
Abstract
Occupational therapy expertise paired with video modeling can provide meaningful support to work occupations.
Autism spectrum disorder (ASD) is a lifelong social, communication, and behavioral condition affecting global occupational engagement (American Psychiatric Association [APA], 2013). Approximately 31% of people with ASD have co-occurring intellectual and developmental disability (IDD), with an IQ of ≤70, whereas 24% of people are within the borderline IQ range of 71 to 85 (APA, 2013; Christensen et al., 2018). Currently, costs related to the care for adults with ASD in the United States range between $136 and $196 billion dollars annually (Buescher et al., 2014). In addition, adolescents and adults with ASD experience difficulties in developing work skills for employment acquisition and job performance, resulting in high unemployment rates (Gentry et al., 2015; Holwerda et al., 2012).
Without having a means to earn a living wage, people with ASD are often financially dependent on caregivers, which can affect quality of life (Holwerda et al., 2012; Piven & Rabins, 2011). Given the complex spectrum of ASD with co-occurring IDD, it is essential to have effective, strengths-based interventions (Steinbrenner et al., 2020). Visual learning tends to be an area of relative strength, whereas auditory processing can be a deficit area for people with ASD (Hess & Chitwood, 2018; Rao & Gagie, 2006). Therefore, interprofessional interventions, including occupational therapy, are needed to promote strengths and implement evidence-based programming addressing work skills (Marsack & Perry, 2018; Rattaz et al., 2017).
Occupational therapy practitioners focus intervention on engagement in meaningful daily occupations. The Occupational Therapy Practice Framework: Domain and Process (4th ed.; OTPF–4; American Occupational Therapy Association [AOTA], 2020) defines occupation as “personalized and meaningful engagement in daily life events by a specific client” (p. 7). Work is one of the nine occupations defined by the OTPF–4 and includes employment interests and pursuits, employment seeking and acquisition, job performance, retirement preparation and adjustment, and volunteer exploration and participation (AOTA, 2020). Occupational therapy practitioners use many intervention strategies, including modeling, hand over hand, and one-on-one instruction. Yet, these techniques often include verbal cuing, therefore requiring auditory processing, which tends to be an area of relative deficit for people with ASD (Tomchek & Dunn, 2007). Practitioners also use assistive technology (AT) as an intervention approach that is within the scope of occupational therapy practice (AOTA, 2020). Specifically, video modeling (VM) is a form of AT that is visually centered and is therefore a strengths-based intervention for most people with ASD (Franzone & Collet-Klingenberg, 2008; Steinbrenner et al., 2020).
Video Modeling and Occupations
VM is defined as “a mode of teaching that uses video recording and display equipment to provide a visual model of the targeted behavior or skill” (Franzone & Collet-Klingenberg, 2008, p. 1). Research has indicated that effective VM for those with ASD includes customization to the client (e.g., filming the user themselves or a familiar adult engaged in the activity, filming in familiar settings with familiar items), concrete language, a deliberate delivery speed, and motivation for task completion (Campbell et al., 2015; Mechling & Gustafson, 2008; Rao & Gagie, 2006). Videos can be viewed in advance of task performance or while engaged in the activity. Moreover, VM can be slowed down, paused, rewound, and viewed on a range of mainstream devices, including tablets, computers, and smartphones (Hess & Chitwood, 2018; Mechling & Gustafson, 2008).
VM was found to be beneficial in interdisciplinary research across various occupations, including activities of daily living, instrumental activities of daily living, and social participation, for people with ASD (Franzone & Collet-Klingenberg, 2008; Hong et al., 2016; Steinbrenner et al., 2020; Wertalik & Kubina, 2018). Specifically, occupational therapy intervention implementing VM has been studied in social and daily living skills for children and adolescents with ASD (Campbell et al., 2015; Meister & Salls, 2015; Stewart & Umeda, 2014). VM for work occupations has also been researched; however, far fewer studies are available (Allen, Wallace, Greene, et al., 2010; Allen, Wallace, Renes, et al., 2010; Burke et al., 2013; Hayes et al., 2015; Kellems & Morningstar, 2012; Walsh et al., 2018). Moreover, little research on VM has been conducted by occupational therapy practitioners, particularly research focused on work occupations.
Therefore, the purpose of this systematic review was to examine the state of the evidence on VM for people with ASD during work occupations. The research team was a collaboration between an occupational therapy university faculty member with extensive intervention and research experience in ASD, AT, and VM in partnership with two honors occupational therapy graduate students. Together, we formatted a participants, interventions, comparisons, outcomes, and study designs (PICOS) guiding question on the basis of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist (Moher et al., 2009). We used the following research question: What is the state of the evidence of VM as a therapeutic modality to support engagement in work occupations for adolescents and adults with ASD across the spectrum, including people with co-occurring IDD?
Method
For this systematic review, we followed the PRISMA checklist (Moher et al., 2009). We met routinely over the course of several months to determine inclusion and exclusion criteria and to review the collected articles. An experienced university research librarian was consulted multiple times while we were designing, implementing, and revising the search for depth and rigor. The following online research databases were searched: Cochrane Collection Plus, CINAHL, PubMed, ERIC, and ProQuest. In addition to the databases, we reviewed occupational therapy sources, including the American Journal of Occupational Therapy and Chapter 6 in the Occupational Therapy Practice Guidelines for Individuals With Autism Spectrum Disorder (Tomchek & Koenig, 2016). We extracted data according to the PRISMA guidelines, including the field of study, level of evidence, research design, measures and operational definitions, relevant results, conclusions, limitations, implications of the study, area of occupation, and device used for VM supporting work occupations. We held multiple meetings over several months to review the process validity, determine manuscript eligibility, assess for bias, and reach consensus after detailed article review and discussion.
Inclusion and Exclusion Criteria
We considered all levels of evidence that examined the implementation of VM for people with ASD, including those with co-occurring IDD, who were age 16 yr or older during work occupations categorized by the OTPF–3 (AOTA, 2014). The articles were included if they were written in English, available for free full-text review, and published between 2008 and 2018 to account for more recent technology. The age limit was selected to be inclusive of average teen and adult working ages ranging from 16 to 64 yr. The following search terms were used: autism, ASD, autism spectrum disorder, occupational therapy, and video modeling. Search terms were intentionally broad to be inclusive of the work categories provided by the OTPF–3. We reviewed articles obtained using the aforementioned search terms to determine whether work occupations were included. Studies were included if the entire sample of the study had a primary diagnosis of ASD, as defined by the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM–5; APA, 2013), or Asperger syndrome, Rett syndrome, childhood disintegrative disorder, and pervasive developmental disorder–not otherwise specified according to the DSM–IV (text rev.; APA, 2000), given the years of study inclusion.
Studies were excluded if they did not meet the inclusion criteria or were qualitative studies, meta-analyses, or systematic reviews. Any pertinent meta-analysis or systematic review references were reviewed for original articles that fit the inclusion criteria. We found and examined studies pertaining to employment seeking and acquisition, in addition to job performance, because other OTPF–3 work categories were not found during the search. Moreover, studies were excluded if they did not use measurement of work occupations as an outcome measure or focused on other non–work related occupations. We also excluded non–peer-reviewed publications, dissertations, theses, and conference posters or presentations. On the basis of these inclusion and exclusion criteria, a risk of author bias is possible across studies at both the study and outcome levels.
Analysis
The systematic review process consisted of a collaborative approach and multiple rounds of analysis. First, titles and abstracts were reviewed and evaluated for inclusion criteria. Next, studies were reevaluated to determine alignment with outcome measures focused on work occupation task analyses and skill improvement based on VM intervention. Then, a literature review spreadsheet was created to track articles for levels of evidence, inclusion and exclusion criteria and key themes related to the participant population, how the VM was designed and used, and work occupation outcomes. The levels of evidence criteria were based on AOTA’s (2017) systematic review guidelines and the Oxford Centre for Evidence-Based Medicine’s (2016) system of five levels of evidence (Sackett, 1989).
We completed “Table 8.5a: The Cochrane Collaboration Tool for Assessing Risk of Bias” from the Cochrane Handbook for Systematic Reviews of Intervention (Version 5.1.0; Higgins et al., 2011) independently and used the handbook as a reference. The independently generated tables were then reviewed and discussed.
The analysis revealed VM as a beneficial intervention to support work occupations at a moderate level of certainty (AOTA, 2017). Results include the following findings: Participants’ age and IQ were varied; the VM style, platform, and viewing frequency were varied; work skills acquisition was the primary outcome measure for VM intervention effectiveness; additional outcome measures for VM included social skills improvement rating scales and various social validity measures; and research designs were primarily Level 4.
Results
The PRISMA flow diagram is shown in Figure 1. A total of 245 records were identified through database searches, and an additional 229 records were identified through other sources (Moher et al., 2009). After 10 duplicates were considered and removed, 464 articles were screened for inclusion and exclusion criteria. Records were excluded during initial title and abstract screening if the study included children with ASD younger than age 16 yr, nonwork occupations, or people lacking ASD as a primary diagnosis. A total of 31 full-text articles were screened for eligibility, and 6 met the full inclusion criteria. Four of the 6 studies were quantitative, whereas 2 studies were mixed methods. As can be seen in Figure 1, full-text articles were excluded if they did not examine VM as an intervention (n = 1), focus on work skill acquisition (n = 1), mention the use of VM (n = 4), have participants with ASD as a primary diagnosis (n = 4), and focus on work occupations (n = 15). Summaries of the 6 studies can be found in Table A.1 in the Appendix.
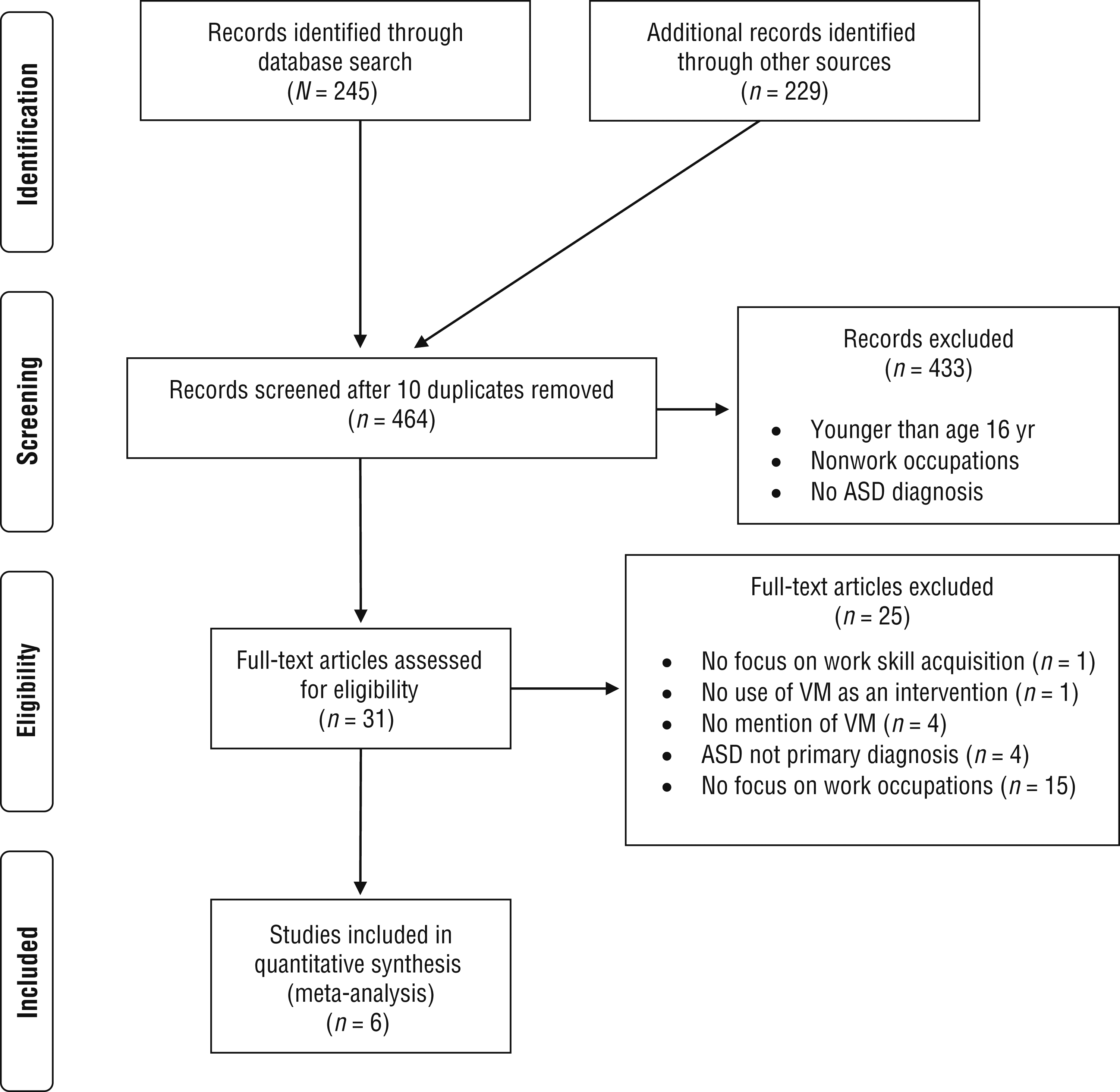
Flow diagram for inclusion and exclusion of peer-reviewed studies in the systematic review.
Evidence Table for the Systematic Review of Video Modeling Use in Work Occupations for People With Autism
Note. ACCESS = Adolescent Curriculum for Communication and Effective Social Skills; ASD = autism spectrum disorder; RCT = randomized controlled trial; SRS–2 = Social Responsiveness Scale–Second Edition; SSiS–RS = Social Skills Improvement System–Rating Scale; TEI–SF = Treatment Evaluation Inventory–Short Form; VM = video modeling.
Key Findings for Video Modeling and Work Occupations
The evidence from the 6 studies suggests that VM facilitates work occupations for people with ASD with a moderate level of certainty. Our results are presented next in response to the PICOS research question.
Participants
Across the studies, demographic characteristics showed that participants’ ages ranged from 17 to 28 yr, participants were 86.49% male, and IQ standard scores ranged from 38 to 112.
Intervention
The design and implementation of VM varied across the 6 studies. Variations included the device used to watch the VM, the video style, and the frequency of VM use.
Devices.
Participants used various devices to watch VM, including the Samsung Galaxy Tab® (Burke et al., 2013), iPod Touch® (Hayes et al., 2015), video iPod® (Kellems & Morningstar, 2012), and other iOS® devices (Hayes et al., 2015). Some studies did not specify the device used (Allen, Wallace, Greene, et al., 2010; Allen, Wallace, Renes, et al., 2010; Walsh et al., 2018).
Video style.
Studies also had variations in video style, including scripted videos (Allen, Wallace, Greene, et al., 2010; Hayes et al., 2015; Walsh et al., 2018), videos in the naturalistic work setting (Allen, Wallace, Greene, et al., 2010; Allen, Wallace, Renes, et al., 2010), video with step-by-step directions (Burke et al., 2013), videos of a familiar person (Kellems & Morningstar, 2012), and video perspective—what the person completing the task sees (Allen, Wallace, Greene, et al., 2010; Allen, Wallace, Renes, et al., 2010) in contrast to the perspective of someone watching the task being completed (Allen, Wallace, Greene, et al., 2010; Allen, Wallace, Renes, et al., 2010; Burke et al., 2013; Hayes et al., 2015). A final video style variation was VM customized for each participant in the sample and their personal work tasks (Kellems & Morningstar, 2012). Videos included both correct examples and incorrect examples of the targeted behaviors (Walsh et al., 2018).
Frequency of video modeling use.
Finally, frequency of VM use varied. In some instances, participants watched a video once and then retried a work task after a specified period of time (Allen, Wallace, Greene, et al., 2010; Allen, Wallace, Renes, et al., 2010; Walsh et al., 2018), whereas others were asked to watch the videos as many times as needed within a specified time frame before data collection of the outcome measurement (Burke et al., 2013; Hayes et al., 2015; Kellems & Morningstar, 2012).
Comparisons and Outcomes
Increased work performance was measured by skill acquisition measures (e.g., percentage of steps correctly performed) in 4 of the 6 studies (Allen, Wallace, Greene, et al., 2010; Allen, Wallace, Renes, et al., 2010; Burke et al., 2013; Kellems & Morningstar, 2012). In the other 2 studies, interview skills necessary for employment seeking and acquisition were measured (Hayes et al., 2015; Walsh et al., 2018). The 2 studies that included a follow-up assessment found that participants were able to generalize and retain the work skills (Allen, Wallace, Greene, et al., 2010; Allen, Wallace, Renes, et al., 2010).
Work performance.
Four studies demonstrated an increase in work performance after VM interventions (Allen, Wallace, Greene, et al., 2010; Allen, Wallace, Renes, et al., 2010; Burke et al., 2013; Kellems & Morningstar, 2012). Employer-determined criteria were used in 3 studies in comparison with baseline (Allen, Wallace, Greene, et al., 2010; Allen, Wallace, Renes, et al., 2010; Burke et al., 2013). Kellems and Morningstar (2012) measured the increased percentage of steps correctly completed and found maintenance of skills up to 30 days.
Employment acquisition and seeking.
Two studies examined improvement in interview skills (Hayes et al., 2015; Walsh et al., 2018). In Hayes et al.’s (2015) study, participants were randomized into a VM intervention group and a control group. Post-VM interview skills were assessed on a scale ranging from 1 (poor) to 4 (excellent) across six categories—presentation, preparation for the interview, verbal communication/content of answers, interpersonal skills, desire/interest, and skill level—with significant improvements found for the intervention group. The following additional observational improvements were noted: decreased fidgeting, increased interview hygiene, and improved formulation of clear and succinct answers.
Walsh et al. (2018) found improvement of social communication skills necessary for employment as measured by scores from the Adolescent Curriculum for Communication and Effective Social Skills placement test, the Social Responsiveness Scale–Second Edition, the Social Skills Improvement System–Rating Scale, and targeted researcher probes comparing baseline with post-VM intervention.
Follow-up assessment.
Three studies conducted follow-ups (Allen, Wallace, Greene, et al., 2010; Allen, Wallace, Renes, et al., 2010; Walsh et al., 2018). Allen and colleagues (Allen, Wallace, Greene, et al., 2010; Allen, Wallace, Renes, et al., 2010) conducted a 1-mo follow-up and found that 5 of the 8 total participants were able to maintain skills acquired during VM intervention. Allen, Wallace, Greene, et al. (2010) additionally assessed at a 3-mo follow-up and found that all participants were able to generalize skills to a novel task. Walsh et al. (2018) conducted a 3-mo follow-up and found that most treatment gains were maintained. Additionally, after completion of the study, participants reported participating in employment and job interviews.
Inconsistent measures of social validity.
Five of the 6 studies included social validity as an outcome measure; however, no consistent operational definition or outcome measure was used across the studies for social validity related to VM as an intervention (Allen, Wallace, Greene, et al., 2010; Allen, Wallace, Renes, et al., 2010; Burke et al., 2013; Kellems & Morningstar, 2012; Walsh et al., 2018). Burke et al. (2013) used questionnaires for participants and parents to measure acceptability of the VM software, VM effectiveness, and whether VM would be recommended to support people with ASD. Walsh et al. (2018) also used questionnaires for participants, parents, and teachers about social skills training and satisfaction. Kellems and Morningstar (2012) analyzed qualitative data from participants, job coaches, and employers and reported themes of helpfulness, enjoyment, and social acceptance of VM. Hayes et al. (2015) also used qualitative methods to learn about VM use and noted participant comments about feeling more confident. In contrast to VM application and effective social validity outcomes, Allen and colleagues (Allen, Wallace, Greene, et al., 2010; Allen, Wallace, Renes, et al., 2010) defined social validity as the participants’ comfort and acceptance of the job itself from questionnaires and anecdotal comments.
Study Designs
In each of the 6 studies, quantitative methods were central to the research designs. One study was a randomized controlled trial, making it a Level I study, whereas the remaining 5 studies were multiple baseline studies, categorized as Level IV studies. In the Level I study, the sample was randomized into one VM intervention group and one control group. In the 5 Level IV studies, participants received a baseline pretest and multiple comparison post-VM intervention tests. Hayes et al. (2015) and Kellems and Morningstar (2012) additionally included qualitative measures within their studies. Across the studies, the sample sizes ranged from N = 3 to N = 8.
Risk of Bias
The 6 studies reviewed were assessed for risk of bias according to Higgins et al.’s (2011) risk-of-bias table format. We collaborated and came to consensus on the risk-of-bias ratings. Discrepancies were resolved through discussion and detailed article review until an agreement was met (Table A.2). One study had a low risk of bias for random sequence generation, allocation concealment, and blinding of participants and personnel (Hayes et al., 2015), whereas the other studies did not have multiple groups (Allen, Wallace, Greene, et al., 2010; Allen, Wallace, Renes, et al., 2010; Burke et al., 2013; Kellems & Morningstar, 2012; Walsh et al., 2018). In terms of self-reported outcomes, 2 studies had a low risk of bias (Burke et al., 2013; Kellems & Morningstar, 2012), 3 studies had a high risk of bias (Allen, Wallace, Greene, et al., 2010; Hayes et al., 2015; Walsh et al., 2018), and the level of bias in 1 study was unclear (Allen, Wallace, Renes, et al., 2010). Five studies had a low risk of bias for both selective reporting and incomplete outcome data (Allen, Wallace, Renes, et al., 2010; Burke et al., 2013; Hayes et al., 2015; Kellems & Morningstar, 2012; Walsh et al., 2018), whereas the level of bias was unclear in 1 study (Allen, Wallace, Greene, et al., 2010). All 6 studies had a low risk of bias for blinding of objective outcomes.
Risk-of-Bias Table for Studies Included in the Systematic Review
Note. Categories for risk of bias: + = low risk of bias; ? = unclear risk of bias;
Discussion
This systematic review has revealed a moderate level of certainty that VM supports work occupations for people with ASD according to the definitions in AOTA’s (2017) guidelines for systematic reviews. Of the 6 studies, 1 is a Level I study, whereas 5 are Level IV studies. The limitations of this systematic review include small sample sizes across all 6 studies examined and screening exclusively of free full-text articles on the basis of our university library database access. Clearly, increased research is needed given the potential of VM and the limited levels of current evidence.
Across the studies, adults with ASD ages 17 to 28 yr with a range of IQ (from typical IQ to moderate IDD) benefited from VM as an intervention to support a variety of work occupations. However, the combined samples were 86.49% male, a proportion larger than in the general population of people with ASD, found to be approximately 75% male (Loomes et al., 2017). Although the actual male-to-female ratio of these combined samples differs slightly, it is consistent with the higher prevalence of ASD in men and boys. Moreover, these samples, with a maximum age of 28 yr, do not represent a large portion of the working-age population. This relatively young maximum age may be attributable to a recent and needed emphasis on school-to-work transitions. Therefore, future research should include adults with a broader age range. A powerful result was the wide IQ range represented in the sample (standard scores from 38 to 112), suggesting that VM can be effective across the spectrum of cognitive abilities.
The VM intervention used across the 6 studies varied greatly. Devices, video style, and the frequency and amount of viewing were customized to each study. Additionally, outcome measures were specific to the work occupation being studied. Despite differences in the design, implementation, and measurement of VM, positive outcomes for a variety of work occupations were found across the 6 studies, including in follow-up assessments. This variation is not a limitation but rather is supportive of VM as a client- and occupation-centered approach.
Finally, participants, parents, managers, and job coaches expressed predominantly positive remarks about VM, indicating that it is both effective and socially acceptable in the workplace. This finding is important because it illustrates that VM is an intervention that will likely be implemented. Notably, some participants obtained employment and participated in interviews after VM interventions (Walsh et al., 2018). Given that people with ASD are underemployed (Holwerda et al., 2012), VM can improve meaningful engagement in work occupations for this population.
Implications for Occupational Therapy Practice
VM is an interdisciplinary evidence-based practice (Steinbrenner et al., 2020). The use of VM by occupational therapy practitioners has been well established for younger clients and for occupations such as activities of daily living and social participation (Franzone & Collet-Klingenberg, 2008; Hong et al., 2016; Wertalik & Kubina, 2018). This systematic review establishes a clear rationale for the use of VM as a therapeutic modality to support engagement in work occupations for adolescents and adults with ASD across the spectrum, including people with co-occurring IDD. The results of this review have the following implications for occupational therapy practice:
• Effective VM varies in style and implementation.
− VM does not need to follow a prescribed formula for it to be beneficial to a spectrum of clients. Therefore, it aligns with individualized, strengths-based, client-centered care, which is a cornerstone of occupational therapy intervention.
− VM can be effective with a variety of video styles (e.g., filming point of view, scripted videos, use of a familiar person) and devices for a range of clients.
− VM implementation can be customized. For example, the client may benefit from frequent viewing or from use of VM for preteaching a task or while completing a task.
− VM outcomes may include acquisition, maintenance, and generalization of skills.
• VM is socially acceptable.
− The social acceptability of mainstream technology, including smartphones, tablets, and computers, affords individualized support with less stigma.
− VM was positively received by those with ASD as well as job coaches, supervisors, and managers. Occupational therapy practitioners frequently collaborate and consult with these professionals to customize intervention plans. Therefore, when the interprofessional team feels that an intervention is beneficial, it is more likely to be implemented and sustained.
Conclusion
Currently, research on VM, ASD, and work occupations is promising yet limited. VM can support engagement in work occupations by people across the spectrum of ASD. However, more research is needed focusing on the working population, including those older than age 28 yr. Therefore, it is essential that occupational therapy practitioners become versed in the benefits of VM and contribute to VM intervention evidence as applied to occupational engagement.
Footnotes
Acknowledgments
We thank Julia Wilbarger, PhD, OTR/L, Caroline Umeda, PhD, OTR/L, Gina Tucker-Roghi, OTD, OTR/L, and Lynn Sondag, MFA, for their valuable feedback on this work. We additionally acknowledge Michael Pujals, Scholarly Communications Librarian, for his guidance and expertise. We also thank the Department of Occupational Therapy at Dominican University of California for their ongoing encouragement and support.
*
Indicates studies included in the systematic review.