
Abstract
Using the ICF to understand care partners’ problems after a sudden-onset condition may provide crucial insight needed to develop effective self-management interventions for care partners in the future.
In the United States, more than 65 million people provide informal care to a person with a chronic illness or disability (National Alliance for Caregiving, 2009). The National Institutes of Health has defined these informal caregivers, or care partners, as “unpaid individuals (spouses, partners, family members, friends, or neighbors) involved in assisting others with activities of daily living and/or medical tasks” (“Promoting Caregiver Health Using Self-Management,” 2017, “93.361” section, para. 1). Often it falls to care partners to provide physical, emotional, and psychosocial support after discharge from inpatient settings, despite their having limited or no caregiving training. Care partners not only provide direct care to people with chronic conditions, but they must also manage their own lives, including the complex dyadic relationship they have with the care recipient (Centers for Disease Control and Prevention [CDC], 2015).
Care partners provide support to people with a multitude of conditions, including, but not limited to, traumatic injuries such as traumatic brain injury (TBI), spinal cord injury (SCI), or burn injury, and other sudden-onset conditions such as stroke. In the United States, more than 5 million people (approximately 2% of the U.S. population) currently live with TBI-related disability (CDC, 2015); approximately 282,000 have SCI-related disability (National Spinal Cord Injury Statistical Center, 2016); as many as 50% of people with burn injury experience associated disability (American Burn Association, 2016); and about 7 million people have stroke-related disability, which is projected to increase by an additional 4 million by 2030 (Roger et al., 2012).
Current understanding of the effects of being a care partner has predominantly been derived from studies of care partners of older adults, particularly those with dementia. Care partners of older adults who provide substantial help with health care are significantly more likely to experience emotional, physical, and financial difficulty than care partners who provide no help (Wolff et al., 2016). The extent to which care partners perceive that their caregiver duties result in adverse effects on their overall functioning is known as caregiver burden (Zarit et al., 1986) and is referred to by the World Health Organization (WHO; 2001) as third-party disability.
Although caregiver issues in dementia have been well examined, there has been far less exploration of the issues faced by care partners of people who experience a sudden-onset condition, especially early in the rehabilitation process while the care recipient is still on an inpatient unit (Lilly et al., 2014). These care partners experience a sudden, high-impact event without warning and with little time to prepare for what is often a life-altering situation. Their ability to cope and problem solve, as well as their psychological and physiological responses to stress, may differ from those who experience a more gradual transition into a care partner role (Saban et al., 2010). Care partners of those with a sudden-onset condition routinely report feeling untrained and unprepared to manage the care of a loved one at the time of transition from hospital to home (Adelman et al., 2014). They report inadequate support from health care providers and feelings of abandonment by the health care system (Lilly et al., 2012) This caregiver burden is typically assessed weeks or months after the sudden-onset condition, and thus researchers are largely unaware of the problems and concerns experienced by care partners during the initial days after a traumatic event (Baker et al., 2017). Therefore, an understanding of the obstacles and concerns faced by care partners in the days, rather than months, after a sudden health event may provide the foundational knowledge necessary to develop effective care partner interventions.
WHO’s (2001) International Classification of Functioning, Disability and Health (ICF) has been used primarily to classify and describe disability and functioning of patient populations (Cieza et al., 2016). However, it is a universal document designed to classify and describe the health and functioning of all people. In the ICF’s “Annex 8: Future Directions for the ICF,” WHO has specifically proposed using the ICF to better understand and meet the needs of care partners. To this end, the ICF has been used to classify and describe the impact of aphasia and hearing impairment on care partners (Grawburg et al., 2013), yet it has not been used to explore the health and health-related issues of care partners of people in other patient populations.
Therefore, in line with WHO’s (2001) call for the application of the ICF to the care partner population and to address the lack of knowledge about care partner needs early in the rehabilitation process, we performed a retrospective analysis of care partner–reported problems using the ICF linking technique. Our aim was to link, classify, and describe care partner–reported problems to explore the experiences of care partners early in the rehabilitation process.
Method
The data used in this study were collected as part of a parent study exploring the feasibility and early efficacy of a self-management problem-solving intervention—Problem-Solving Training (PST)—initiated with care partners (n = 9) of patients with TBI, SCI, burn injury, or stroke during the care recipient’s inpatient rehabilitation care. The parent study methodology can be found in Juengst et al. (2019). Care partner inclusion criteria were (1) ≥1 yr relationship with care recipient, (2) fluent in English, (3) capacity to consent, and (4) ownership of a smartphone. The study allowed for one care partner per care recipient.
As part of the first session of the 1:1 care partner PST, care partners complete a worksheet designed to help them brainstorm problems they experience while their loved one is admitted to the hospital. Care partners are encouraged to include problems they are experiencing of any nature; that is, the problems do not have to be directly related to caregiving or the care recipient. The worksheet provides general prompts such as “problems with relationships” or “problems with work” and then provides a free-text space where care partners can list and describe any problems they experience in each area. All data are free-text responses written on the worksheet. Not every problem recorded on the worksheet is addressed during the six sessions. The coders linked all the problems recorded on the worksheets (those addressed and unaddressed during the PST sessions) to the ICF.
Linking Concepts to the ICF
Coders identified meaningful concepts in each participant’s free-text entry on the worksheet before the independent linking process. A meaningful concept was defined as a single health aspect or an environmental factor with the potential to affect health status (Offenbächer et al., 2007). The meaning of each concept was determined on the basis of the refined ICF linking rules endorsed by WHO (Cieza et al., 2016), and the intent and structure of the problem worksheet were used to contextualize the nature of each concept. An expert ICF coder (Candice L. Osborne) linked concepts to the ICF at the most specific level possible. Concepts considered too broad to link at the chapter level were linked at Level 1 of the ICF taxonomy (see Cieza et al., 2016, for the list of linking rules).
The ICF is composed of five components: body structures (s), body functions (b), activities and participation (d), environmental factors (e), and personal factors (pf). The components, except for personal factors, are divided into chapters, which are further classified into categories. Some categories contain subcategories, and some subcategories are further dissected into third- and fourth-level subcategories. Categories become more detailed with each descending level. Per Cieza et al.’s (2016) standardized linking instructions, concepts considered too vague or general for linking are linked at a broader ICF level, coded at the category level as “unspecified” or coded as “not defined (nd).” All health conditions or diagnoses were labeled as “not covered—health conditions (nc–hc)” because they are considered linked to the ICF’s partner document, the International Classification of Diseases (ICD).
Two examples of care partner entries on the PST worksheet are as follows: (1) “[I] have additional responsibilities since the tragedy of my husband” and (2) “[I have] problems staying asleep.” Each entry contains one meaningful concept: (1) additional responsibilities and (2) staying asleep. The following are examples of the ICF linking process. “Additional responsibilities” is categorized under the activities and participation (d) component and falls under Chapter 2 (d2), “General Tasks and Demands.” It can be further classified into the category of undertaking multiple tasks (d220). Because the concept contains too little information to know whether the participant is referring to carrying out tasks, completing tasks, or undertaking tasks independently or in a group, the concept is linked as undertaking multiple tasks–unspecified (d2209). Concept 2, staying asleep, falls under the domain body functions (b); Chapter 1 (b1), “Mental functions”; category, sleep functions (b134); subcategory, maintenance of sleep (b1342). The final code is b1342, maintenance of sleep.
Reliability
To establish the interrater reliability of the linking process on the basis of the most current version of the standardized ICF linking rules, a second coder (Shannon B. Juengst) linked a random 25% of the meaningful concepts. The level of agreement between Coder 1 (Osborne) and Coder 2 (Juengst) was established using percentage agreement and the κ statistic. A κ coefficient greater than .61 is considered good agreement (Brennan & Silman, 1992). Codes that differed between the two raters after independent coding were then discussed, and a final code assignment was made upon consensus.
Results
Nine care partners completed the first PST session and the problem worksheet in the parent study. Six of the care partners were White, non-Hispanic; 2 were White, Hispanic; and 1 was African American. All the care partners had known their care recipient for >10 yr, and 5 lived with their care recipient. Four of the care recipients were people with stroke, 1 had a TBI, 1 had an SCI, and 3 had a burn injury. Two of the 9 care partners were men. Two care partners were parents of the care recipients, 3 were spouses, 2 were children, 1 was a sibling, and 1 was another relative.
The care partners reported a total of 64 problems, which included a total of 72 meaningful concepts. Ninety percent of the concepts were linkable to the ICF. Concepts were linked to 13 of 30 ICF chapters. Reliability assessment yielded a κ coefficient of .75, indicating good interrater reliability of the coding process. Coders disagreed on a code twice (11%). The coding discrepancies were resolved through discussion. Seven concepts (10%) were not linkable to the ICF—3 were considered health conditions that can be coded by the ICD and were therefore coded as nc–hc, and 4 were considered too vague to link to the ICF and were coded as nd.
Body Functions Component
Body functions are the “physiological functions of body systems (including psychological functions)” (WHO, 2001, p. 10). Of the 72 meaningful concepts, 22 (31%) were linked to the body functions component, the second most commonly linked component after the activities and participation component. All of the body functions concepts were linked to five mental functions categories in Chapter 1, “Mental Functions” (Figure 1): thought functions (b160), emotional functions (b152), sleep functions (b134), energy and drive functions (b130), and temperament and personality functions (b126). The majority of these concepts were linked to subcategories of emotional functions. One concept, sadness, was linked to the broader emotional functions category, 1 concept was linked to the range of emotions subcategory (b1522), 2 concepts were linked to the regulation of emotions subcategory (b1521), and 8 concepts were linked to the emotional functions–other specified subcategory (b1528). These concepts related to stress, frustration, boredom, guilt, and anxiety. The concept of dissatisfaction was linked to emotional functions–unspecified (b1529). The remaining eight body functions chapters were not linked to any care partner–reported problems.

Body functions representation by chapter.
Body Structure Component
Body structures are defined by the ICF as “anatomical parts of the body such as organs, limbs, and their components” (WHO, 2001, p. 10). No meaningful concepts were linked to the body structures component. However, some participants reported problems regarding health conditions that include specific body structure deficits, such as scoliosis and diabetes. These conditions were coded as nc–hc in accordance with the revised standardized linking rules.
Activities and Participation Component
Thirty-four concepts (47%) were linked to the activities and participation component, making it the most frequently linked component. Eight of the nine activities and participation chapters were linked to care partner–reported meaningful concepts (Figure 2). Chapter 1, “Learning and Applying Knowledge,” was the only chapter not linked to any care partner problem. Chapter 8, “Major Life Areas,” was the most frequently linked chapter; areas included finances (d870), employment (d850), and school (d820). Chapter 5, “Self-Care”; Chapter 6, “Domestic Life”; and Chapter 7, “Interpersonal Interactions and Relationships” were the next most frequently linked. Self-care areas included managing health (d570) and managing diet and fitness (d5701). Domestic life areas included assisting others–other specified: finances and establishing resources (d669), assisting others in health maintenance (d6605), and preparing meals (d630). Interpersonal interactions and relationships included interpersonal interactions and relationships–other specified: expectations (d789), regulating behaviors within interactions (d7202), and parent–child relationship (d7600). Chapter 2, “General Tasks and Demands”; Chapter 3, “Communication”; Chapter 4, “Mobility”; and Chapter 9, “Community, Social, and Civic Life” were also linked.
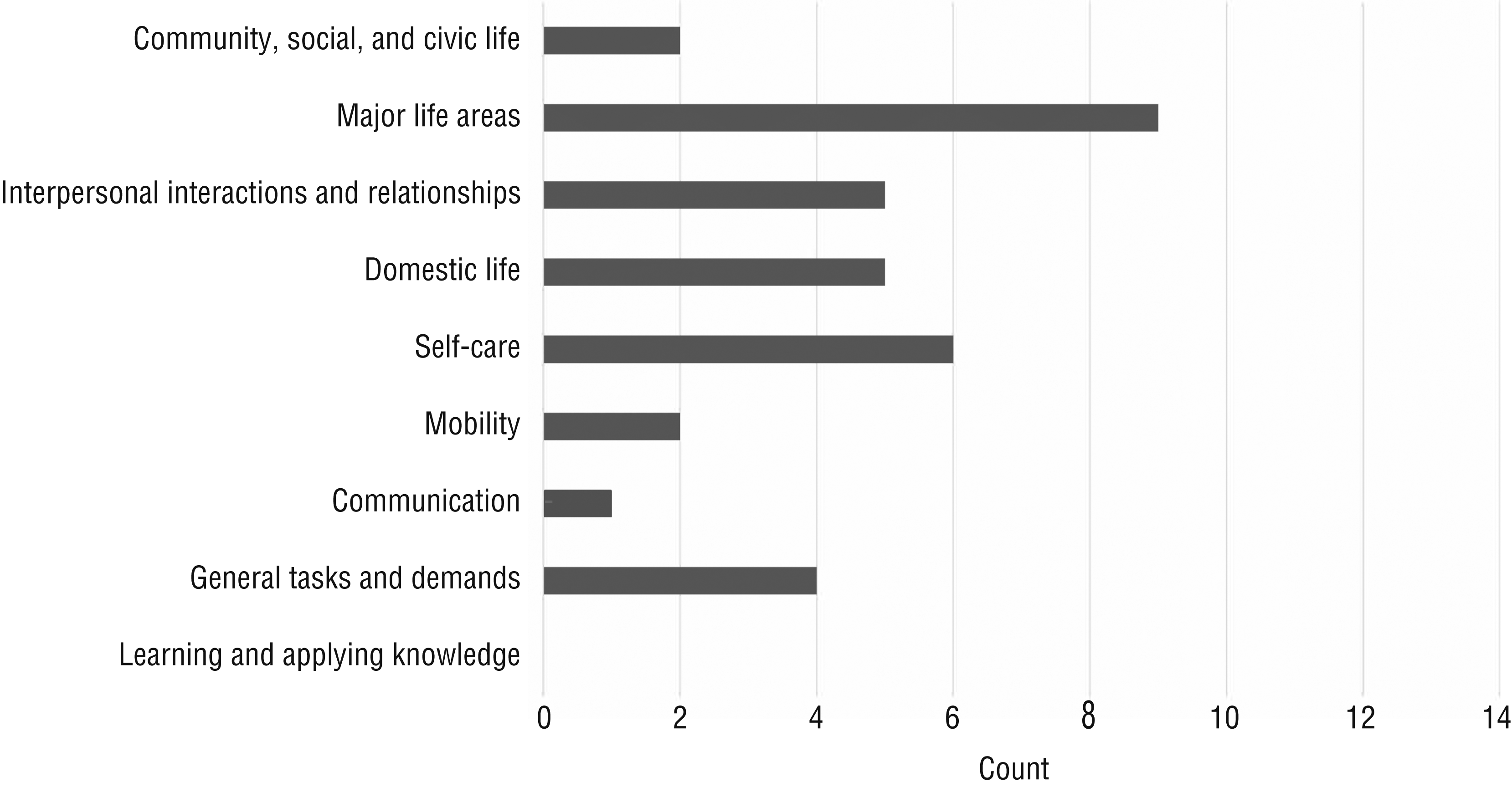
Activities and participation representation by chapter.
Environmental Factors Component
Nine concepts (13%) were linked to the environmental factors component. Four of five environmental factors chapters were linked (Figure 3). Concepts were most frequently linked to Chapter 3, “Support and Relationships”; areas included support and relationships–unspecified: help at work (e399), extended and immediate family (e310), and friend (e320). The next most frequently linked chapter was Chapter 1, “Products and Technology”; these concepts all related to financial assets (e1650). One concept was linked to Chapter 4, “Attitudes,” and one was linked to Chapter 5, “Services, Systems, and Policies.” No concepts were linked to Chapter 2, “Natural Environment and Human-Made Changes to the Environment.”
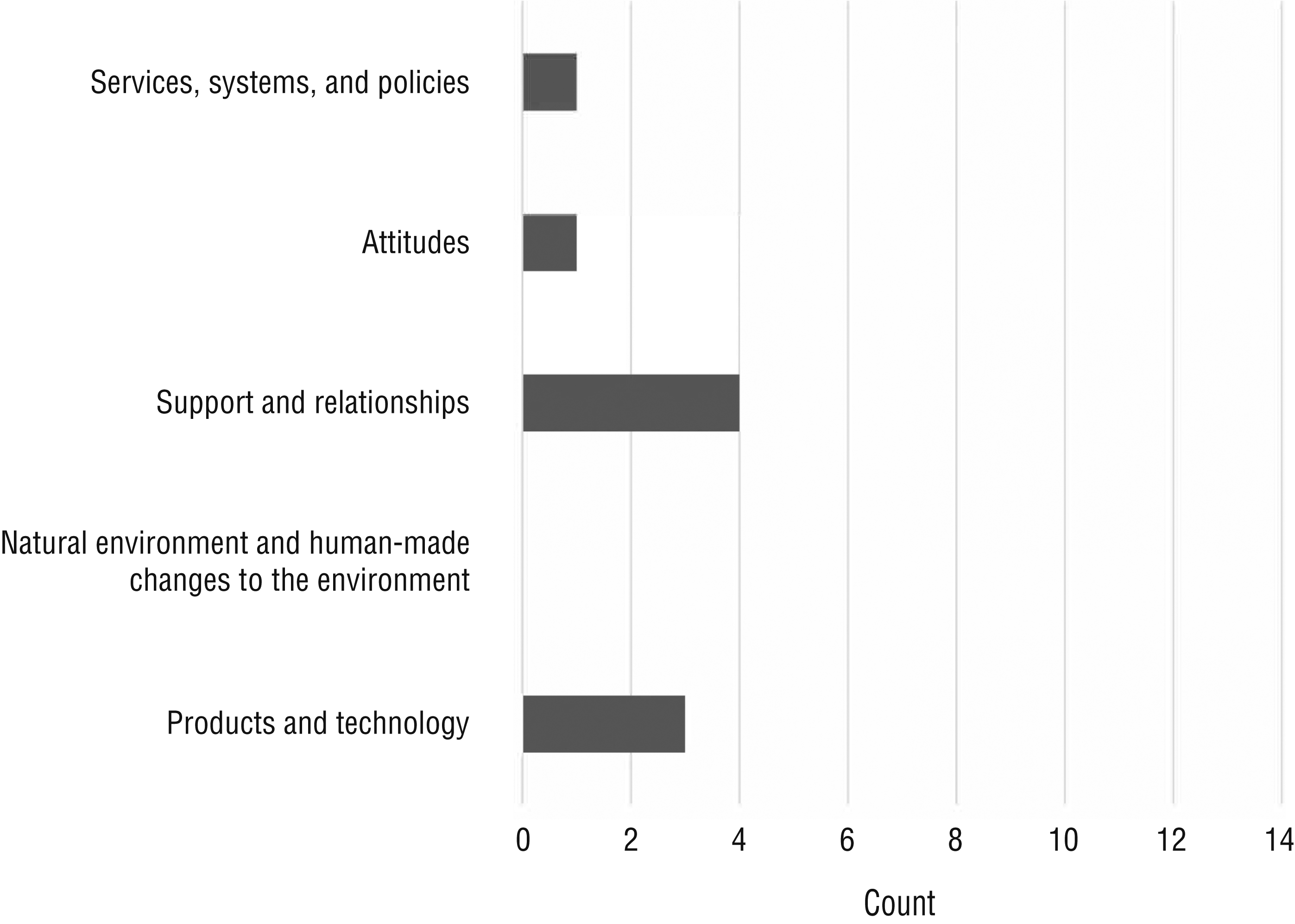
Environmental factors representation by chapter.
Discussion
The epidemiology of care partner burden has been broadly characterized by demographic, clinical, psychosocial, and contextual risk factors (Adelman et al., 2014), and evidence suggests that burden is largely predicted by the extent to which care partners’ perceived needs are met (Lutz et al., 2011). Perceived needs during the acute phase after traumatic injury or stroke include clear explanations of the condition, realistic expectations and prognosis, resources (e.g., services, financial planning), emotional support, normalizing reactions, and constructive coping strategies (Kolakowsky-Hayner et al., 2001; Luker et al., 2017; Lutz et al., 2011; Phillips et al., 2007). After discharge, care partners report a need for information about lifetime management planning; community integration; management of cognitive, behavioral, and emotional issues; and access to community resources (Lutz et al., 2011; Murphy & Carmine, 2012; Phillips et al., 2007). The findings from this study support the existing evidence, which is a broad understanding of the overarching areas of care partner concerns during the early stages of recovery. This study offers unique insight by providing a more granular examination of the lived experience of care partners through the mapping of meaningful concepts to a comprehensive taxonomy of functioning, disability, and health.
Care partners in this study most commonly reported problems in seven areas:
Emotional function: Participants reported problems related to feelings of stress, anxiety, frustration, anger, sadness, and guilt. Some reported symptoms of emotional dysfunction, such as losing their temper, disinterest in doing things, and lack of focus.
Major life areas: Many reported problems with finances, such as managing life with less income, paying medical bills, maintaining insurance, managing finances for a loved one, and lack of knowledge about how to manage finances. Some reported problems with work, specifically finding time to work or feeling unsupported at work.
Self-care: Many reported a lack of time to exercise, poor nutritional habits, and decreased ability to manage their own health conditions, such as back pain and diabetes.
Domestic life: Participants reported lacking time to prepare meals and feeling overwhelmed with caregiving tasks, such as coordinating medical appointments, searching for resources, coordinating home health, and preparing for the patient’s transition home.
Interpersonal interactions and relationships: Participants reported decreased time with their children and changes in the dynamics of their relationship with the care recipient, specifically communication and new role expectations.
Sleep functions: Some reported trouble going to sleep and staying asleep.
Support and relationships: One participant reported a lack of support at work, and another reported difficulty asking for and accepting assistance from others.
These findings suggest that care partners’ problems early in the rehabilitation process are complex and interrelated. They both affect and are affected by body functions, activities and participation, environmental factors, and their ability to manage their own health conditions.
A literature review of measures used to assess stress and physical health among caregivers of stroke survivors (Saban et al., 2010) found little consistency between studies regarding measurements used and variables assessed. A systematic approach to understanding care partner needs is necessary to develop interventions to address those needs early in the rehabilitation process (Saban et al., 2010). We demonstrated that the universal language of the ICF framework can be used to characterize care partner needs. With an understanding of these needs, the ICF may also afford a systematic approach to care partner assessment and intervention development, as it has for patients with various diagnoses. This systematic approach decreases data-gathering inconsistencies, resulting in improved patient and care partner outcomes (Cieza et al., 2016).
Limitations
A first limitation is that one coder linked all concepts to the ICF, and a second linked 25% of randomly selected concepts to determine reliability. Although this is a widely accepted practice, one coder linking only 25% of concepts may potentially bias the results toward the main coder’s linking. Second, because this study was conducted retrospectively, we were unable to discuss or clarify the meaningful concepts expressed on the worksheets. Therefore, nuances may have been lost to the coding process. The ICF could provide a foundation for the future research and development of interventions designed to meet the needs of care partners during the predischarge rehabilitation process.
Implications for Occupational Therapy Practice
The results of this study have the following implications for occupational therapy practice:
The ICF can be used to examine care partner experiences and may therefore serve as a tool to determine specific care partner needs.
Care partners experience myriad problems after a sudden-onset event, before the care recipient is discharged from the hospital. Health care providers may improve clinical practice through early care partner intervention implementation that is tailored to meet the needs of each care partner.
Conclusion
A future study with a larger and more diverse sample size will provide more insight into the nature of the problems care partners face early after sudden-onset conditions. With an enhanced understanding of these problems, effective self-management interventions can be tailored to meet care partner needs in the future.