
Abstract
Researchers found a correlation between caregivers’ limiting the distance traveled during vehicular transportation and behavioral safety issues, leading to concerns that caregivers may not be fully accessing the community and engaging in leisure pursuits.
Autism spectrum disorder (ASD) is a lifelong condition affecting 1 in 59 children that arises from overall underconnectivity in the brain with overconnectivity in specific regions. It usually is identified early in development, at around ages 26 to 36 months (Centers for Disease Control & Prevention [CDC], 2018; Fodstad et al., 2012; Lord et al., 2018) and results in the reorganization of the brain of the person with ASD, leading to “persistent deficits in social communication and social interaction across multiple contexts” and “restricted, repetitive patterns of behavior, interests, or activities” (American Psychiatric Association [APA], 2013, p. 50).
People with ASD commonly demonstrate maladaptive behaviors, such as atypical eating and sleeping, self-injurious behavior, aggression and tantrums, and wandering, that can lead to parental concern regarding transporting their children with ASD (Konst et al., 2013; Solomon & Lawlor, 2018). Self-injurious behaviors such as head banging, head hitting, self-biting, punching or slapping the body, pinching or scratching the skin, and eye poking, as well as aggressive behaviors, occur among 1 in 4 children with ASD and often result in serious medical consequences while further impairing the child’s functioning (Fodstad et al., 2012; Hagopian & Leoni, 2017; Hill et al., 2014). Of the types of aggressive behaviors demonstrated by children with ASD, hot aggression, which is characterized as occurring in the form of tantrums, is the most prevalent (Carroll et al., 2014). Unlike hot aggression, cold aggression lacks explosive behavior and may occur as a result of the child’s desire for an object or to escape (Carroll et al., 2014). An identified cold aggression is elopement or wandering, characterized by the child’s tendency to leave the supervision or safe space of the caregiver, thus exposing the child to potential danger (Anderson et al., 2012). Other behaviors may include poor sensory modulation, including hyperresponsive, hyporesponsive, and sensory-seeking behaviors (Boyd et al., 2010; Carroll et al., 2014; Fodstad et al., 2012; Hagopian & Leoni, 2017).
When children with ASD exhibit these behaviors during vehicular transportation, it can create a challenging and unsafe situation that may have a negative effect on parental and family participation in the community. These behaviors may also result in social isolation for the child and family (Reynolds et al., 2011). In addition, children with ASD and their caregivers may face environmental barriers that limit the frequency, variety, and intensity of community engagement. Families may refrain from engaging with family and friends because of safety concerns with the child’s behavior toward other children, such as biting, hitting, or elopement. Difficulties in vehicular travel because of elopement may dissuade caregivers from long-distance travel for vacations and holidays, affecting other children who may be in the household. Reduced participation may negatively affect the child’s and family’s quality of life (Bedell et al., 2013). Limited empirical evidence has measured diminished participation and quality of life specific to personal transportation and the appropriateness of car safety restraints, but anecdotally caregivers have reported their concerns regarding elopement and the appropriateness of car safety restraints to therapists during treatment sessions and in goal setting. Elopement from a vehicle (a safe space) is potentially lethal. Preventing elopement requires consideration of car safety sytems that go beyond the simple lap and shoulder belt because children can easily unlock these and remove themselves from a vehicle.
Child passenger safety (CPS) involves the consistent use of correctly installed safety and booster seats, seat belts, car door child locks, and other safety devices that are appropriate for a child’s age, weight, and size (Children’s Safety Network, 2018; Townsend, 2012). Sizes, models, styles, and device accessories may vary; however, all child safety devices must meet safety standards that are appropriate for each child and must be appropriately installed in the vehicle (National Highway Traffic Safety Administration, 2014; Sapp & Thelin, 2013). Motor vehicle accidents (MVAs) are the leading cause of unintentional deaths for children ages 1 and older. However, according to the CDC (2014, as cited in Weatherwax et al., 2016), child safety seats decrease the risk of fatalities for infants and toddlers by 45% to 75%, depending on the child’s age. Up to 80% of car seats are improperly installed, and children ages 4 to 8 rank lowest in the use of appropriate child safety restraints (Bruckner & Rocker, 2009, Weatherwax et al., 2016). Moreover, children with special health care needs, such as ASD, are identified as a high-risk population for misuse of car restraints (Falkmer et al., 2004; Korn et al., 2007). Misuse of restraints and being unrestrained in vehicles leads to more serious injuries (and resulting increased health care costs) when accidents occur (Sauber-Schatz et al., 2015).
Children with ASD also have difficulty with sensory modulation and experience distress with small changes and during transitions (APA, 2013). Transportation consistently involves transitions and multiple sensory stimuli; thus, children with ASD often manifest severe behavior problems in response to these challenges (Cihak et al., 2010). The increase in these behaviors during transportation place the child and the driver at greater risk, so appropriate restraint systems are needed to promote the safety of all vehicular occupants. Children’s behaviors, such as crying, refusing to sit, and removing the seat belt, are often given by caregivers as reasons for nonuse. In addition, appropriate restraints may not be available (Nicholas et al., 2016). Without a more informed understanding of how the environment, specifically the ability to use one’s personal vehicle to transport the child with ASD, professionals may be limited in designing interventions to meet the range of needs of parents and children with ASD.
There is a correlation between misuse of safety equipment and parental lack of knowledge of relevant rules and regulations (Falkmer et al., 2004). Parents, including those of children with ASD, often report a lack of knowledge regarding behavioral and sensory strategies, available safe transportation equipment, and seat belt safety laws, and they report concerns about misinformation, cost, and attitudes regarding car safety devices (Weatherwax et al., 2016; Wooster et al., 2016). Currently, the literature exploring how parents of children with ASD perceive their safety and that of their child and other passengers during personal vehicle transportation is limited (Konst et al., 2013; Solomon & Lawlor, 2018). Lack of education and resources, and increased difficulty in participating in the community, have been identified as problem areas and gaps in current research. This study aimed to explore caregivers’ personal accounts of current practice and prior experiences while transporting children diagnosed with ASD and how these experiences affect their participation.
Method
Research Design
To gain insight into caregivers’ experiences, we used a concurrent nested mixed-methods design (Corcoran, 2017). A phenomenological approach was used to collect and analyze data from a population-based survey of caregivers of children with ASD that examined their firsthand experiences (Park Lala & Kinsella, 2011). The use of a survey method allows common themes to be developed and analyzed (Angell & Solomon, 2018; Edwards et al., 2018; Falkmer et al., 2004; Zhou & Yi, 2014). Surveys have been used to gather information on family quality of life, severity of the disorder, social support, coping strategies of families of children with ASD, perceived risk, and current car seat knowledge (Falkmer et al., 2004; Hillman et al., 2017; Pozo et al., 2014). Previous studies have found discrepancies between parent reports and observed use of vehicle restraints with children with special needs resulting from the desire to produce socially desirable responses when interviewed by someone with professional status (Korn et al., 2007). This study sought to eliminate this discrepancy by maintaining anonymity.
Participants
A convenience sample of caregivers was recruited from multiple platforms, including social media sites, email addresses, and personal contacts. Inclusion criteria were as follows: caregivers, ages 18 and older, of a child diagnosed with ASD, who have traveled with or transported the child. Respondents included caregivers of children with either a primary or secondary diagnosis of ASD. Various other co-occurring diagnoses were identified; the most frequently reported were attention deficit hyperactivity disorder, cerebral palsy, and epilepsy. We did not ask the age of the child with ASD. Of the 54 respondents to the question regarding their relationship to the child with ASD, 41 were mothers, 6 were fathers, 2 identified as siblings, and 5 identified as other caregivers. Respondents represented 17 different states or provinces (Table 1).
States or Provinces Represented by Respondents (N = 49)
One participant identified “Mendenhall”; 2 specified “not applicable.”
Measures
An online Qualtrics survey was designed on the basis of common themes identified from the literature, including decreased knowledge regarding CPS, decreased access to easily read and understood CPS literature, need for information on MVAs and proper car seats, increased caregiver anxiety, parental awareness related to child safety, and ASD-specific behaviors (Angell & Solomon, 2018; Boyd et al., 2010; Bruckner & Rocker, 2009; Carroll et al., 2014; Edwards et al., 2018; Falkmer et al., 2004; Fodstad et al., 2012; Hagopian & Leoni, 2017; Townsend, 2012; Wooster et al., 2016; Zhou & Yi, 2014). The survey questions were composed by a formative committee after a comprehensive review of the literature on the topic. The survey was then reviewed by a summative committee of CPS technicians with knowledge of transportation of children with special health care needs. The final survey was then edited for content validity. The question formats included fill in the blank, check all that apply, and multiple choice.
Procedure
The survey was distributed online through social media, including Twitter, Facebook, Reddit, and personal contacts. The study was verified as exempt by the university’s institutional review board, and informed consent was collected from all respondents before survey participation. Data collection was conducted from December 2018 through February 2019. Of those who started the survey, 63 respondents answered the first question, and 41 respondents completed the survey in its entirety. Some did not answer the question regarding residency.
Data Analysis
The data from the survey were compiled and entered into a single Excel file. The surveys were individually coded and then examined through thematic analysis by comparing identical questions in all surveys. Qualitative data were analyzed through index coding and conceptual labeling to categorize open-ended responses into themes (Peacock & Paul-Ward, 2017). These data were analyzed until saturation was reached and common themes were identified. We used a binary method in which we identified the problem and then thematically explored the meaning of the response. Specific themes, including behaviors, participation, and education, were chosen for further analysis. Cross-tabular summaries of the reports of behaviors (aggression, elopement, distracting sensory behaviors, and self-injurious behaviors) and limiting distance travel to and participation in activities outside of the home were generated. Cramer’s V and χ2 statistics were used to assess the strength and direction of the associations of the behaviors with limitations in family functions. An α of .05 (p < .05) was used to determine statistical significance.
Results
The data analysis identified three significant themes that represent caregivers’ experiences and perceptions of traveling with children with ASD: behaviors, participation, and education. We did not ask specific questions regarding the positive effects children with ASD may experience during a drive, which itself can be a calming strategy.
Behaviors
Common behaviors exhibited by the children in this study during vehicular transportation included elopement, distracting sensory modulation behaviors, aggression, and self-injurious behaviors. Of the respondents, 58% reported that children had attempted to elope from the transportation vehicle. Statements from caregivers about elopement included “Child has attempted to open the door to leave the vehicle while moving, or while stopped,” “My child has tried to get out of his seat in a moving vehicle many times. He would unfasten any restraints or wiggle out of them to move freely throughout the vehicle,” and “No injuries, but has jumped out of the car twice because she was having a meltdown.”
Ninety-five percent of respondents said that their child displayed distracting sensory modulation behaviors (Figure 1). Statements about distracting sensory modulation behaviors included “screaming, flapping, throwing, removing seat belt/harnesses, etc.” and “screaming, stimming on shadows and moving objects, head banging.” Sixty-eight percent reported that their child displayed aggressive behaviors during vehicular transportation (Figure 2). Statements from caregivers about aggressive behaviors included “has punched the driver (me) in the head, pulled the driver’s (my) hair, punched the rear windows, and lunged into the front seat to try to pull the keys out of the ignition” and “kicking, hitting, biting, throwing object at us in the front seat or at her sister. Our windshield is cracked because she kicked it during a meltdown. Often makes messes in the car when angry.”
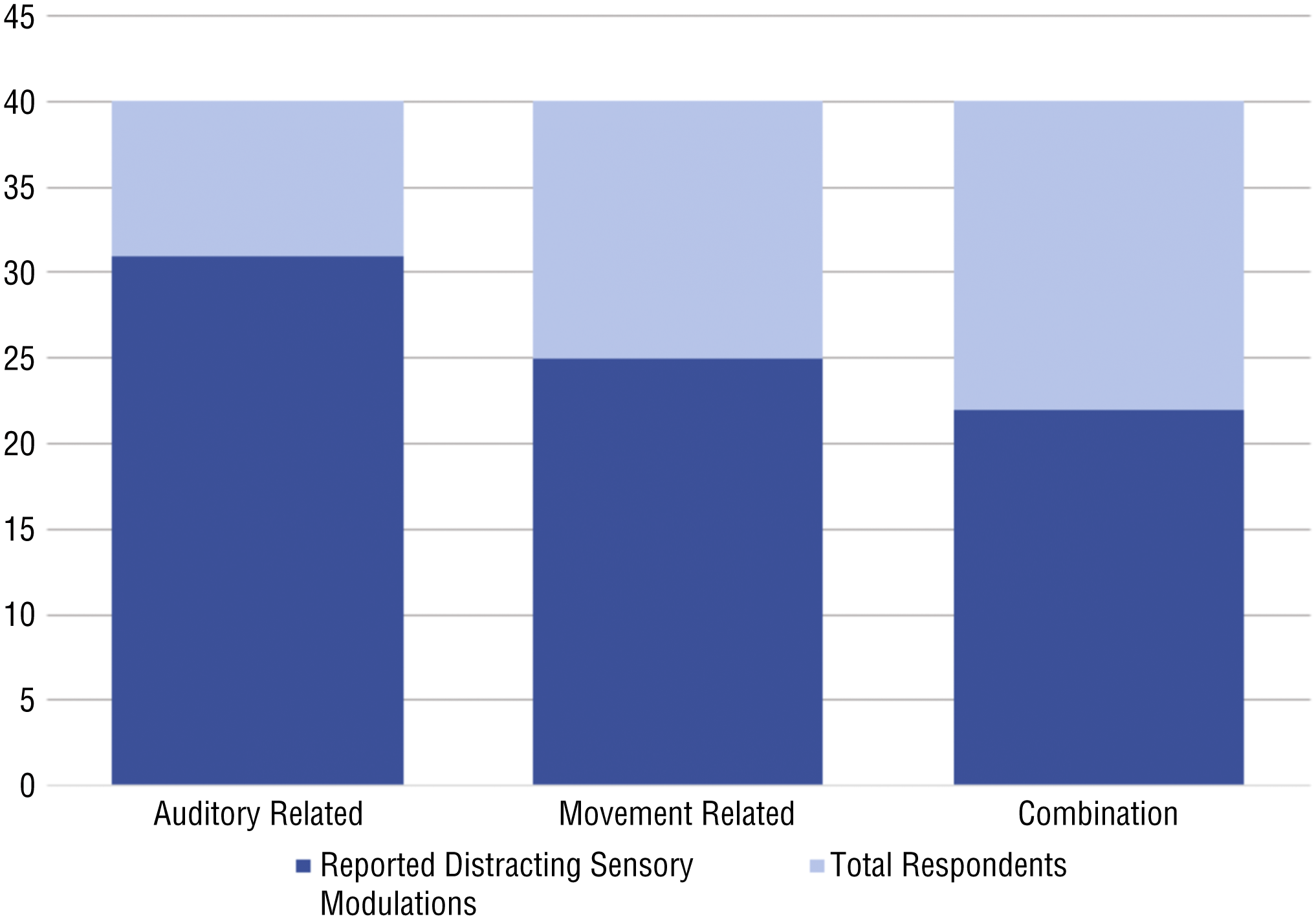
Identified distracting sensory modulation behaviors.
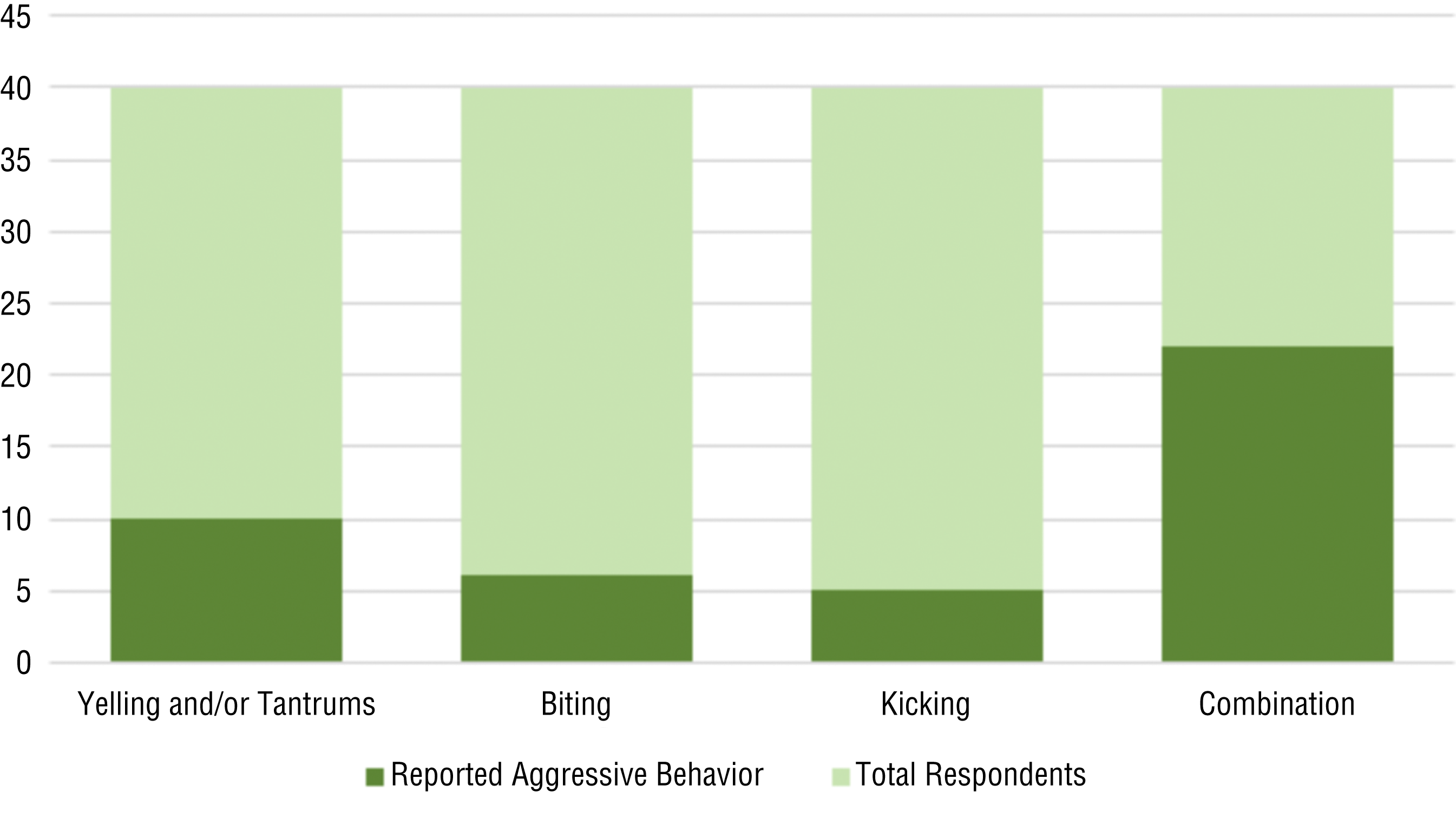
Identified aggressive behaviors.
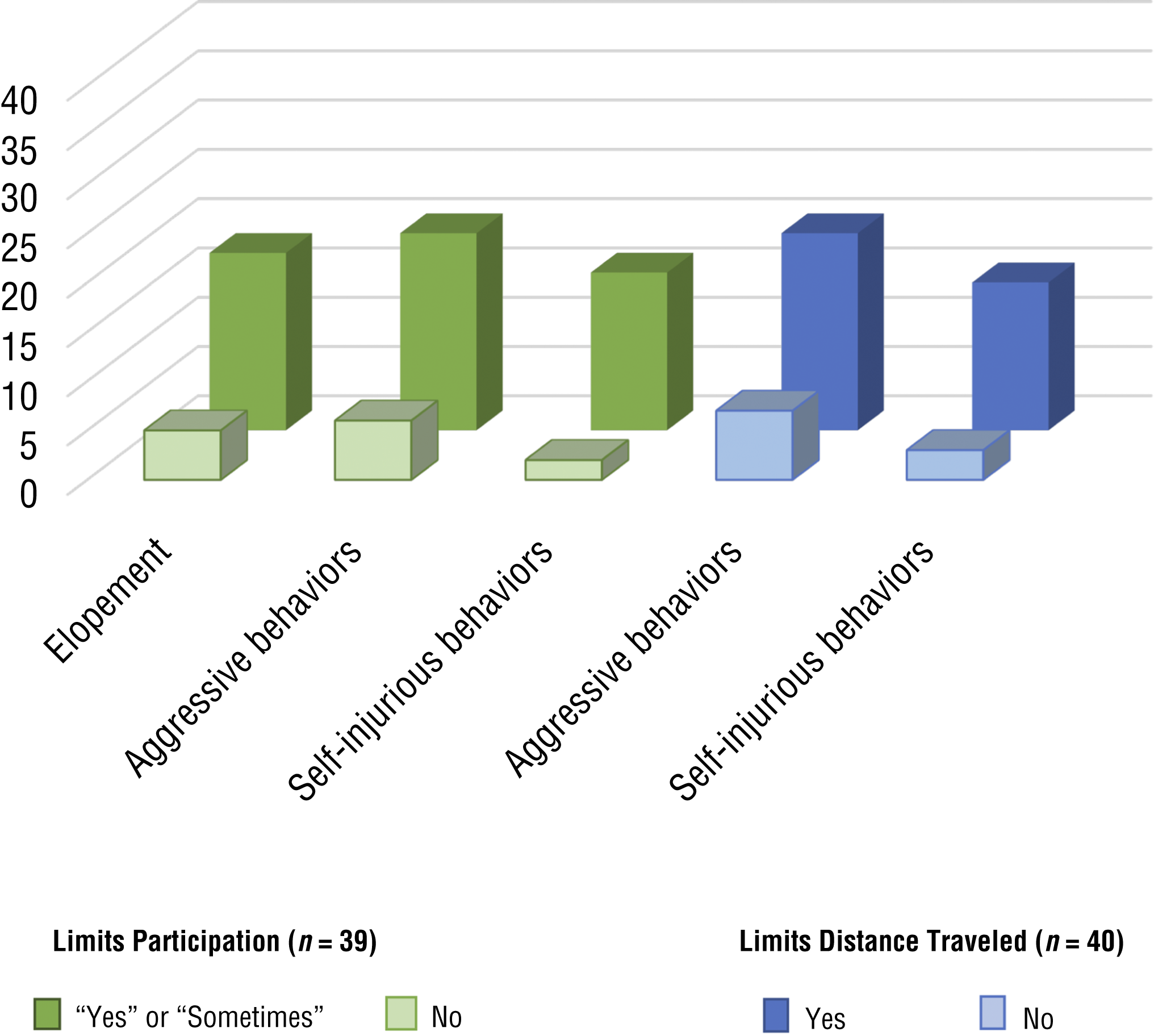
Relationship between behaviors and caregiver limitations on vehicular transportation.
Twenty-nine percent of respondents reported that their child had displayed self-injurious behavior during vehicular transportation. Statistically significant findings include a χ2 correlation indicating that caregivers (n = 39) were less likely to participate in activities away from home (yes or sometimes) if the child had attempted to elope (p = .013), displayed aggressive behaviors (p = .005), or had self-injurious behaviors (p = .001).
Participation
Caregivers were asked about their level of participation in activities that involved vehicular transportation. Of the participants, 60% (n = 40) reported limiting the distance that they travel with their child, with statistically significant χ2 correlations for limiting the vehicular distance traveled if the child displayed aggressive behaviors (p = .009) and self-injurious behaviors (p = .006; Figure 3). Statements from caregivers included “Never go too far from home in case something were to happen” and “We don’t leave the city and stay in the car as briefly as possible. I moved therapists because one was too far away and he would be having a meltdown by the time we got there.” Fifty-nine percent responded “yes” or “sometimes” to the question about deciding not to participate in activities that involve transportation. A caregiver stated, “Any events or activities that are more than 20 min in the car aren’t really feasible.”
Education
The respondents to this survey were asked about their education on CPS. Eighty-eight percent of caregivers stated that they used a seat belt 96% to 100% of the time when in a vehicle. When asked to elaborate on their choice, 1 respondent stated, “On bus, no seat belts,” and another stated, “I have to take it on and off so many times to reach into the backseat to handle things with the kids that I often don’t put it back on.” Eighty-seven percent of caregivers felt competent (yes or somewhat) in their ability to install a car seat. Fifty-five percent of respondents felt that resources, including both equipment and education, were available to them.
Relating to educational resources, 1 respondent stated, “I am not aware of any resources to help with my safety when driving my nephew.” Specifically relating to equipment, 1 respondent stated, “There may be resources but not easily accessible. . . . We had to buy everything on our own. If we didn’t have the devices, it would be extremely unsafe.” Another stated, “My eldest needs a safety vest as he is a flight risk; however, because of lack of accessibility to them we don’t have one.” The caregivers were asked where they purchased the car seats they used; 59% identified that the car seat they currently used was a personal purchase (new). Twenty-six percent responded that they did not use a car seat or CPS device. The remaining responses indicated that their device was covered by medical insurance, used, provided by an organization, or customized by a family member (2.6% each).
Caregivers were also asked to report where they acquired information on their car seat (or safety device). Twenty-seven percent identified that they acquired information from either a website or at the store where the seat was purchased. Seven percent responded that they acquired information from a therapist. Twenty-four percent indicated that they had not been provided information regarding car seats (or safety devices). Sixty-eight percent of respondents identified that they had not had their car seat inspected by a CPS technician.
Discussion
This study explored caregivers’ perceptions of transporting children with ASD. The behaviors identified by caregivers of children with ASD are consistent with those referenced in the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders, such as signs and symptoms of “persistent deficits in social communication and social interaction” and “restricted, repetitive patterns of behavior, interests, or activities” (APA, 2013, p. 50). Respondents stated that children displayed persistent maladaptive behaviors while being transported that limited both child and caregiver participation.
Our findings suggest that caregivers are more likely to limit the distance they travel if the child with ASD displays maladaptive behaviors. Limiting participation, engagement with friends, and social opportunities may contribute to social isolation and diminished overall quality of life for the child and family. In this study, we specifically asked how difficulties with personal transportation limits travel. More to the point, we were interested in knowing what level of awareness and understanding the participants had regarding specialized car safety seats designed for transport of children who elope or disrupt the driver.
Ninety-five percent of caregivers reported that their child displayed other distracting sensory modulation behavior (cold aggression), which is consistent with previous research but is new in the context of transportation. Fifty-eight percent of caregivers reported that their child has attempted to elope, a form of cold aggression. One caregiver stated, “My child has tried to get out of his seat in a moving vehicle many times. He would unfasten any restraints or wiggle out of them to move freely throughout the vehicle.”
Respondents reported that they had not been provided information or education regarding car seats. Many who felt that there were resources available still felt that these resources were not easily accessible. This finding is important because it underscores the disconnect between resources and education. Although resources may be available to these caregivers of children with ASD, they may still not receive appropriate education regarding CPS. This finding highlights the importance of occupational therapists’ role in advocacy and education regarding safe transport and sensory interventions and their ability to direct parents to resources to secure appropriate safety devices. Occupational therapists can obtain additional education to become car seat technicians and integrate this into their practice. Therapists can also obtain the names of local providers of this service and refer families to obtain an evaluation and recommendation.
Limitations
Several limitations of this study could affect the generalizability of the results. Data collected for this study were acquired from a small sample over a limited time period. Results were gathered using an internally created survey instrument; therefore, validity and reliability were not established. Because the survey was distributed through social media and other online platforms, respondents needed access to both a computer and the internet. Responses were received from a limited number of states and provinces (N = 17) and, therefore, fractionally represent the nation.
Implications for Occupational Therapy Practice
The findings of this study have the following implications for occupational therapy practice:
Occupational therapists should educate caregivers of children with ASD on the available resources and equipment that can address their child’s behavioral safety concerns and literature that supports the safe and effective use of these resources (American Occupational Therapy Association, 2020).
Occupational therapists who work with people with ASD should be familiar with CPS restraints, particularly for elopement; educate families on them; and advocate for their use.
The occupational therapy evaluation should include questions regarding vehicular transport, participation, and behavior concerns during car transportation.
In addition, occupational therapy curricula should include education on CPS for all children, and in particular for children with ASD.
Conclusion
Commonly reported behaviors displayed by children with ASD during transportation include elopement, distracting sensory behaviors, aggressive behaviors, and self-injurious behaviors. In addition, the findings suggest a correlation between caregivers limiting the distance traveled during vehicular transportation and participation in activities when transporting a child with ASD who displays behavioral safety concerns, including elopement, aggressive behaviors, and self-injurious behaviors. Our findings suggest that caregivers of children with ASD are more likely to experience decreased occupational participation, with the potential for social isolation. Although caregivers believe that resources are available to address these concerns, their responses indicate that obtaining these resources is difficult. It is within occupational therapy's scope of practice to address factors that affect community mobility and safety for caregivers and children.
Future research should include a similar study that addresses a larger demographic so that results can be more generalizable. In addition, research should be conducted to determine best-practice interventions that effectively address the behavioral safety concerns for children with ASD during transportation. We suggest that research should investigate how this area of practice is being addressed in occupational and physical therapy programs. Without this research, best-practice interventions cannot be successfully implemented to promote the safety and occupational well-being of caregivers and their children with ASD.