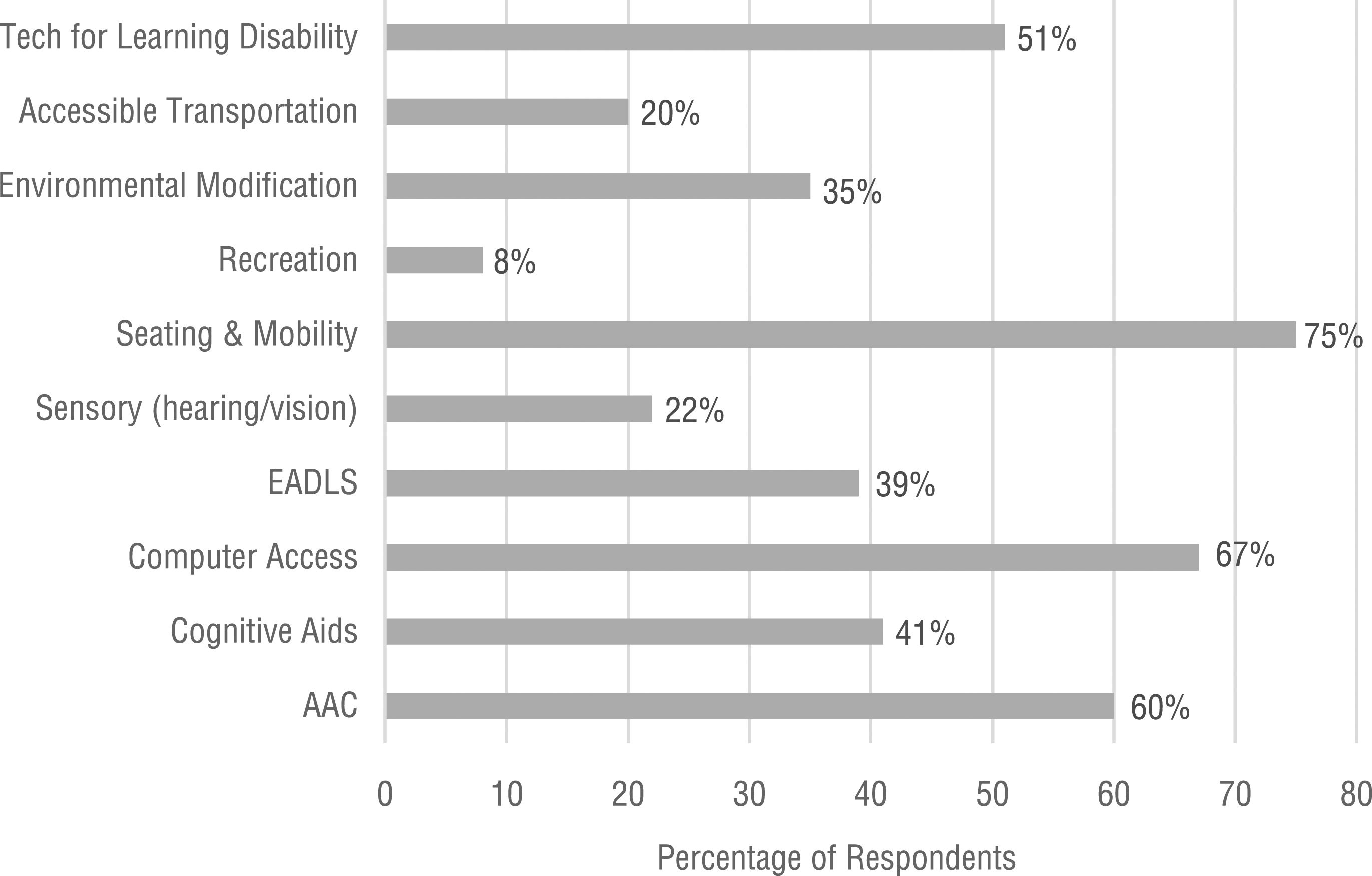
Top AT categories in which participants desired more education during OT curricula.
When participants were asked how often they incorporate AT into occupational therapy intervention, 91% reported they use AT always or often. The categories of AT that participants reported using most often were seating and mobility, environmental modifications, and sensory (hearing and vision). Participants reported least often using AT during intervention for learning disabilities, accessible transportation, and recreation.
Participants’ responses to the question of how they explain AT to practitioners and clients included describing AT as a way of increasing a person’s independence, as tools to assist clients, or by using the Individuals With Disabilities Education Improvement Act of 2004 (Pub. L. 108-446) definition. One participant answered, “AT is tools to help the student accomplish his/her goal and demonstrate the skills and knowledge that they already have.” Another answered, “AT is devices and equipment that improve function to achieve greater independence, safety, productivity, self-determination, communication, social connections, and community inclusion.”
Participants’ open-ended responses on AT categories they would recommend being included in OT curricula were varied, although most agreed more education and training about seating and mobility should be added. One participant answered, “They should at least understand that they should know the role AT plays and actively embrace technologies as new tools for achieving OT goals.”
Analysis
Independent-samples two-tailed t tests (Salkind, 2017) were conducted to determine whether a participant received entry-level training in an AT topic area and used that type of AT in practice. Significant differences were found between those who did and did not receive training in cognitive aids and sensory (vision and hearing) categories and use of them in practice, t(123) = −3.628, p < .001, and t(126) = −3.778, p < .001, respectively, meaning that participants reported using these AT categories more often if they had been exposed to them in their professional education.
We conducted a Pearson correlation analysis (McGraw & Wong, 1996), which revealed significant correlations between the length of time as an occupational therapist and frequency of AT use, r(147) = .251, p < .05; time as an ATP, r(147) = .395, p < .001; and time as an ATP, r(147) = .395, p < .001. We found significant correlations between frequency of AT use and perceptions of the importance of AT, r(147) = .456, p < .001, and length of time as an ATP, r(147) = .238, p < .05. We did not find a significant correlation between length of time as an ATP and perception of the importance of AT, r(147) = .124, p > .05 (Table 1).
Pearson Correlations Between Experience as an ATP and Value, Importance, Frequency of AT Use
Note. ATP = assistive technology professional; AT = assistive technology; OT = occupational therapist.
p < .05. **p < .001.
We conducted a Pearson χ2 analysis (Agresti, 2013) of the area of education most desired by participants during their entry-level occupational therapy education and current areas of employment. This test compares categorical or nominal variables and their frequencies. We found significant associations between participants’ work settings and areas of desired entry-level education for computer access, χ2(7) = 17.615, p < .05; EADLs, χ2(7) = 14.423, p < .05; seating and mobility, χ2(7) = 22.220, p < .05; environmental modification, χ2(7) = 20.537, p < .05; and technology for learning disabilities, χ2(7) = 51.151, p < .001 (Table 2).
Pearson χ2 Analysis of Occupational Therapy Work Setting and Desired Categories of AT Education in OT Curricula
Note. AAC = augmentative and alternative communication; AT = assistive technology; EADLs = electronic aids to daily living; OT = occupational therapy.
p < .05. **p < .001.
Discussion
We found that occupational therapists do not perceive that their entry-level curricula, whether bachelor’s, master’s, or doctorate, adequately prepared them in the 10 categories of AT studied. Seating and mobility, environmental modifications, and sensory (hearing and vision) aids are the AT categories on which participants agreed they received the most training. Gitlow and Sanford (2003) reported similar results; participants reported they received adequate training in basic AT categories while identifying that they still had critical gaps in AT knowledge. Brady et al. (2007) found that although AT education on specific AT devices and services for children with disabilities were provided, several critical categories were not offered.
AAC, computer access, and technology for learning disabilities are AT categories in which therapists reported receiving little to no training. These results demonstrate a positive correlation with the AT categories participants reported using most in intervention, including computer access and technology for learning disabilities, indicating a possible need for computer access and technology, specifically for learning disabilities, to be incorporated into AT training in entry-level occupational therapy programs. These results demonstrate the recent advances in and recognition of computer access and technology for learning disabilities and the fact that most participants had been professionals for 11 or more years. Other AT categories, including cognitive aids, accessible transportation, and EADLs, are areas in which only half of therapists received training in occupational therapy programs. This information agrees with the open-ended responses to our survey, in which participants indicated a desire for students to receive training in all categories of AT during their entry-level programs.
When we asked in which AT categories participants desired more training during their occupational therapy program, participants reported the areas of seating and mobility, computer access, AAC, and technology for learning disabilities. Brady et al. (2007) found that pediatric occupational therapy practitioners desired more AT training in the areas of high-tech devices such as computers, AAC devices, and funding for devices. Our findings agree with the literature: More training on high-tech AT is desired to meet the needs of occupational therapists.
We found that more experienced occupational therapists valued AT more and used it more in their practice. An explanation for this finding may be that AT was a novel area of practice emphasized in curricula in the 1990s. As we hypothesized, length of time as an ATP correlated with value of AT and time as an occupational therapist. A professional who makes the extra effort to gain ATP certification would most likely value AT as an area of practice. One correlation that was not significant was that between the importance of AT and the length of time as an ATP. One possible explanation is that being so fully immersed in AT shifts one’s perception of the importance of AT in daily practice.
Participants who were trained in specific AT areas (cognitive aids, sensory, recreation, and EADLs) used these more frequently in their practice, suggesting that professional education is critical to their use in practice. In addition, we found an association between participants who desired more education in specific categories of AT (computer access, EADLs, seating and mobility, environmental modification, and technology for learning disabilities) and primary area of occupational therapy practice. This association may be explained by the frequency of use of these specific technologies in the practice area. For example, participants who worked in school-based practice most desired additional entry-level education in technology for learning disabilities, suggesting that therapists in this practice setting have greater need for this type of AT.
One concern for occupational therapy educators is that curricula are already overloaded with content required by accrediting bodies such as ACOTE. One way to add more AT content is to embed technology into education on related practice areas. By embedding technology into existing coursework, educators can highlight relevant technology without adding additional courses. However, this approach requires cross-training faculty in both their area of expertise and AT, which increases the burden on faculty members. An educational approach using both separate AT courses or sections and embedding AT into current courses may be the most effective delivery method. Another option for OTD students interested in more AT training could be using AT as a capstone topic.
Limitations
One limitation to the study identified early on was incorrect or outdated contact information in the RESNA email database. Although 782 participants were identified through the RESNA database, 82 invitations were returned because of incorrect email addresses. Another limitation was that we surveyed occupational therapists who were ATP certified and knowledgeable about AT, and they could be biased toward the importance of AT in practice and the desire to include more AT in occupational therapy curricula. This could limit generalizability of the results because these therapists’ opinions may not represent those of the entire population of occupational therapy practitioners. A third limitation is that we did not ask participants to identify what type of entry-level degree they obtained—bachelor’s, master’s, or doctorate. Comparing the results of participants with different entry-level degrees could provide data to discover whether AT education has changed since moving from an entry-level bachelor’s to an entry-level master’s degree.
Participants’ interpretation of survey questions was a limitation noted in the latter part of the research. Participants skipped some open-ended survey questions (Question 1, n = 19; Question 2, n = 15), and some participants answered these questions in a way that seemed to indicate that they misunderstood what was being asked. Also, participants skipped some of the other survey questions. Participant practice area is another limitation of the study because a majority practiced in school-based therapy or seating and mobility. One final limitation relates to the number of years participants had been occupational therapists. With the advancement of technology in the past 10 to 15 yr and changes in ACOTE standards for occupational therapy curricula, and given that the majority of participants had 11 or more years of experience as a practitioner, this could be a one-sided representation of occupational therapists.
Future Research
Research with a larger sample size and a more generalized sample of occupational therapists is necessary to compare results and obtain more detailed evidence for which AT categories should be prioritized in entry-level occupational therapy programs. This evidence could be used to improve occupational therapy education and encourage the profession to better understand AT as a vital part of occupational therapy intervention. Providing continuing education opportunities for occupational therapy educators on how to disseminate AT education in the curricula may spur research implementation. Data may also be used to assist ACOTE in the revision of occupational therapy accreditation standards on AT. Future research could also look at where AT education fits into the fieldwork experience.
Implications for Occupational Therapy Education
The findings of this study have the following implications for occupational therapy practice:
Continued and selective AT education in entry-level occupational therapy curricula is needed.
Occupational therapy entry-level programs should reexamine current education provided in the AT categories of seating and mobility, environmental modifications, computer access, AAC, and technology for use by people with learning disabilities.
Further research with a larger and diverse sample of occupational therapists is needed to collect significant data supporting the need for including all categories of AT in entry-level occupational therapy curricula.
Technology is embedded in all human occupations, including work, education, play, leisure, rest, and self-care and therefore should be supported in occupational therapy curricula for comprehensive integration in occupational therapy practice.
Conclusion
This study identified the AT categories in which therapists received little to no education in their occupational therapy curricula and the AT categories used most in intervention. These results provide evidence to support the recommendation for occupational therapy programs to review AT categories currently provided and where best to embed additional categories in the curricula.