
Abstract
Dry needling was found to be an effective physical agent modality to decrease spasticity and increase ROM.
Dry needling is an emerging intervention with evidence of effectiveness as a treatment to improve range of motion (ROM) and reduce spasticity. It is termed dry needling because it involves the use of thin filiform needles and does not involve medication or injection. In a typical dry needling session, these thin needles are inserted into trigger points of targeted muscles and connective tissues with the aim of remediating muscle function and improving activity and participation (American Physical Therapy Association, 2013). Inactivating these trigger points loosens taut muscle bands (Ay et al., 2010). Once a needle has elicited a local twitch response (an involuntary spinal cord reflex in which the muscle fibers in the taut band of muscle contract), the needle is removed, and another needle is placed in a separate trigger point. This process is repeated until all trigger points in the target area have been addressed.
Dry needling is commonly associated with acupuncture; however, dry needling needles are inserted into the muscle, whereas acupuncture needles are inserted only at or below skin level (Furlan et al., 2005). In addition to helping to alleviate pain in the back, neck, and knee, acupuncture has been found to be helpful in reducing headaches and some symptoms resulting from cancer treatment (National Center for Complementary and Integrative Health, 2016). Unlike dry needling, acupuncture is based on the principles of traditional Chinese medicine, in which the disease is viewed as the result of disharmony in the body’s internal energy. Acupuncture is believed to restore balance to the flow of energy (Berman et al., 2010).
Dry needling has received growing interest from health professionals and has been the subject of several systematic reviews (Gattie et al., 2017; Griswold et al., 2019; Hall et al., 2018; Hu et al., 2018). The majority of published systematic reviews have addressed dry needling as an intervention for pain management, but analyses of its use to increase ROM and manage spasticity have not been reviewed. Despite the invasive nature of dry needling, it could qualify as an intervention to support occupations, which are defined in the Occupational Therapy Practice Framework: Domain and Process (4th ed.; American Occupational Therapy Association [AOTA], 2020) as “methods and tasks that prepare the client for occupational performance” (AOTA, 2020, p. 59). More specifically, it could be included under “physical agent and mechanical modalities” (AOTA, 2020, p. 59). Although AOTA does not have practice guidelines for dry needling, it has published a practice response stating that the AOTA Commission on Practice “does not have sufficient information at this time to assert that dry needling is part of occupational therapy practice” (AOTA, 2017b, para. 6). The purpose of this systematic review is to describe the published studies on dry needling to improve ROM and reduce spasticity and to discuss its potential for use in occupational therapy practice.
Previous research has indicated that improved ROM and decreased spasticity are related to increased independence in and improved performance of activities of daily living (ADLs) and instrumental activities of daily living (IADLs; Beissner et al., 2000; Bhimani et al., 2012; Cobian et al., 2013; Gates et al., 2016). ROM is an underlying body function that aids in completion of functional activities. ADLs and IADLs require ROM, which is why occupational therapy intervention commonly targets deficits in ROM (Cobian et al., 2013; Gates et al., 2016). Additional research by Beissner et al. (2000) has indicated that ROM is a predictor of ADL and IADL performance among older adults.
Bhimani et al. (2012) investigated the lived experiences of people with spasticity. Participants in their study reported impaired functional mobility and difficulty completing daily functions as a result of stiff muscles and unpredictable spasticity. They reported spending several hours on their morning routines because of spasticity and the fatigue that comes from the extra energy expended as a result of muscle jerking and tightness while completing these activities.
Previous systematic reviews involving dry needling have studied its effects on alleviation of myofascial pain in various parts of the body and have had variable results. A systematic review completed by Hu et al. (2018) concluded that dry needling is a more effective intervention to reduce low back pain than acupuncture. Another systematic review suggested that dry needling is more effective than sham therapy in reducing pain but, because of the low quality of the evidence, cannot be recommended over sham therapy or other interventions (Vier et al., 2019). In addition, a meta-analysis conducted by Hall et al. (2018) suggested that although several studies have supported the use of dry needling, there is still relatively little evidence to support these findings. These studies demonstrate a need for further research into the use of dry needling as a therapeutic intervention to relieve pain.
Recent research has also examined the effectiveness of dry needling on spasticity poststroke (Fakhari et al., 2017; Mendigutia-Gómez et al., 2016; Salom-Moreno et al., 2014; Sánchez-Mila et al., 2018). Additional studies have examined the effectiveness of dry needling specifically for increasing ROM in the neck, upper extremities, and lower extremities (Ay et al., 2010; Fakhari et al., 2017; Ga et al., 2007; Kamali et al., 2019; Kim et al., 2012; Martín-Rodríguez et al., 2019; Mejuto-Vázquez et al., 2014; Mendigutia-Gómez et al., 2016; Sánchez-Mila et al., 2018; Tabatabaiee et al., 2018). Despite the wealth of studies examining spasticity and ROM, no synthesis of information has been published to summarize the overall effectiveness of dry needling across studies.
As noted earlier, AOTA (2017b) recently stated that insufficient evidence exists to determine whether dry needling is within the scope of occupational therapy practice. If dry needling is found to be effective, the technique could be considered as a physical agent modality in a variety of occupational therapy intervention settings, including neurological clinics, outpatient rehabilitation, and inpatient rehabilitation. It could be used to increase functional capacity during sessions and improve client outcomes by increasing ROM and decreasing spasticity. It could thus contribute to clients’ increased participation in many of the occupations addressed by occupational therapy (AOTA, 2020). The purpose of this systematic review is to evaluate the evidence for the effectiveness of dry needling in reducing spasticity and increasing ROM. It summarizes the evidence for dry needling to determine whether it is adequate to support dry needling as an effective intervention for incorporation into occupational therapy practice.
Method
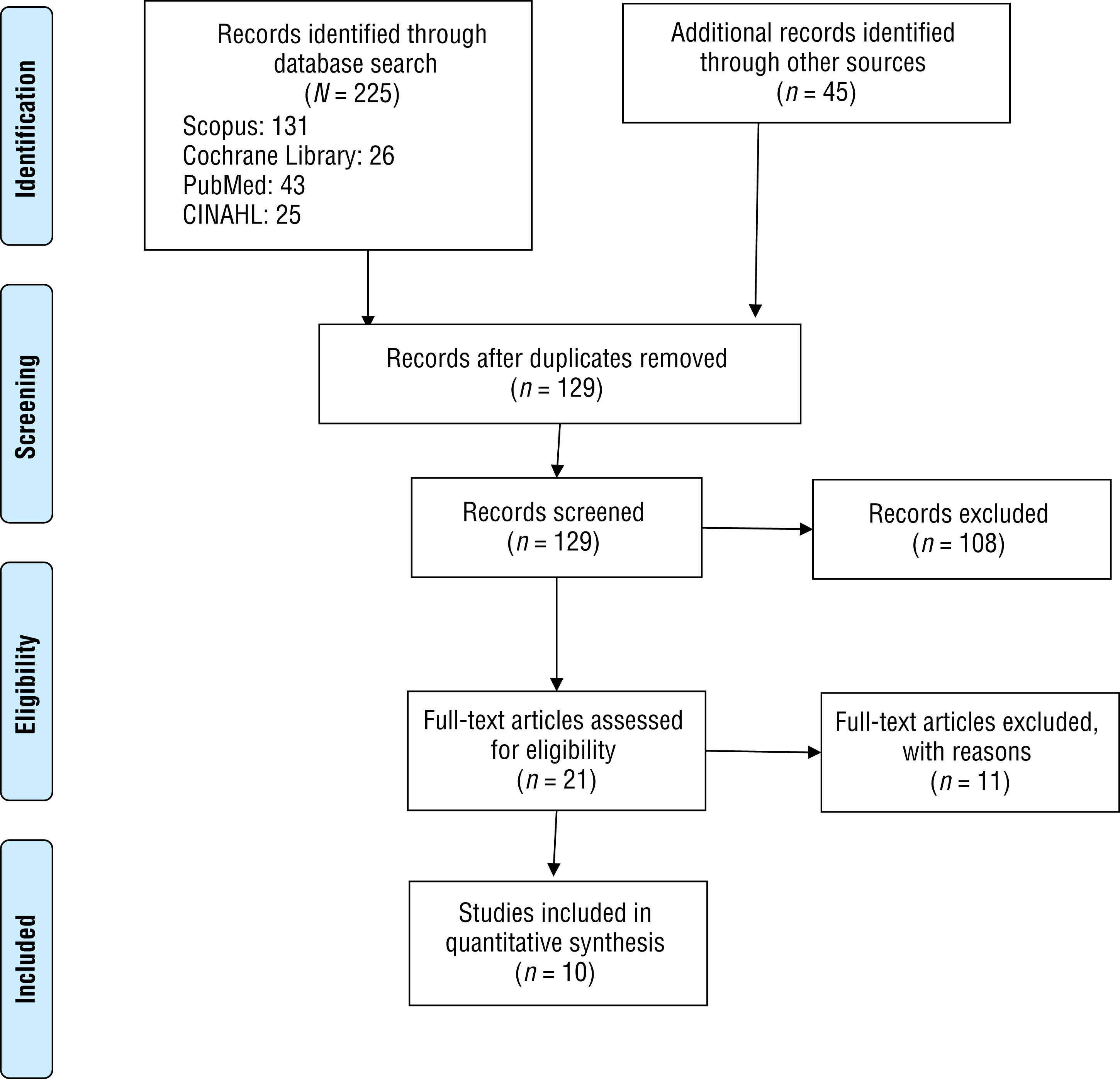
The search terms were determined by the first five authors, with guidance from the University of Texas Medical Branch library staff (Table 1). Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines were used as a model for this systematic review (Moher et al., 2009). We reviewed article citations and abstracts from Scopus, Cochrane Library, PubMed, CINAHL, and a university library search. These five authors reviewed the titles for all articles, and at least two authors independently reviewed each abstract to determine eligibility for inclusion in the review. After the abstract review, at least two authors reviewed the full text of each article to further determine eligibility. Any discrepancies found during the abstract or full-text review were discussed among these five authors, and a consensus was reached on whether to include the article in the review.
Search Terms
Inclusion criteria were as follows: peer-reviewed journal articles published in English between January 2007 (the earliest available studies) and October 2019. We also chose to include case series studies because of the limited availability of higher level evidence. The search included any rehabilitative therapy using dry needling and any variations of that therapy. We focused on the effects of dry needling on spasticity and ROM, and study outcomes were required to include outcomes related to measures of spasticity, hypertonia, or ROM. Search terms included functional dry needling, deep dry needling, dry needling, fdn (functional dry needling), needling, hypertonicity, spasticity, high tone, range of motion, ROM, muscle tightness, and joint mobility.
We excluded articles that examined acupuncture and other traditional Eastern medicine methods of needling, such as row and warm needling, because of the difference in methodology and reasoning. We also excluded studies that focused solely on pain or expert reviews of therapies; studies that focused on connective tissue disorders, such as adhesive capsulitis and anterior cruciate ligament repairs; studies that focused on the methodology of dry needling, such as the physiological mechanism; and studies that did not contain complete information regarding the study methods, participants, or outcomes to ensure a reliable, comprehensive review. Level IV and V studies were also excluded (AOTA, 2017a). Finally, we excluded studies that examined participants without a medical diagnosis and those in which treatment was not directly administered to the muscle that executed the movement being tested. Figure 1 displays the flow of articles through review.
All of the articles were reviewed according to the levels of evidence recommended by AOTA (2017a). Risk of bias was assessed for each of the included studies. Bias is an error in an experimental study that may affect its outcome. By assessing the risk of bias, we sought to determine the accuracy and reliability of the outcomes associated with a dry needling intervention. The types of bias screened for were selection bias, performance bias, detection bias, attrition bias, and reporting bias. To organize this information, we developed a risk-of-bias table using the format provided in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins et al., 2011).
Results
Ten studies were assessed to evaluate the effects of dry needling as an intervention to reduce spasticity and improve ROM. Of the 10 studies, 8 were Level I studies, and 2 were Level III studies. Although 8 studies provided Level I evidence, the diversity of intervention targets and outcome measures were too varied to complete a meta-analysis (Lipsey & Wilson, 2001). The studies are summarized in Table A.1 in the Appendix.
We examined all 10 studies for risk of bias in accordance with the methods described by Higgins et al. (2011; Table A.2). For random sequence generation, 1 study presented a high risk of bias because of the use of case series and single pretest–posttest study design (Fakhari et al., 2017). In addition, 5 studies had a high risk of allocation concealment bias (Fakhari et al., 2017; Ga et al., 2007; Kamali et al., 2019; Mendigutia-Gómez et al., 2016; Tabatabaiee et al., 2018). The most common risk of bias across the studies in this systematic review was performance bias. Blinding of participants and personnel was difficult to accomplish because of the invasive nature of the intervention. However, 3 studies presented a low risk of bias through use of blunt needling and different personnel to implement the intervention and assess outcome measures (Ga et al., 2007; Martín-Rodríguez et al., 2019, Mendigutia-Gómez et al., 2016). One study presented a high risk of attrition bias (Martín-Rodríguez et al., 2019). None of the studies presented a risk of reporting bias. Detection bias was assessed only for objective outcomes because the studies included in this systematic review did not use self-report measures. Three of the studies presented a high risk of bias for objective measure outcomes (Fakhari et al., 2017; Ga et al., 2007; Tabatabaiee et al., 2018), and 1 had an unclear risk of bias (Kamali et al., 2019).
We grouped studies by the outcome measures, the Modified Modified Ashworth Scale (Ansari et al., 2009), and ROM. Studies that addressed both spasticity and ROM were included in both categories. ROM was further divided into categories on the basis of the targeted body part.
Spasticity
Four studies, 2 Level I (Salom-Moreno et al., 2014; Sánchez-Mila et al., 2018) and 2 Level III (Fakhari et al., 2017; Mendigutia-Gómez et al., 2016), evaluated the effects of dry needling on spasticity in 109 poststroke patients. Each study used the MMAS (Ansari et al., 2009) to evaluate spasticity. Three of these studies found a significant decrease in spasticity after dry needling (Fakhari et al., 2017, Salom-Moreno et al., 2014; Sánchez-Mila et al., 2018), and 1 did not (Mendigutia-Gómez et al., 2016).
Cervical Range of Motion
Six studies, all Level I, examined the effects of dry needling on cervical ROM in 268 participants (Ay et al., 2010; Ga et al., 2007; Kamali et al., 2019; Martín-Rodríguez et al., 2019; Mejuto-Vázquez et al., 2014; Tabatabaiee et al., 2018). Cervical ROM was evaluated using a goniometer. Four studies demonstrated significantly improved cervical ROM after the intervention (Ay et al., 2010; Ga et al., 2007; Mejuto-Vázquez et al., 2014; Tabatabaiee et al., 2018). Of the studies that showed improved cervical ROM, 1 found that it did not increase cervical extension (Ga et al., 2007). Two studies did not show a significant increase in cervical ROM (Kamali et al., 2019; Martín-Rodríguez et al., 2019).
Upper Extremity Range of Motion
Two studies, both Level III, evaluated the effects of dry needling on upper extremity ROM in 49 participants (Fakhari et al., 2017; Mendigutia-Gómez et al., 2016). Upper extremity ROM was measured using goniometry and clinical observation. Participants in both studies demonstrated significantly improved upper extremity ROM after the intervention.
Lower Extremity Range of Motion
One Level I randomized controlled trial (RCT; Sánchez-Mila et al., 2018) examined the effects of dry needling on lower extremity ROM in 26 participants using the Fugl-Meyer Assessment. Participants demonstrated statistically significant improvements in ROM after the intervention.
Discussion
This systematic review examined the efficacy of dry needling as an intervention for reducing spasticity and improving ROM. A majority of the studies included participants with cardiovascular accident and myofascial pain syndrome because spasticity and decreased ROM are prevalent among people with these conditions. Several studies included people with generalized neck pain and tension-type headaches. Of the 10 studies reviewed, 8 were Level I, and 2 were Level III; thus, the overall level of evidence for the efficacy of dry needling in addressing ROM and spasticity is strong because it is supported by more than 2 well-designed Level I studies (AOTA, 2017a). Of the 10 studies, 4 demonstrated a significant decrease in spasticity, and 7 demonstrated a significant increase in ROM after administration of dry needling.
Of the 5 studies evaluating spasticity, only 1 did not show a significant improvement among participants after the dry needling intervention (Mendigutia-Gómez et al., 2016). Although the decrease in spasticity was not statistically significant, participants did experience a statistically significant improvement in ROM. It is possible that the MMAS may not have been sensitive enough to detect the changes in spasticity.
Of the 9 articles that addressed ROM, 2 did not show significant improvement among participants (Kamali et al., 2019; Martín-Rodríguez et al., 2019). Both studies were conducted with participants with either nonspecific neck pain or tension-type headaches. The inclusion criteria did not require that participants have abnormal muscle tone or decreased ROM at baseline, so it is possible that the participants in this study were already at their maximum range and could not improve further.
Strengths and Limitations
A strength of this systematic review is that most of the included studies were Level 1 RCTs. The studies included participants with a large range in age, and 9 had at least 20 participants. The studies were conducted in various settings (e.g., hospital, clinic, athletic training facility) and examined a range of different muscle groups (e.g., cervical, upper trapezius, hamstrings). All but 2 of the studies used random sequence generation, and none had attrition or reporting bias.
Weaknesses of this review include the lack of blinding of participants in many of the RCTs. Although some studies incorporated alternative methods as control conditions, such as the injection of a local anesthetic, most of the control groups received a completely different intervention or no intervention (Ay et al., 2010; Fakhari et al., 2017; Kamali et al., 2019; Mejuto-Vázquez et al., 2014; Mendigutia-Gómez et al., 2016; Salom-Moreno et al., 2014; Sánchez-Mila et al., 2018; Tabatabaiee et al., 2018). In addition, the comparison of dry needling with other physical agent modalities is limited. A few studies compared dry needling with other physical agent modalities, such as ultrasound; however, the majority had either no intervention for the control group or some form of exercise and stretching (Mendigutia-Gómez et al., 2016; Sánchez-Mila et al., 2018; Tabatabaiee et al., 2018). In addition, none of the studies were conducted by occupational therapists or examined functional occupational therapy outcomes. Finally, this review included 2 Level III studies (Fakhari et al., 2017; Mendigutia-Gómez et al., 2016), which are less rigorous because they do not include random group assignment; this should be considered when interpreting the findings.
Implications for Occupational Therapy Practice and Research
Dry needling has not yet been included in the occupational therapy scope of practice. As noted in the introduction, the Commission on Practice “does not have sufficient information at this time to assert that dry needling is part of occupational therapy practice” (AOTA, 2017b, para. 6). In addition, dry needling would be considered a physical agent modality, which requires additional education and training to be incorporated into occupational therapy interventions (AOTA, 2018). If dry needling were used in an occupational therapy setting, it would be used as part of or in preparation for an occupation-based activity.
The findings from this study have the following implications for occupational therapy practice:
The findings show strong evidence that the use of dry needling could improve ROM and spasticity and could be useful as an evidence-based physical agent modality to manage spasticity and improve ROM to support functional outcomes.
Dry needling may be an instrumental modality to improve occupational performance by addressing limited ROM and spasticity.
Dry needling has the potential to help clients perform functional occupations, and it could be a valuable addition to the modalities used in occupational therapy practice.
Current occupational therapy research examining dry needling is limited. Implications for future research may include studies that examine the effects of dry needling on occupational performance. Current rehabilitation research has most commonly looked at the effects of dry needling on people who have had a stroke. Future studies are needed to examine a broader range of conditions affected by spasticity and subsequent loss of ROM, including cerebral palsy, brain injury, multiple sclerosis, or amyotrophic lateral sclerosis. Research is also needed to compare dry needling with less invasive treatments, such as electrical stimulation (Howlett et al., 2015). Both treatments have been shown to reduce muscle tightness, but it is not clear which is more effective. Future studies are also needed to examine the effects of dry needling on a broader range of diagnoses, the impact of dry needling on occupational performance, and the comparison of this intervention with less invasive treatments.
Conclusion
This systematic review examined the efficacy of dry needling as an intervention to decrease spasticity and improve ROM. The purpose was to better understand the benefits of dry needling and its possible use as an occupational therapy intervention. We found strong evidence to support the use of dry needling to target spasticity and active and passive ROM.
Footnotes
Acknowledgments
The authors thank Janet Burk at the University of Texas Medical Branch library for her help with the literature search.
Appendix
Risk-of-Bias Table for Studies Included in the Systematic Review
| Citation | Selection Bias | Performance Bias: Blinding of Participants and Personnel | Detection Bias | Attrition Bias: Incomplete Outcome Data | Reporting Bias: Selective Reporting | ||
| Random Sequence Generation | Allocation Concealment | Blinding of Outcome Assessment: Self-Reported Outcomes | Blinding of Outcome Assessment: Objective Outcomes | ||||
| Ay et al. (2010) | + | + | − | N/A | + | + | + |
| Fakhari et al. (2017) | − | − | − | N/A | − | + | + |
| Ga et al. (2007) | + | − | + | N/A | − | + | + |
| Kamali et al. (2019) | + | − | − | N/A | ? | + | + |
| Martín-Rodríguez et al. (2019) | + | + | + | N/A | + | − | + |
| Mejuto-Vázquez et al. (2014) | + | + | − | N/A | + | + | + |
| Mendigutia-Gómez et al. (2016) | + | − | + | N/A | + | + | + |
| Salom-Moreno et al. (2014) | + | + | − | N/A | + | + | + |
| Sánchez-Mila et al. (2018) | + | + | − | N/A | + | + | + |
| Tabatabaiee et al. (2018) | + | − | − | N/A | − | + | + |
Note. Categories for risk of bias: + = low risk of bias; ? = unclear risk of bias; − = high risk of bias. N/A = not applicable. Risk-of-bias table format adapted from “Assessing Risk of Bias in Included Studies,” by J. P. T. Higgins, D. G. Altman, and J. A. C. Sterne, in Cochrane Handbook for Systematic Reviews of Interventions (Version 5.1.0), by J. P. T. Higgins and S. Green (Eds.), 2011. http://www.cochrane-handbook.org. Copyright © 2011 by The Cochrane Collaboration.
*Indicates studies included in the systematic review.